State-of-the-Art Lung MRI for Lung Nodule & Cancer Staging
1Kyushu University, Fukuoka, Japan
Synopsis
Keywords: Body: Lung
Lung MRI has been limited in clinical applications owing to its long scanning time and low signal-to-noise ratio. However, the clinical use of lung MRI for characterizing and staging cancer is increasing because of its superior tissue characterization and ability to perform without radiation exposure, including contrast-enhanced or dynamic breathing studies and diffusion-weighted images, in comparison to CT scans. I will review the role of lung MRI in the characterization of solitary pulmonary nodules and the T, N, and M staging of lung cancer.Abstract
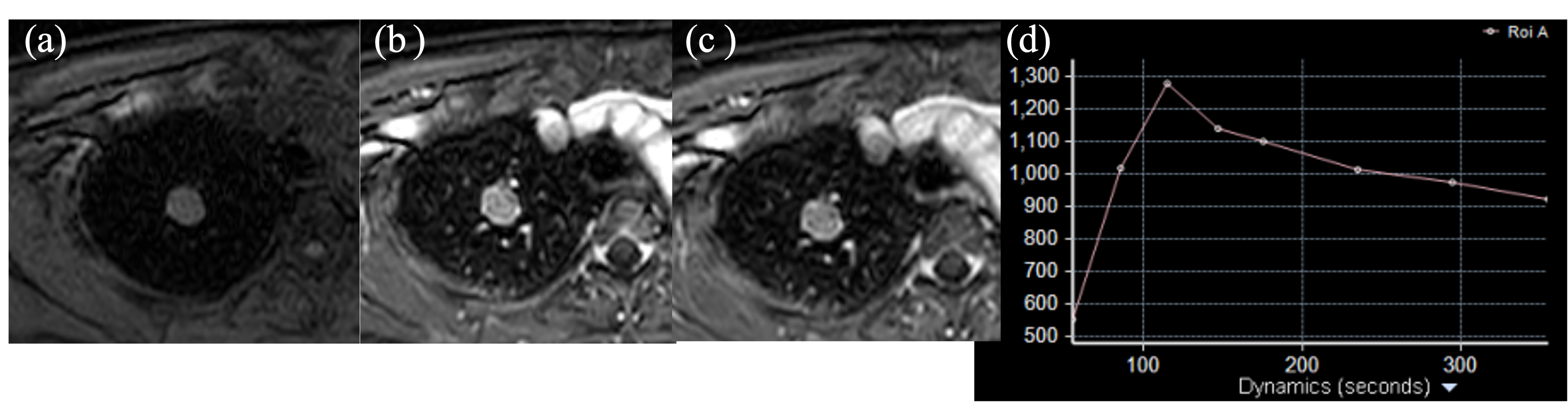
Lung MRI has been limited in clinical applications owing to its long scanning time and low signal-to-noise ratio. However, the clinical use of lung MRI for characterizing and staging cancer is increasing because of its superior tissue characterization and ability to perform without radiation exposure, including contrast-enhanced or dynamic breathing studies and diffusion-weighted images, in comparison to CT scans1.Dynamic contrast-enhanced MRI (DCE-MRI), diffusion-weighted imaging (DWI), and chemical shift imaging are valuable for characterizing solitary pulmonary nodules (SPNs)2-4. Tuberculomas and hamartomas must be differentiated from lung cancer on CT scans; tuberculomas exhibit ring enhancement on DCE-MRI, while chemical shift imaging can detect a small amount of fat in hamartomas. This is particularly helpful for fatless hamartomas identified on CT scans5.
