Cardiac MRI During Exercise
1Beth Israel Deaconess Medical Center, Boston, MA, United States
Synopsis
Keywords: Cardiovascular: Cardiovascular
This educational talk presents an overview of cardiac MRI during exercise, highlighting its challenges and recent advancements. We explore technical specifications for optimal imaging during exercise and advancements in Ex-CMR sequences and image reconstruction techniques. The aim is to shed light on the complexities of capturing accurate cardiac images during physical stress and the potential of these techniques in diagnosing and managing cardiovascular diseases.Introduction
Exercise cardiac magnetic resonance (Ex-CMR) imaging is a stress test with promising clinical value in the management of patients with cardiovascular disease (1, 2). From an imaging perspective, Ex-CMR cine and perfusion combine the capabilities of echocardiography and nuclear stress tests. Tagging, 4D flow, spectroscopy, and other CMR sequences may also provide novel imaging stress biomarkers in specific patient populations (3, 4). From a more physiological perspective, exercise stress has many advantages compared to pharmacological stress. In this educational talk, we will discuss 1) how exercise is done in the MRI environment, 2) the “ideal” technical specifications for Ex-CMR, and 3) recent advances in sequences and image reconstruction.Exercise in the MRI Environment
Exercise is accomplished with commercial or custom equipment inside or outside the scanner bore, most commonly using a supine cycle ergometer (Fig. 1). New designs are being explored to the reduce equipment costs (5). Exercise protocols progressively increase the exercise intensity. Adequate staffing is required to monitor and “encourage” patients during exercise. Many factors influence the exercise response and its interpretation. The equipment used for exercise (e.g., supine ergometer, upright treadmill) has an impact on the baseline cardiac volumes and the maximum workload. Exercise intensity (e.g., 10W vs 20W steps) is also often tailored to each patient, and the timing of imaging (e.g., during peak stress, post-exercise) may affect the assessment of the overall response.Ideal Technical Specifications for Ex-CMR
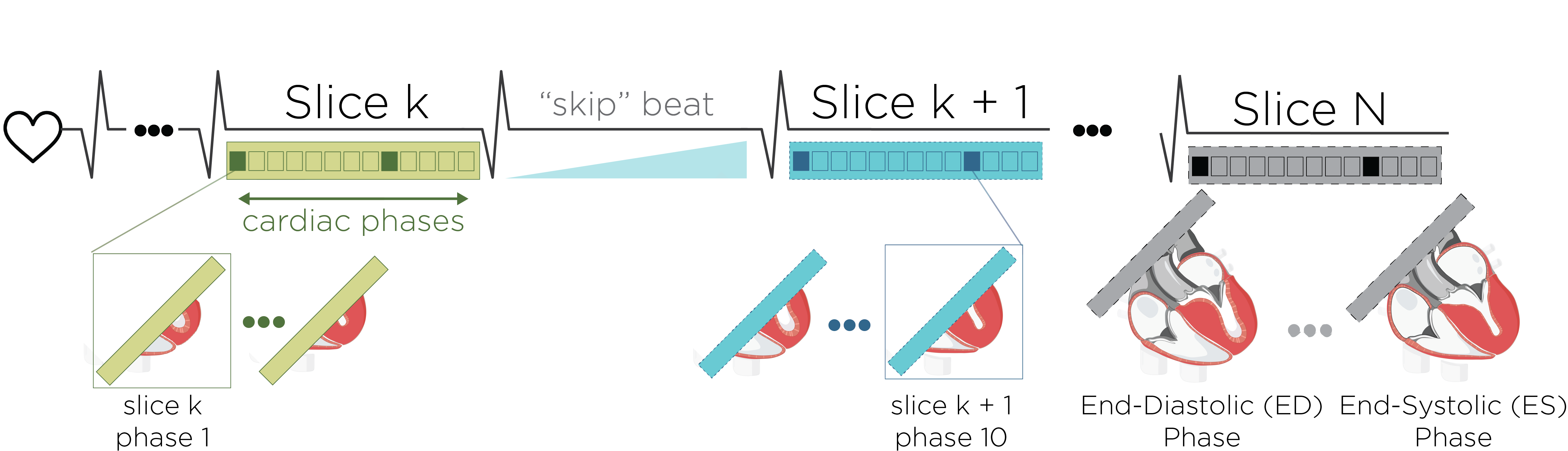
In cardiac MRI, there is a tradeoff between spatiotemporal resolution, signal-to-noise ratio (SNR), and scan time. That is, better resolution results in longer breath-holds due to the increased scan time. However, during physiological stress, breath-holding becomes challenging for patients due to fatigue. Also, electrocardiogram (ECG)-segmented imaging is unreliable due to increased patient movement and cardiorespiratory motion, which is often substantial. Thus, imaging during physiological stress should ideally be entirely free-breathing and ungated, i.e., real-time. Ex-CMR imaging protocols include dynamic sequences such as cine, flow, and tagging (Fig. 2). Subsequently, gadolinium contrast may be injected to assess stress perfusion. Because there is a tradeoff between non-contrast