Basics of Abdominal Trauma: Mechanisms & Acute/Chronic Sequelae of Traumatic Injury, Including Chest, Abdomen & Pelvis
1Tohoku University, Sendai, Japan
Synopsis
Keywords: Cardiovascular: Angiography, Body: Urogenital, Body: Body
In acute trauma cases, CT is preferred for its accessibility and speed, though concerns arise over radiation and contrast agents. MR imaging supplements CT, particularly in assessing traumatic lesions. For chest trauma, MR aids in blunt thoracic aortic injury assessment, guiding management decisions. It's also useful for chest wall fracture assessment, revealing occult rib fractures. In abdominal trauma, MRCP helps detect pancreatic and biliary duct injuries; Gd-EOB-DTPA also aids in bile duct injury evaluation. MR imaging is valuable in pelvic injuries due to its excellent tissue contrast. Considering radiation exposure, MR imaging would be preferred in pediatrics and pregnant patients.Chest:
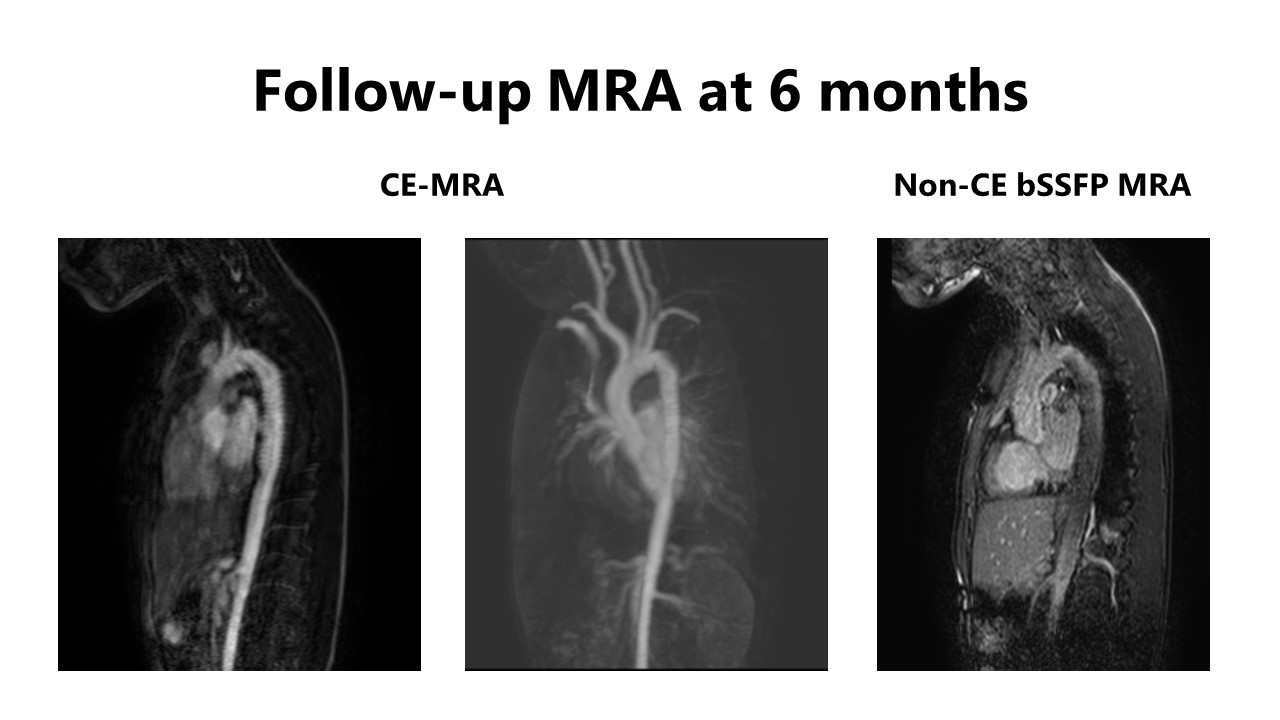
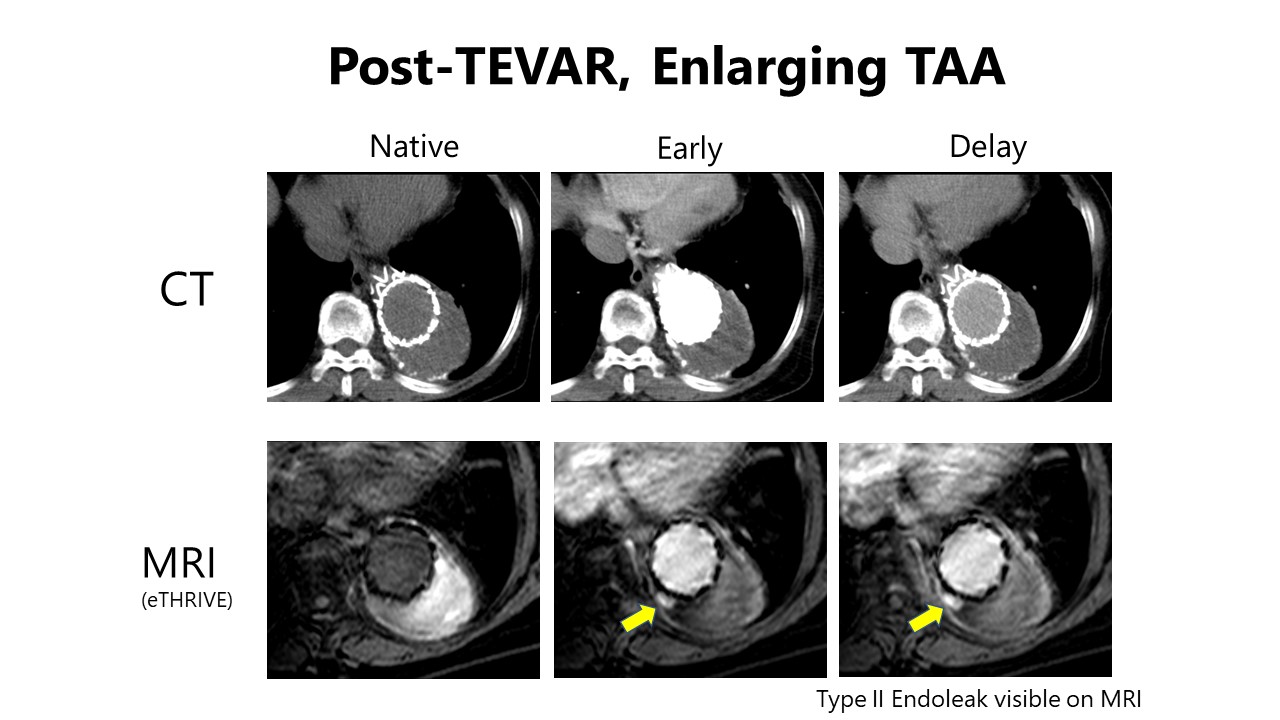
Blunt thoracic aortic injury (BTAI) is a rare but lethal entity, most commonly occurring in motor vehicle collisions(6). While contrast-enhanced CT is typically utilized for assessment of the aorta and other organs, MR imaging examinations can be beneficial when the use of iodinated contrast agents is challenging. The management strategies for BTAI include medical