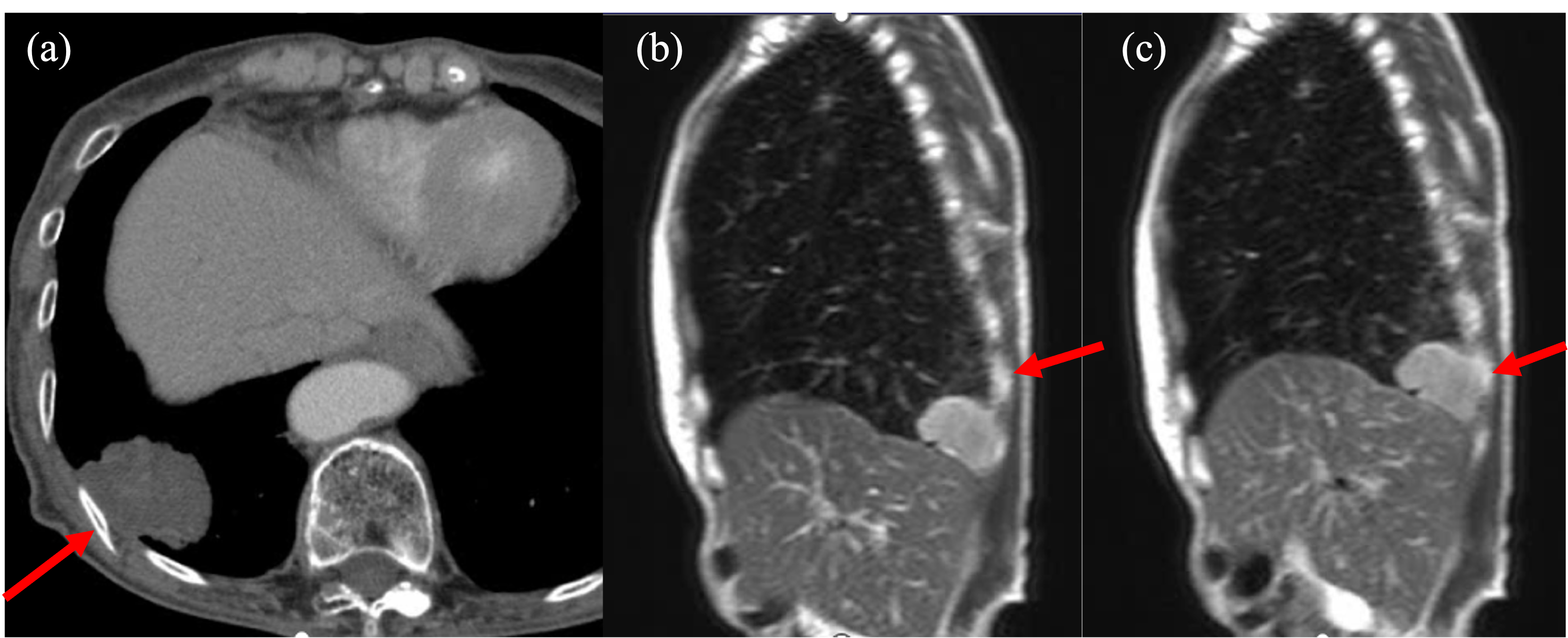
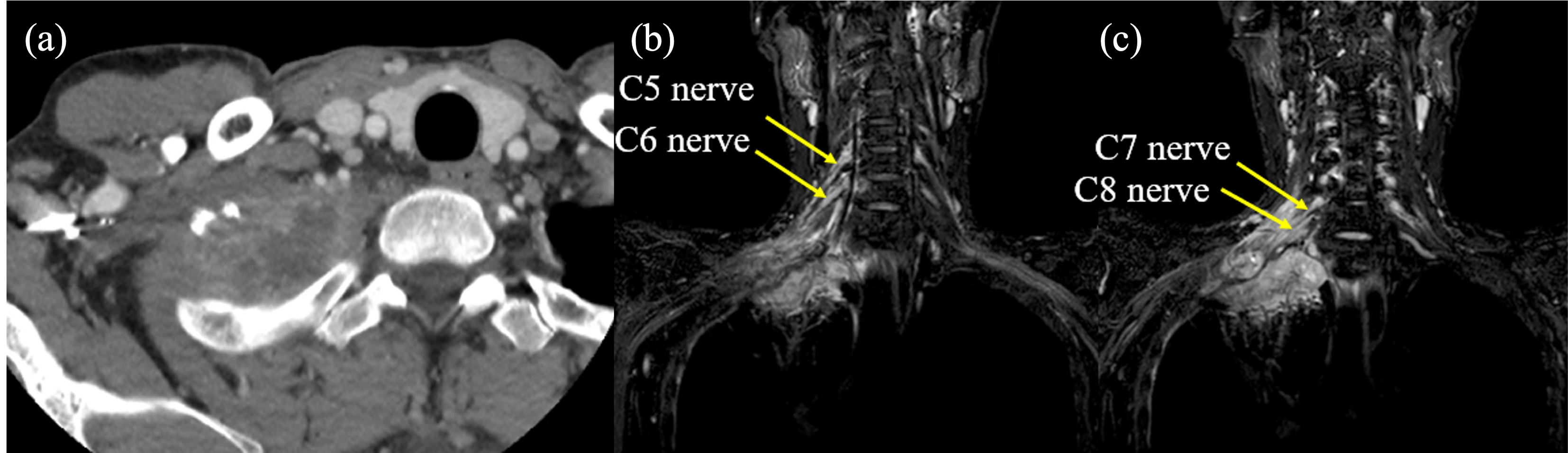
Lung MRI is also useful in T and N staging in primary lung cancer. For T staging, contrast-enhanced MRI or cine MRI using dynamic breathing techniques is indicated when determining whether it is T3 (invasion of the chest wall or pericardium) or T4 (invasion into the diaphragm, mediastinum, heart and major vessels, trachea, carina, esophagus, or spine) based on enhanced CT or FDG-PET/CT6. Contrast-enhanced MRI is superior in tissue characterization and is useful in the evaluation of chest wall or mediastinal invasion. Dynamic breathing MRI can obtain dynamic chest wall motion of both the lung tumor and chest wall, mediastinum, and great vessels. When we can confirm the separate motion of the lung tumor and chest wall or mediastinum, direct invasion into the mediastinum or mediastinum can be ruled out7.