sequences and perfusion imaging, it is important to minimize the time between cessation of exercise and stress perfusion. Further, achieving the optimal resolution for cardiac stress imaging is only possible with use of high acceleration rates, which may compromise image quality and increase reconstruction latency. Depending on the imaging protocol, re-planning can be needed after exercise. Therefore, reconstruction latency should be minimized to avoid interfering with downstream sequences. Dynamic sequences should ideally image each slice during a single beat, allowing rapid coverage of multiple slices. However, a “skip” heartbeat is currently used to stablish steady state (Fig. 3). It has been shown that heart volumes may begin to show recovery 4 seconds after peak exercise (6), and that heart motion abnormalities can resolve sixty seconds after peak exercise (7). Therefore, regardless of whether cines images are used to quantify volumes or to detect motion abnormalities, rapid imaging is needed for accurate assessment. Scan time may be reduced at the expense of spatial or temporal resolution. However, accurate assessment of volumes and function may require a temporal resolution of less than 40 ms, and a spatial resolution of at least 2 × 2 mm2 (8). Ex-CMR flow imaging is also more susceptible to turbulent flow and might require higher temporal resolutions as well as short echo times (9). The optimal imaging parameters likely vary based on the acceptable margin of error and the anticipated response to exercise within specific patient groups, and many successful Ex-CMR clinical studies are based on a sequence with less than “ideal” resolution (10). Nevertheless, as new sequences and applications are developed, studies aimed at characterizing the impact of imaging should be welcomed.Recent Advances in Ex-CMR Sequences and Image Reconstruction
There have been many advances in Ex-CMR in the last decade to assess function (10-15), deformation (16, 17), hemodynamics, and perfusion (18-21). In cine imaging, the field has made significant advances since the early attempts to quantify heart volumes (14) and assess motion abnormalities during cardiac stress (18). Sequences with < 2 × 2 mm2 spatial resolution and < 40 ms have been reported using radial imaging with iterative reconstruction (12, 22) and with Cartesian incoherent random undersampling with compressed sensing reconstruction (13, 23). Deep learning (DL) reconstruction of radially sampled real-time data can reduce reconstruction time, enabling inline visualization of cine images in the scanner console with low latency (11). Compressed sensing was also recently combined with DL-based resolution enhancement, which resulted in a combined 15-fold acceleration rate (15). Tagging imaging could provide quantitative measures of deformation during cardiac stress, which are difficult to obtain from cine images due to respiratory motion. However, Ex-CMR tagging has mainly been mainly used with breath-holding (17). A bSSFP real-time tagging sequence was recently demonstrated