therapy, thoracic endovascular aortic repair (TEVAR), and surgical repair. Especially with device development, TEVAR has emerged as the dominant therapy for BTAI(6). MR imaging can be used for the follow-up examination after interventions; especially patients treated by TEVAR require long-term follow-up, raising concerns about radiation exposure on CT(7). Depending on the materials of the stent graft, endoleak evaluation after TEVAR is feasible. Furthermore, functional analysis (flow analysis) of the thoracic aorta may add prognostic information after TEVAR(8).
Chest wall fractures can commonly occur; radiographs are usually the first choice imaging modality used in suspected chest wall fractures. However, MR imaging may provide a potential complementary tool for the assessment of chest wall fractures. Early MR imaging after work-related chest trauma can identify the source of pain, mainly radiographically occult rib fractures(9).
Abdomen:
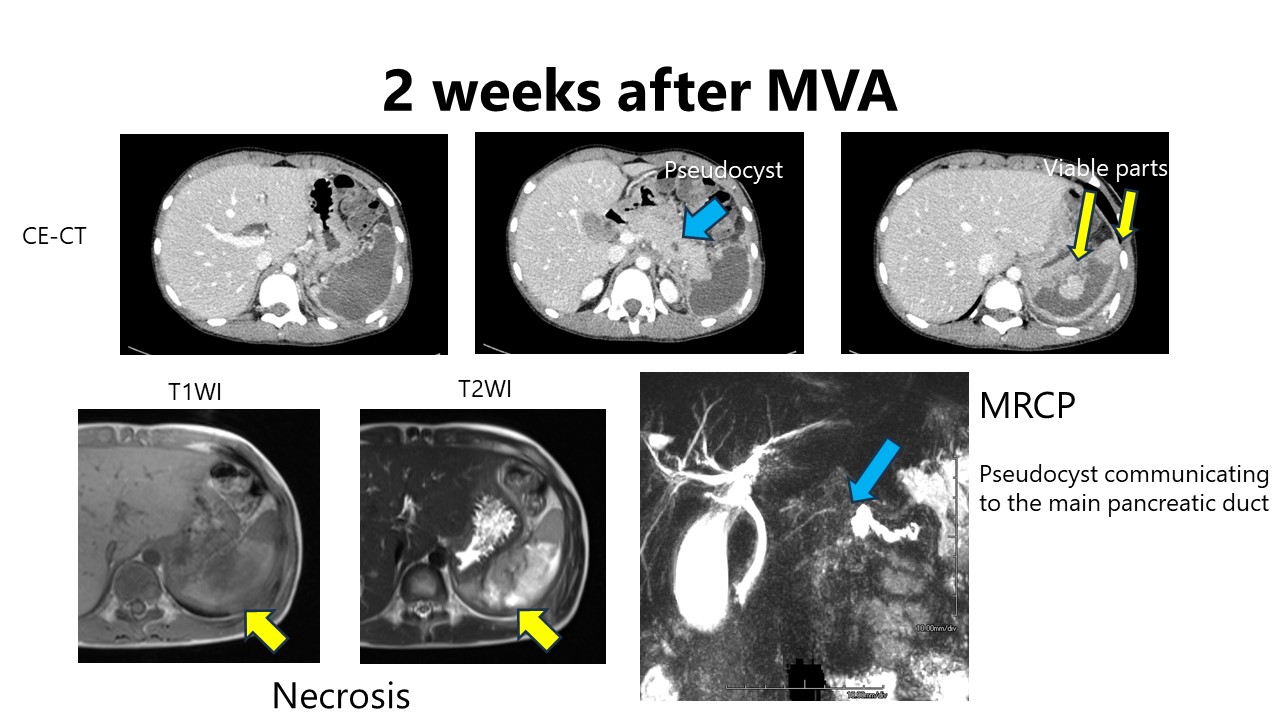
In abdominal trauma cases, the evaluation of pancreatic and biliary duct injuries via magnetic resonance cholangiopancreatography (MRCP) can provide valuable information for determining treatment plans(4, 10). In cases with traumatic pancreatic injury, CT may be limited for the evaluation of main pancreatic duct. MRCP allows for detection of pseudocysts communicating with the main