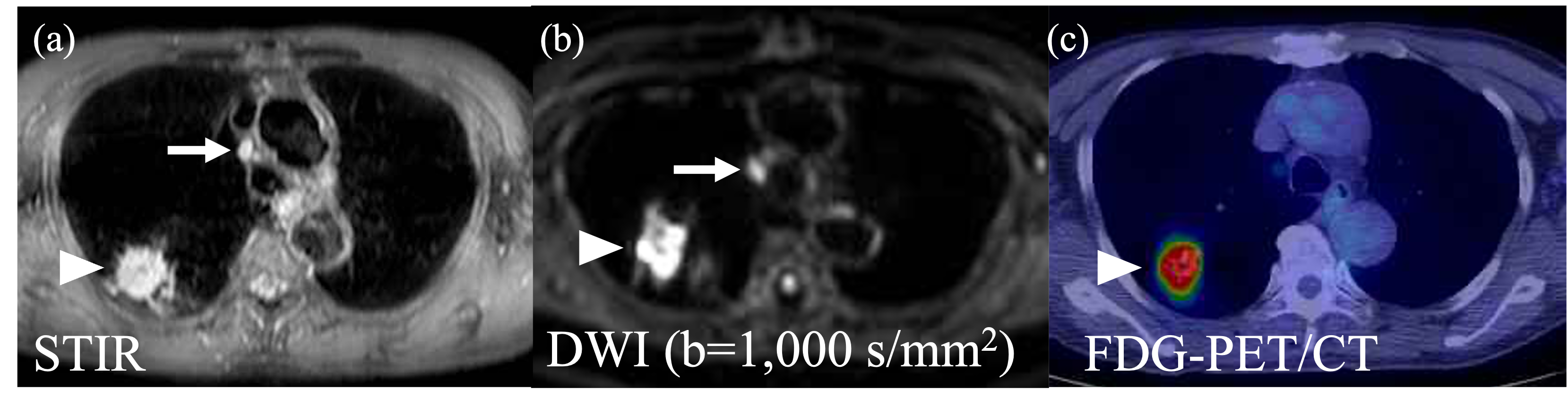
There have been many studies on the utility of lung MRI for N-staging of lung cancer. Ohno et al. reported that STIR demonstrated superior diagnostic value than FDG-PET/CT and DWI showed comparable value to FDG-PET/CT in N-staging8. Three previous meta-analyses on MRI have shown that DWI demonstrates equal or even superior diagnostic value for N-staging compared with FDG-PET/CT, and those studies showed pooled sensitivity/specificity per patient of 68%/92%, 87%/88%, and 72%/97%, respectively9-11. Shen et. al. reported that the pooled sensitivity and specificity were 72%/97% for DWI and 65%/93% for FDG-PET/CT, although there was no significant difference11.