for Ex-CMR using a combination of compressed sensing with DL-based resolution enhancement, which enabled 2 × 2 mm2 spatial resolution with a temporal resolution of 29 ms. (16). Interestingly, flow and tagging sequences can be combined to assess both hemodynamics and deformation during stress (17). Accelerated imaging of flow is challenging due to the reduced SNR and temporal resolution. Shared velocity encoding has been used to improve temporal resolution (24). The feasibility of 4D flow during exercise has also been demonstrated in healthy subjects (25). Ex-CMR 4D flow may be used to extract novel hemodynamic stress biomarkers such as pressure gradients and energy loss, and kinetic energy (26), which are now becoming available in commercial software. Nevertheless, 4D flow sequences suffer from low spatial resolutions and long scan times. Therefore, additional technological advances are needed. In addition, further advances are needed in dynamic imaging to improve the SNR and contrast lost due to acceleration. In both pharmacologic and exercise stress studies, static perfusion images with saturation recovery contrast are collected at different slice locations across multiple heart beats. Therefore, acceleration is used to increase spatial coverage while maintaining sufficient spatial resolution and small acquisition windows. In addition, higher acceleration rates and robust reconstruction methods are needed with exercise stress due to the signification respiratory motion. Nevertheless, despite some advances in acceleration (20), echo-planar imaging is the only sequence with demonstrated diagnostic capabilities (21). Further development in three-dimensional or multi-slice imaging could provide greater slice coverage.Acknowledgements
No acknowledgement found.References
1. Trankle CR, Canada JM, Jordan JH, Truong U, Hundley WG. Exercise Cardiovascular Magnetic Resonance: A Review. J Magn Reson Imaging 2022;55(3):720-754. doi: 10.1002/jmri.27580
2. Craven TP, Tsao CW, La Gerche A, Simonetti OP, Greenwood JP. Exercise cardiovascular magnetic resonance: development, current utility and future applications. J Cardiovasc Magn Reson 2020;22(1):65. doi: 10.1186/s12968-020-00652-w
3. Rajiah PS, Francois CJ, Leiner T. Cardiac MRI: State of the Art. Radiology 2023;307(3):e223008. doi: 10.1148/radiol.223008
4. Leiner T, Rueckert D, Suinesiaputra A, Baessler B, Nezafat R, Isgum I, Young AA. Machine learning in cardiovascular magnetic resonance: basic concepts and applications. J Cardiovasc Magn Reson 2019;21(1):61. doi: 10.1186/s12968-019-0575-y
5. He B, Chen Y, Wang L, Yang Y, Xia C, Zheng J, Gao F. Compact MR-compatible ergometer and its application in cardiac MR under exercise stress: A preliminary study. Magn Reson Med 2022;88(4):1927-1936. doi: 10.1002/mrm.29311
6. Beaudry RI, Samuel TJ, Wang J, Tucker WJ, Haykowsky MJ, Nelson MD. Exercise cardiac magnetic resonance imaging: a feasibility study and meta-analysis. Am J Physiol Regul Integr Comp Physiol 2018;315(4):R638-R645. doi: 10.1152/ajpregu.00158.2018
