The Problem with PI-RADS
Yan Mee Law1
1SINGAPORE GENERAL HOSPITAL, Singapore
1SINGAPORE GENERAL HOSPITAL, Singapore
Synopsis
Keywords: Body: Urogenital, Cross-organ: Cancer, Image acquisition: Multiparametric
PI-RADS v2.1 is widely adopted by the international radiology and urology communities in risk assessment of clinically significant prostate cancer (csPCa) at multi-parametric MRI (mpMRI) in treatment naïve men. This consensus document, aimed at establishing uniformity in acquisition and interpretation of mpMRI, has been prone to performance variations. A non-negligible number of csPCa are missed at mpMRI as these lesions resemble benign lesions or possess mpMRI features that do not fit a defined PIRADS category. We discuss the limitations and controversies of PIRADS and tips and tricks that may be useful to improve the conspicuity of “MRI occult” csPCa.BACKGROUND
Prostate multiparametric MRI (mpMRI) and PIRADS play a critical role in lesion detection, biopsy guidance and staging of clinically significant prostate cancer (csPCa). A consensus document, PIRADS version 1, aimed at establishing uniform standards in acquisition and interpretation of mpMRI was first released in 2012. PIRADS version 2 was subsequently released in 2015 and refined in 2019 to PIRADS v2.1. Compared to PIRADS version 1, PIRADS v2 and subsequently v2.1 has been widely adopted by the international radiology and urology community because a single “simplified” score is assigned to each lesion based on all mpMRI sequences.LIMITATIONS OF PIRADS - MPMRI QUALITY
PIRADS assessment is primarily used for risk stratification of lesions detected on mpMRI in treatment naïve men and subsequently in guiding biopsy strategies. Accuracy in csPCa diagnosis with mpMRI and PIRADS is multifactorial including technical factors such as image quality and readers experience. Despite refinements in the updated version of PIRADS v2.1 in 2019, inter-reader and intra-reader variability in mpMRI interpretation remain a concern due to subjective definitions in assigning PIRADS categories.PIRADS grading is only as accurate as the quality of mpMRI. While PIRADs addresses the technical parameters for mpMRI acquisition, it does not address the quality of images. Factors impairing image quality include patient factors such as motion artefacts from patient movement and rectal peristalsis, presence of implants and hardware factors such as quality of MRI systems. Poor mpMRI image quality significantly impacts radiologist interpretation, accuracy of biopsy guidance and adversely affecting clinical outcome. It is important to assess mpMRI image quality as this provides invaluable insights on reliability and reproducibility of mpMRI and PIRADS in prostate cancer management.
LIMITATIONS OF PIRADS - MPMRI INTERPRETATION
Despite level 1 evidence supporting the role of mpMRI and PIRADS in clinical management of csPCa, a non-negligible number of csPCa are missed. Some of these cancers may have MRI features which overlap with benign lesions, further compounded by heterogeneous appearance of transition zone (TZ) and many missed cancers have features that do not fit the described appearances in various PIRADS categories. In addition, small volume cancers, readers experience, inconspicuity of cancers using the current PIRADS criteria are other possible reasons.Approximately 70% of prostate cancer arise in the peripheral zone (PZ), 20% in the TZ. Cancer can but rarely arise in the central zone (CZ). Analysis of CZ is challenging, even for experienced readers. Cancer arising in CZ has a higher risk of more aggressive behavior although the reason is unclear. PIRADS v2.1 is unclear on CZ assessment with no clear criteria on assigning a PIRADs category to lesions arising from the CZ.
A subjective binary approach is recommended by PIRADS v2.1 in interpreting dynamic contrast MRI (DCE MRI) which may be confusing for novice readers. In the current format, role of DCE MRI is primarily for upgrading of equivocal peripheral zone lesions that receive a PIRADS score of 3 to 4 if DCE MRI is positive. Despite a limited role of DCE MRI in PIRADS for transition zone (TZ) lesions, it remains helpful in detecting csPCa in TZ, particularly small cancers which may be obscured by BPH nodules and stroma. Although DCE MRI ultimately does not play a role in the final PIRADS category assessment for TZ lesions, enhancement pattern of transition zone lesions in DCE MRI provides pertinent information for lesion characterization that is not described in PIRADS.
While the role of DCE MRI is limited in PIRADS v2.1, it is important to be aware of DCE MRI findings that can improve accuracy in mpMRI interpretation. In patients with suboptimal diffusion weighted imaging (DWI) due to distortion from rectal peristalsis, rectal gas or pelvic implants, DCE MRI acts as an important safety net in assigning a PIRADS category based on T2-weighted MRI findings corroborated with DCE MRI findings. DCE MRI can be a useful adjunct in assessing tumor volume and identifying index lesion in the era of precision medicine and focal therapy of prostate cancer as PIRADS 4 lesion may appear larger in DCE MRI and be ugraded to PIRADS 5, affecting focal therapy treatment planning.
Acknowledgements
No acknowledgement found.References
- Khan A, Moore CM, Minhaj Siddiqui M. Prostate MRI and image quality: The urologist's perspective. Eur J Radiol. 2024 Jan;170:111255. doi: 10.1016/j.ejrad.2023.111255. Epub 2023 Dec 9. PMID: 38101197.
