Hepatobiliary Trauma: Bilious Attack
Yon-Cheong Wong1, Li-Jen Wang2, and Cheng-Hsien Wu3
1Tucheng New Taipei Municipal Hospital, Chang Gung Medical Foundation, New Taipei City, Taiwan, 2Medical Imaging and Intervention, Chang Gung Memorial Hospital, Gueishan, Taoyuan, Taiwan, 3Chang Gung Memorial Hospital, Gueishan, Taoyuan, Taiwan
1Tucheng New Taipei Municipal Hospital, Chang Gung Medical Foundation, New Taipei City, Taiwan, 2Medical Imaging and Intervention, Chang Gung Memorial Hospital, Gueishan, Taoyuan, Taiwan, 3Chang Gung Memorial Hospital, Gueishan, Taoyuan, Taiwan
Synopsis
Keywords: Body: Liver, Image acquisition: Visualization, Education Committee: Clinical MRI
Contrast-enhanced magnetic resonance cholangiography (CEMRC) utilizing gadoxetic acid disodium, a gadolinium-based MRI contrast agent, where approximately 50% is excreted by hepatocytes, proves advantageous in evaluating the biliary tree. Research has indicated that CEMRC not only detects post-traumatic bile leaks but also aids in characterizing their morphology. However, the duration for image acquisition can vary significantly, ranging from 20 to 180 minutes. In this presentation, the speaker will discuss the experience at Chang Gung Memorial Hospital regarding optimal CEMRC acquisition times, the feasibility of bile leak detection, and the characterization and significance of various types of bile leaks.Liver
cysts, liquefaction of liver hematoma, liver abscesses, and bile leaks all
manifest as fluid signals on magnetic resonance imaging (MRI) across all pulse
sequences. These fluid collections within the liver pose a challenge in
differentiation from bile leaks due to their shared property of long
T2-relaxation, rendering them hyperintense on T2-weighted images. Even
conventional magnetic resonance cholangiography struggles to confidently
delineate them. However, employing gadoxetic acid disodium as a contrast agent,
which about 50% is excreted by hepatocytes, enables contrast-enhanced magnetic
cholangiography (CEMRC) to readily identify bile through T1-shortening effects.
Studies have shown that biliary tree opacification can be discerned on CEMRC
acquired approximately 20 minutes post-administration of the
hepatocyte-specific contrast agent. However, the optimal acquisition time for
CEMRC using Gd-EOB-DTPA among trauma patients remains unexplored. This study
aims to determine the optimal acquisition time to expedite examination for
trauma patients.
In this
retrospective analysis of prospectively collected CEMRC data approved by the
institutional review board, informed consent was obtained from participants.
Over a 2.5-year period, 22 patients (17 men, 5 women) with a median age of 24.5
years were included. The study assessed whether non-invasive CEMRC using
gadoxetic acid disodium could detect traumatic bile leaks. Three radiologists
independently graded biliary tree visualization and bile leak detection on
CEMRC acquired at 10, 20, 30, and 90-minute time points using a 5-point Likert
scale, with interrater reliability assessed by the Intraclass Correlation
Coefficient (ICC).
Of the
22 CEMRC scans, 15 revealed bile leaks (8 expanding, 7 contained). Optimal
biliary tree visualization was observed at the 90-minute acquisition mark
(score 4.30), with excellent interrater reliability (ICC = 0.930). The accuracy
of post-traumatic bile leak detection, measured by the area under receiver
operating characteristic curves (AUROC), peaked at 90 minutes, with AUROC
values of 0.824 (p=0.017), 0.914 (p=0.002), and 0.929 (p=0.002) for the three
radiologists, respectively, and an ICC of 0.816.
In
conclusion, CEMRC effectively detects and characterizes bile leaks following
major blunt liver trauma. Notably, a high incidence of biliary injuries was
associated with active liver hemorrhage on arrival CT scans (92.3%).
Furthermore, angioembolization, often employed to manage active arterial
hemorrhage, was found to be associated with bile leaks (86.7%), likely due to
compromised vascular supply to bile duct walls. Severe lacerations from major
liver trauma may not only injure hepatic arteries but also disrupt bile ducts
and portal veins. This local epithelial perfusion defect exacerbated by
angioembolization not only hampers the healing process at the site of biliary
injuries but also predisposes to delayed bile leaks. Expanding bile leaks (type
II) necessitate more aggressive treatment than contained leaks (type I), with
higher levels of total serum bilirubin and catheter drainage observed in type
II cases. This underscores the importance of prompt and accurate detection of
bile leaks to optimize patient management and outcomes following blunt liver
trauma.