7. Hecht HS, DeBord L, Sotomayor N, Shaw R, Dunlap R, Ryan C. Supine bicycle stress echocardiography: peak exercise imaging is superior to postexercise imaging. J Am Soc Echocardiogr 1993;6(3 Pt 1):265-271. doi: 10.1016/s0894-7317(14)80062-x
8. Setser RM, Fischer SE, Lorenz CH. Quantification of left ventricular function with magnetic resonance images acquired in real time. J Magn Reson Imaging 2000;12(3):430-438. doi: 10.1002/1522-2586(200009)12:3<430::aid-jmri8>3.0.co;2-v
9. O'Brien KR, Myerson SG, Cowan BR, Young AA, Robson MD. Phase contrast ultrashort TE: A more reliable technique for measurement of high-velocity turbulent stenotic jets. Magn Reson Med 2009;62(3):626-636. doi: 10.1002/mrm.22051
10. La Gerche A, Claessen G, Van de Bruaene A, Pattyn N, Van Cleemput J, Gewillig M, Bogaert J, Dymarkowski S, Claus P, Heidbuchel H. Cardiac MRI: a new gold standard for ventricular volume quantification during high-intensity exercise. Circ Cardiovasc Imaging 2013;6(2):329-338. doi: 10.1161/CIRCIMAGING.112.980037
11. Morales MA, Assana S, Cai X, Chow K, Haji-Valizadeh H, Sai E, Tsao C, Matos J, Rodriguez J, Berg S, Whitehead N, Pierce P, Goddu B, Manning WJ, Nezafat R. An inline deep learning based free-breathing ECG-free cine for exercise cardiovascular magnetic resonance. J Cardiovasc Magn Reson 2022;24(1):47. doi: 10.1186/s12968-022-00879-9
12. Uecker M, Zhang S, Voit D, Karaus A, Merboldt KD, Frahm J. Real-time MRI at a resolution of 20 ms. NMR Biomed 2010;23(8):986-994. doi: 10.1002/nbm.1585
13. Lin ACW, Strugnell W, Riley R, Schmitt B, Zenge M, Schmidt M, Morris NR, Hamilton-Craig C. Higher resolution cine imaging with compressed sensing for accelerated clinical left ventricular evaluation. J Magn Reson Imaging 2017;45(6):1693-1699. doi: 10.1002/jmri.25525
14. Lurz P, Muthurangu V, Schievano S, Nordmeyer J, Bonhoeffer P, Taylor AM, Hansen MS. Feasibility and reproducibility of biventricular volumetric assessment of cardiac function during exercise using real-time radial k-t SENSE magnetic resonance imaging. J Magn Reson Imaging 2009;29(5):1062-1070. doi: 10.1002/jmri.21762
15. Yoon S, Nakamori S, Amyar A, Assana S, Cirillo J, Morales MA, Chow K, Bi X, Pierce P, Goddu B, Rodriguez J, L HN, W JM, Nezafat R. Accelerated Cardiac MRI Cine with Use of Resolution Enhancement Generative Adversarial Inline Neural Network. Radiology 2023;307(5):e222878. doi: 10.1148/radiol.222878
16. Morales MA, Yoon S, Fahmy A, Ghanbari F, Nakamori S, Rodriguez J, Yue J, Street JA, Herzka DA, Manning WJ, Nezafat R. Highly accelerated free-breathing real-time myocardial tagging for exercise cardiovascular magnetic resonance. J Cardiovasc Magn Reson 2023;25(1):56. doi: 10.1186/s12968-023-00961-w
17. Sampath S, Derbyshire JA, Ledesma-Carbayo MJ, McVeigh ER. Imaging left ventricular tissue mechanics and hemodynamics during supine bicycle exercise using a combined tagging and phase-contrast MRI pulse sequence. Magn Reson Med 2011;65(1):51-59. doi: 10.1002/mrm.22668