Contrast-enhanced CT, contrast-enhanced brain MRI, bone scintigraphy, and FDG-PET/CT are the gold standards for M staging in primary lung cancer; however, there have been several promising reports on whole-body MRI such as STIR-FACE, DWIBS, and PET-MRI for M-staging12-15. Medeiros et al. reported a meta-analysis based on four studies that showed pooled sensitivity and specificity of 92% and 93% for whole-body MRI, 78% and 91% for whole-body DWI, and 83% and 93% for FDG-PET/CT, respectively, and there were no statistical differences between the diagnostic odds ratio of whole-body MRI and DWI and that of PET/CT16.
In this educational lecture, I will review the role of lung MRI in the characterization of solitary pulmonary nodules and the T, N, and M staging of lung cancer.
Acknowledgements
All authors have no grant supporting and no conflict of interests in the submission of this manuscript.References
1) Ohno Y, et al. State of the Art MR Imaging for Lung Cancer TNM Stage Evaluation. Cancers (Basel) 2023;15:950
2) Kono R, et al. Dynamic MRI of solitary pulmonary nodules: comparison of enhancement patterns of malignant and benign small peripheral lung lesions. AJR 2007; 188:26-36
3) Chung MJ, et al. Pulmonary sclerosing hemangioma presenting as solitary pulmonary nodule: dynamic CT findings and histopathologic comparisons. AJR 2006; 187:430-437
4) Chong S, et al. Neuroendocrine tumors of the lung: clinical, pathologic, and imaging findings. Radiographics 2006; 26:41-58
5) Hochhegger B, et al. Chemical-shift MRI of pulmonary hamartomas: initial experience using a modified technique to assess nodule fat. AJR 2012; 199:W331-W334
6) Tang W, et al. The presurgical T staging of non-small cell lung cancer: efficacy comparison of 64-MDCT and 3.0 T MRI. Cancer Imaging 2015; 15:14-20
7) Sakai S, et al. Bronchogenic carcinoma invasion of the chest wall: Evaluation with dynamic cine MRI during breathing. J Comput Assist Tomogr 1997; 21:595–600
8) Ohno Y et al. N stage disease in patients with non-small cell lung cancer:efficacy of quantitative and qualitative assessment with STIR turbo spin-echo imaging, diffusion-weighted MR imaging, and fluorodeoxyglucose PET/CT. Radiology 2011; 261:605-615
9) Shen G, et al. Performance of DWI in the nodal characterization and assessment of lung cancer:a meta-analysis. AJR Am J Roentgenol 2016; 206:283-290
10) Peerlings J, et al. The diagnostic value of MR imaging in determining the lymph node status of patients with non-small cell lung cancer:a meta-analysis. Radiology 2016; 281:86-98
11) Shen G, et al. Comparison of 18F-FDG PET/CT and DWI for detection of mediastinal nodal metastasis in non-small cell lung cancer:a meta-analysis. PLoS One 2017; 12:e0173104
12) Takenaka D, et al. Detection of bone metastases in non-small cell lung cancer patients: Comparison of whole-body diffusion-weighted imaging (DWI), whole-body MR imaging without and with DWI, whole-body FDG-PET/CT, and bone scintigraphy. J. Magn. Reson. Imaging 2009; 30:298–308
13) Lee SM, et al. Preoperative staging of non-small cell lung cancer: Prospective comparison of PET/MR and PET/CT. Eur Radiol 2016; 26:3850–3857
14) Schaarschmidt BM, et al. Thoracic staging with 18F-FDG PET/MR in non-small cell lung cancer—Does it change therapeutic decisions in comparison to 18F-FDG PET/CT? Eur Radiol 2017; 27:681–688
15) Ohno Y, et al. Comparison of Diagnostic Accuracy for TNM Stage Among Whole-Body MRI and Coregistered PET/MRI Using 1.5-T and 3-T MRI Systems and Integrated PET/CT for Non-Small Cell Lung Cancer. AJR Am J Roentgenol 2020; 215:1191–1198
16) Medeiros TM, et al. 18F-FDG PET/CT and whole-body MRI diagnostic performance in M staging for non-small cell lung cancer: A systematic review and meta-analysis. Eur Radiol 2020; 30:3641–3649.
Figures