Acknowledgements
This study was supported by the Chang Gung Medical Foundation Research Project Grant (CMRPG3B0521).References
- Wong, Y. C., Wang, L. J., Wu, C. H. et al. Detection and characterization of traumatic bile leaks using Gd-EOB-DTPA enhanced magnetic resonance cholangiography. Scientific reports 8:14612, DOI:10.1038/s41598-018-32976-0 (2018).
- Dabbs, D. N., Stein, D. M. & Scalea, T. M. Major hepatic necrosis: a common complication after angioembolization for treatment of high-grade liver injuries. The Journal of trauma 66, 621-627; discussion 627–629 (2009).
- Yuan, K. C. et al. Screening and management of major bile leak after blunt liver trauma: a retrospective single center study. Scandinavian journal of trauma, resuscitation and emergency medicine 22, 26, https://doi.org/10.1186/1757-7241-22-26 (2014).
- Fang, J. F. et al. Classification and treatment of pooling of contrast material on computed tomographic scan of blunt hepatic trauma. Journal of Trauma-Injury Infection & Critical Care 49, 1083–1088 (2000).
- Sharma, B. C., Mishra, S. R., Kumar, R. & Sarin, S. K. Endoscopic management of bile leaks after blunt abdominal trauma. Journal of gastroenterology and hepatology 24, 757–761 (2009).
- Bala, M. et al. Complications of high grade liver injuries: management and outcome with focus on bile leaks. Scandinavian journal of trauma, resuscitation and emergency medicine 20, 20, https://doi.org/10.1186/1757-7241-20-20 (2012).
- Kantarci, M. et al. Non-invasive detection of biliary leaks using Gd-EOB-DTPA-enhanced MR cholangiography: comparison with T2-weighted MR cholangiography. European radiology 23, 2713–2722, https://doi.org/10.1007/s00330-013-2880-4 (2013).
- Cieszanowski, A. et al. Detection of active bile leak with Gd-EOB-DTPA enhanced MR cholangiography: comparison of 20–25 min delayed and 60–180 min delayed images. European journal of radiology 82, 2176–2182, https://doi.org/10.1016/j.ejrad.2013.08.021 (2013).
- Lee, Y. H. et al. Predictive factors for early failure of transarterial embolization in blunt hepatic injury patients. Clinical radiology 69, e505–511, https://doi.org/10.1016/j.crad.2014.08.013 (2014).
Figures
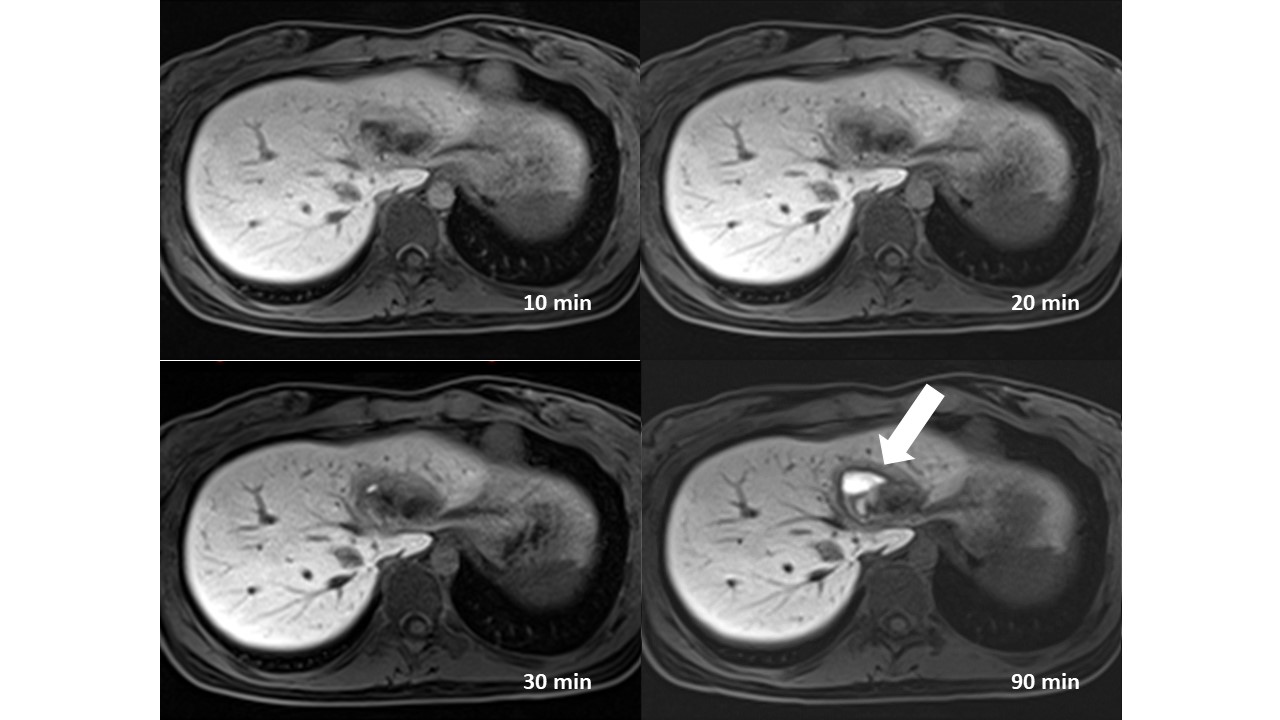
Figure
1. This is a patient with grade III liver injury. Her CEMRC shows a type I bile
leak which is most apparent at a 90-minutes acquisition image (arrow).