pancreatic duct. Gadolinium ethoxybenzyl (Gd-EOB-DTPA) is an MR contrast agent that is approximately 50% taken up by hepatocytes and excreted by the biliary system(11). Although the contrast agent is generally applied to evaluate primary and metastatic liver tumors, it can be also utilized for evaluating bile duct injuries. Gd-EOB-DTPA-MRCP enables adequate detection and localization of bile leakages in postoperative and post-traumatic patients(12).
MR imaging also works for evaluation of indetermined findings on CT by utilizing its superior soft tissue contrast, which include mimickers in the spleen and liver.
Pelvic Region:
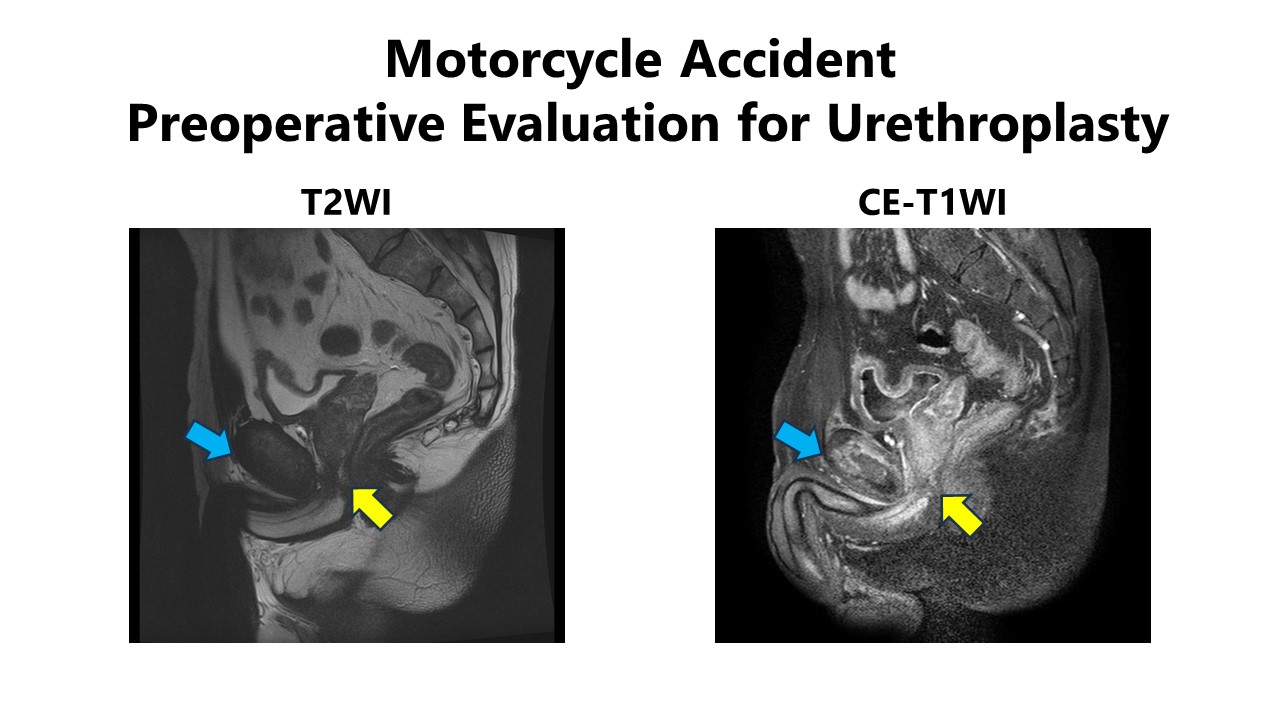
Detailed lesion evaluations utilizing excellent tissue contrast are also achievable in pelvic injuries. Role of MR imaging in the management of male urethral injury with or without pelvic fracture has been reported(13). MR imaging provides detailed information on the post-traumatic anatomy, including the urethral gap length and displacement of the prostate. MR imaging is recommended as a second-line imaging examination in cases of scrotal trauma and non-diagnostic ultrasound findings(14)
Others:
MR imaging may be employed for a thorough investigation of incidental findings, usually detected by other imaging modalities, in trauma cases. Cases of chronic expanding hematoma will also be demonstrated.