18. Raman SV, Dickerson JA, Jekic M, Foster EL, Pennell ML, McCarthy B, Simonetti OP. Real-time cine and myocardial perfusion with treadmill exercise stress cardiovascular magnetic resonance in patients referred for stress SPECT. J Cardiovasc Magn Reson 2010;12(1):41. doi: 10.1186/1532-429X-12-41
19. Foster EL, Arnold JW, Jekic M, Bender JA, Balasubramanian V, Thavendiranathan P, Dickerson JA, Raman SV, Simonetti OP. MR-compatible treadmill for exercise stress cardiac magnetic resonance imaging. Magn Reson Med 2012;67(3):880-889. doi: 10.1002/mrm.23059
20. Pflugi S, Roujol S, Akcakaya M, Kawaji K, Foppa M, Heydari B, Goddu B, Kissinger K, Berg S, Manning WJ, Kozerke S, Nezafat R. Accelerated cardiac MR stress perfusion with radial sampling after physical exercise with an MR-compatible supine bicycle ergometer. Magn Reson Med 2015;74(2):384-395. doi: 10.1002/mrm.25405
21. Raman SV, Dickerson JA, Mazur W, Wong TC, Schelbert EB, Min JK, Scandling D, Bartone C, Craft JT, Thavendiranathan P, Mazzaferri EL, Jr., Arnold JW, Gilkeson R, Simonetti OP. Diagnostic Performance of Treadmill Exercise Cardiac Magnetic Resonance: The Prospective, Multicenter Exercise CMR's Accuracy for Cardiovascular Stress Testing (EXACT) Trial. J Am Heart Assoc 2016;5(8). doi: 10.1161/JAHA.116.003811
22. Backhaus SJ, Lange T, George EF, Hellenkamp K, Gertz RJ, Billing M, Wachter R, Steinmetz M, Kutty S, Raaz U, Lotz J, Friede T, Uecker M, Hasenfuss G, Seidler T, Schuster A. Exercise Stress Real-Time Cardiac Magnetic Resonance Imaging for Noninvasive Characterization of Heart Failure With Preserved Ejection Fraction: The HFpEF-Stress Trial. Circulation 2021;143(15):1484-1498. doi: 10.1161/CIRCULATIONAHA.120.051542
23. Lin ACW, Seale H, Hamilton-Craig C, Morris NR, Strugnell W. Quantification of biventricular strain and assessment of ventriculo-ventricular interaction in pulmonary arterial hypertension using exercise cardiac magnetic resonance imaging and myocardial feature tracking. J Magn Reson Imaging 2019;49(5):1427-1436. doi: 10.1002/jmri.26517
24. Lin HY, Bender JA, Ding Y, Chung YC, Hinton AM, Pennell ML, Whitehead KK, Raman SV, Simonetti OP. Shared velocity encoding: a method to improve the temporal resolution of phase-contrast velocity measurements. Magn Reson Med 2012;68(3):703-710. doi: 10.1002/mrm.23273
25. Macdonald JA, Beshish AG, Corrado PA, Barton GP, Goss KN, Eldridge MW, Francois CJ, Wieben O. Feasibility of Cardiovascular Four-dimensional Flow MRI during Exercise in Healthy Participants. Radiol Cardiothorac Imaging 2020;2(3):e190033. doi: 10.1148/ryct.2020190033
26. Garcia J, Barker AJ, Markl M. The Role of Imaging of Flow Patterns by 4D Flow MRI in Aortic Stenosis. JACC Cardiovasc Imaging 2019;12(2):252-266. doi: 10.1016/j.jcmg.2018.10.034
Figures
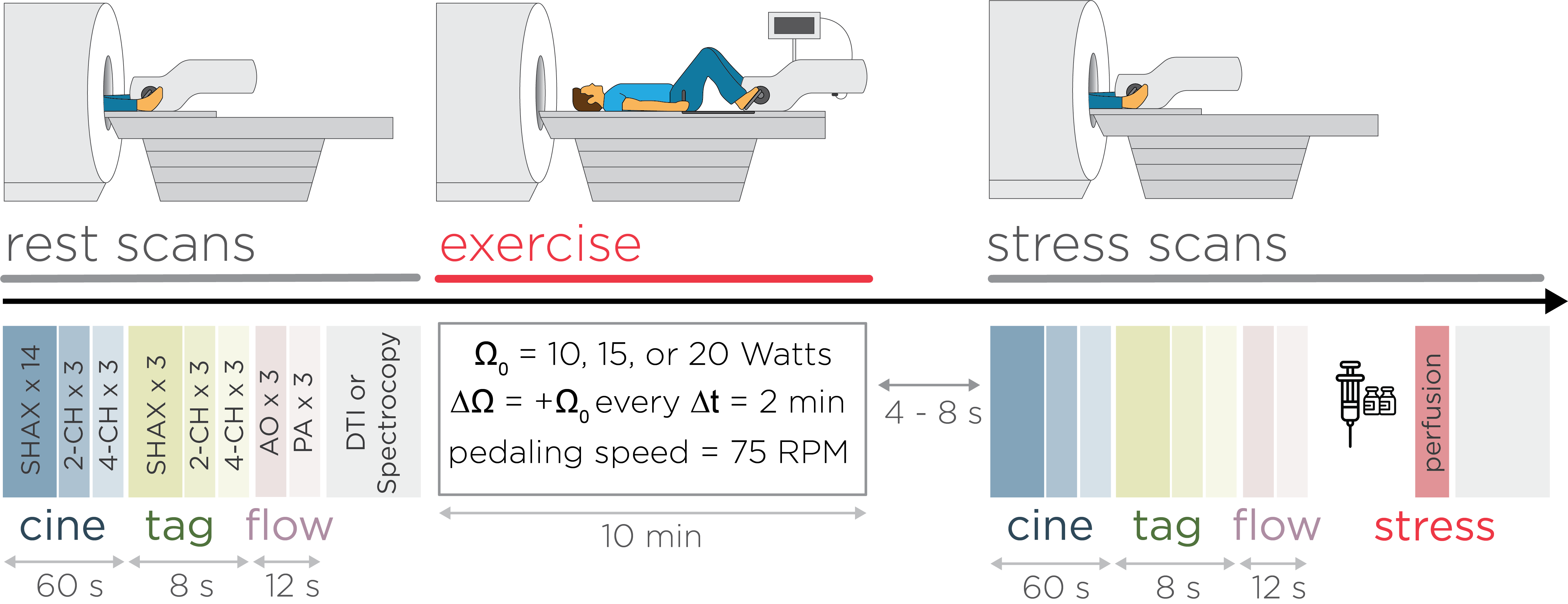
Figure 2. Example of exercise cardiac magnetic resonance (Ex-CMR) imaging protocol. Ex-CMR imaging protocols include sequences such as cine, tagging, flow, or other sequences such as spectroscopy. These sequences are used before and after/during exercise. Subsequently, gadolinium contrast may be injected to assess stress perfusion.