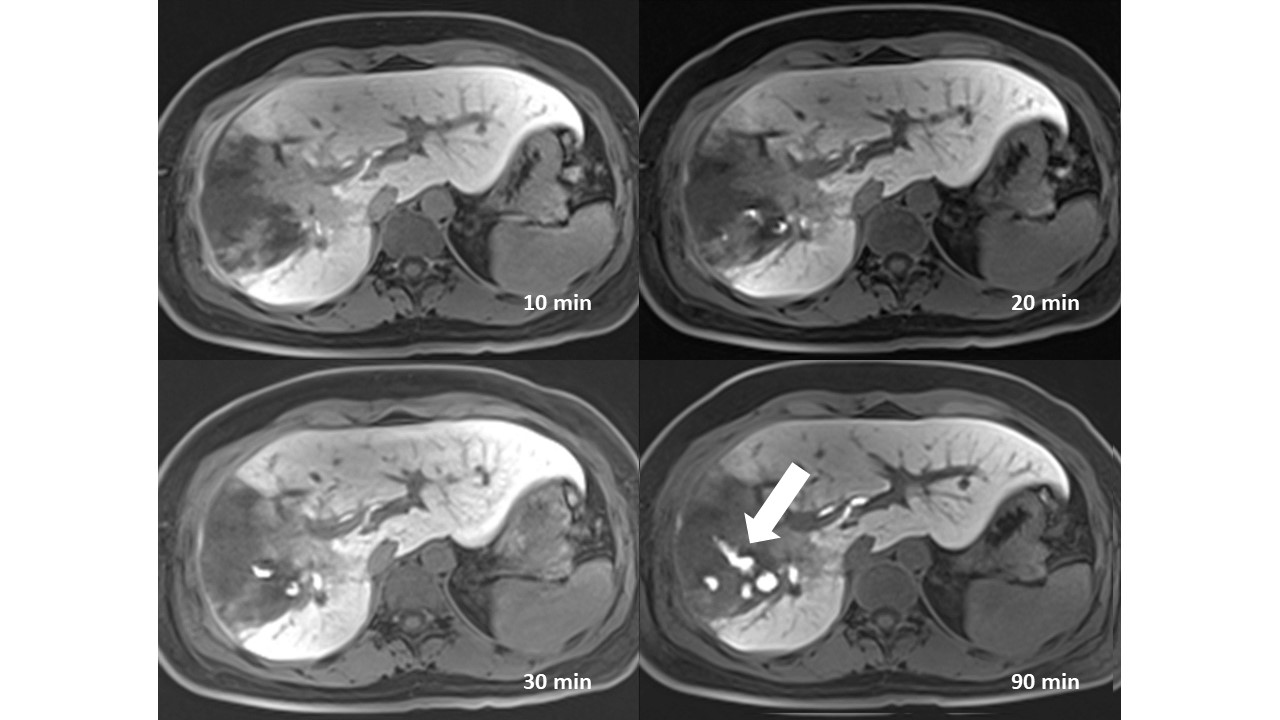
Figure
2. This is a patient with grade III liver injury. Her CEMRC shows a type II
bile leak which is most apparent at a 90-minutes acquisition image (arrow).
Coronal plane obtained immediately after the 90-minutes acquisition shows
T1-shortening bile at right subphrenic space confirming it is a type II bile
leak (not shown).