This presentation aims to outline the imaging workflow in trauma cases, provide examples and case presentations illustrating the indications for MR imaging, thereby introducing the role of MR imaging in trauma care.
Acknowledgements
No acknowledgement found.References
1. Linsenmaier U, Krötz M, Häuser H, et al.: Whole-body computed tomography in polytrauma: techniques and management. Eur Radiol 2002; 12:1728–1740.
2. Körner M, Krötz MM, Degenhart C, Pfeifer K-J, Reiser MF, Linsenmaier U: Current Role of Emergency US in Patients with Major Trauma. RadioGraphics 2008; 28:225–242.
3. Heller MT, Oto A, Allen BC, et al.: ACR Appropriateness Criteria® Penetrating Trauma–Lower Abdomen and Pelvis. J Am Coll Radiol 2019; 16:S392–S398. [ACR Appropriateness Criteria®–November 2019]
4. Rajput MZ, Mellnick VM: The Role of Magnetic Resonance in Evaluating Abdominopelvic Trauma - Part 1: Pancreatic and Hepatobiliary Injuries. Can Assoc Radiol J 2022; 73:680–688.
5. Rajput MZ, Mellnick VM: The Role of Magnetic Resonance in Evaluating Abdominopelvic Trauma - Part 2: Trauma in Pregnancy, Vascular, and Genitourinary Injuries. Can Assoc Radiol J 2022; 73:689–696.
6. Akhmerov A, DuBose J, Azizzadeh A: Blunt Thoracic Aortic Injury: Current Therapies, Outcomes, and Challenges. Ann Vasc Dis 2019; 12:1–5.
7. Fattori R, Celletti F, Descovich B, et al.: Evolution of post-traumatic aortic aneurysm in the subacute phase: magnetic resonance imaging follow-up as a support of the surgical timing. Eur J Cardio-Thorac Surg Off J Eur Assoc Cardio-Thorac Surg 1998; 13:582–586; discussion 586-587.
8. Oberhuber A, Schabhasian D, Kohlschmitt R, Rottbauer W, Orend K-H, Rasche V: The bird beak configuration has no adverse effect in a magnetic resonance functional analysis of thoracic stent grafts after traumatic aortic transection. J Vasc Surg 2015; 61:365–373.
9. Capelastegui A, Oca R, Iglesias G, Larena JA: MRI in suspected chest wall fractures: diagnostic value in work-related chest blunt trauma. Skeletal Radiol 2024; 53:275–283.
10. Ibrahim A, Wales PW, Aquino MR, Chavhan GB: CT and MRI findings in pancreatic trauma in children and correlation with outcome. Pediatr Radiol 2020; 50:943–952.
11. Bollow M, Taupitz M, Hamm B, Staks T, Wolf KJ, Weinmann HJ: Gadolinium-ethoxybenzyl-DTPA as a hepatobiliary contrast agent for use in MR cholangiography: results of an in vivo phase-I clinical evaluation. Eur Radiol 1997; 7:126–132.
12. Marth AA, Auer TA, Walter-Rittel TC, et al.: Gd-EOB-DTPA-MRCP to localize bile leakage after liver trauma and surgery: impact on treatment and outcome. Eur Radiol 2023; 33:5933–5942.
13. Horiguchi A, Edo H, Shinchi M, et al.: Role of magnetic resonance imaging in the management of male pelvic fracture urethral injury. Int J Urol 2022; 29:919–929.
Figures