- Lin Y, Yilmaz EC, Belue MJ, Turkbey B. Prostate MRI and image Quality: It is time to take stock. Eur J Radiol. 2023 Apr;161:110757. doi: 10.1016/j.ejrad.2023.110757. Epub 2023 Feb 25. PMID: 36870241; PMCID: PMC10493032.
- Smith CP, Harmon SA, Barrett T, Bittencourt LK, Law YM, Shebel H, An JY, Czarniecki M, Mehralivand S, Coskun M, Wood BJ, Pinto PA, Shih JH, Choyke PL, Turkbey B. Intra- and interreader reproducibility of PI-RADSv2: A multireader study. J Magn Reson Imaging. 2019 Jun;49(6):1694-1703. doi: 10.1002/jmri.26555. Epub 2018 Dec 21. PMID: 30575184; PMCID: PMC6504619.
- Turkbey B, Purysko AS. PI-RADS: Where Next? Radiology. 2023 Jun;307(5):e223128. doi: 10.1148/radiol.223128. Epub 2023 Apr 25. PMID: 37097134; PMCID: PMC10315529.
- Huebner NA, Korn S, Resch I, Grubmüller B, Gross T, Gale R, Kramer G, Poetsch N, Clauser P, Haitel A, Fajkovic H, Shariat SF, Baltzer PA. Visibility of significant prostate cancer on multiparametric magnetic resonance imaging (MRI)-do we still need contrast media? Eur Radiol. 2021 Jun;31(6):3754-3764. doi: 10.1007/s00330-020-07494-1. Epub 2020 Dec 2. PMID: 33263793; PMCID: PMC8128749.
- Westphalen AC, McCulloch CE, Anaokar JM, Arora S, Barashi NS, Barentsz JO, Bathala TK, Bittencourt LK, Booker MT, Braxton VG, Carroll PR, Casalino DD, Chang SD, Coakley FV, Dhatt R, Eberhardt SC, Foster BR, Froemming AT, Fütterer JJ, Ganeshan DM, Gertner MR, Mankowski Gettle L, Ghai S, Gupta RT, Hahn ME, Houshyar R, Kim C, Kim CK, Lall C, Margolis DJA, McRae SE, Oto A, Parsons RB, Patel NU, Pinto PA, Polascik TJ, Spilseth B, Starcevich JB, Tammisetti VS, Taneja SS, Turkbey B, Verma S, Ward JF, Warlick CA, Weinberger AR, Yu J, Zagoria RJ, Rosenkrantz AB. Variability of the Positive Predictive Value of PI-RADS for Prostate MRI across 26 Centers: Experience of the Society of Abdominal Radiology Prostate Cancer Disease-focused Panel. Radiology. 2020 Jul;296(1):76-84. doi: 10.1148/radiol.2020190646. Epub 2020 Apr 21. PMID: 32315265; PMCID: PMC7373346.
- Purysko AS, Baroni RH, Giganti F, Costa D, Renard-Penna R, Kim CK, Raman SS. PI-RADS Version 2.1: A Critical Review, From the AJR Special Series on Radiology Reporting and Data Systems. AJR Am J Roentgenol. 2021 Jan;216(1):20-32. doi: 10.2214/AJR.20.24495. Epub 2020 Nov 19. PMID: 32997518.
- Ziayee F, Schimmöller L, Boschheidgen M, Kasprowski L, Al-Monajjed R, Quentin M, Radtke JP, Albers P, Antoch G, Ullrich T. Benefit of dynamic contrast-enhanced (DCE) imaging for prostate cancer detection depending on readers experience in prostate MRI. Clin Radiol. 2023 Dec 14:S0009-9260(23)00579-2. doi: 10.1016/j.crad.2023.11.026. Epub ahead of print. PMID: 38185579.
Figures
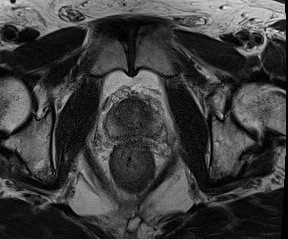
Axial T2W mpMRI shows a lenticular T2W hypointense PIRADS 4 mass at midline and right anterior transition zone mid gland.
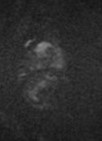
Axial high B-value DWI mpMRI shows a lenticular 1.2 cm hyperintense PIRADS 4 mass at midline and right anterior transition zone mid gland.
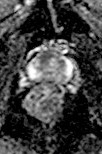
Axial ADC map shows a lenticular 1.2 cm hypointense PIRADS 4 mass at midine and right anterior transition zone mid gland.

Axial dynamic contrast enhanced MRI shows a 1.7 cm early enhancing mass at midline and right anterior transition zone mid gland, larger than DWI/ADC dimension and upgraded to PIRADS 5 due to size >1.5 cm. MRI-ultrasound fusion targeted biopsy was positive for ISUP GG2 cancer at area of enhancement. Focal therapy performed ablated a larger area based on DCE MRI finding and altering treatment planning.