9021
Challenge examples: Visualisation of shear from cine MRI for detection of gastrointestinal adhesions1Centre for Medical Imaging, University College London, London, United Kingdom
Synopsis
Keywords: Gastrointestinal Motility
Motivation: Further examples and methodology extending our abstract to the Unmet Needs Challenge on Gastrointestinal Motility [1].
Goal(s): Localisation of regions of bowel that are affected by adhesions.
Approach: We previously proposed that regions of reduced shear may correspond to bowel motility hindered by adhesions [1]. Shear was calculated from coronal cine frames and presented as red colour overlays. Here we present further examples and add a linked-cursor that links regions of restricted motility to impressions of tethering in axial structural images, e.g. angulated bowel loops.
Results: Descriptive exemplars are presented.
Impact: Adhesions cannot be directly seen in MRI but tethering may be apparent in structural and motility images. The proposed post-processing methods use readily available MR sequences and Results suggest further investigation to validate observations and to assess potential clinical benefit.
Introduction
In previous work [1] we computed local shear from the deformation fields derived as part of registering cine frames. Regions with low shear were presented as a red overlay and may be indicative of restricted motility due to adhesions. Here we provide additional examples and add a 3D linked cursor to aid visualisation of structural features in orthogonal axial slices.Method and Results
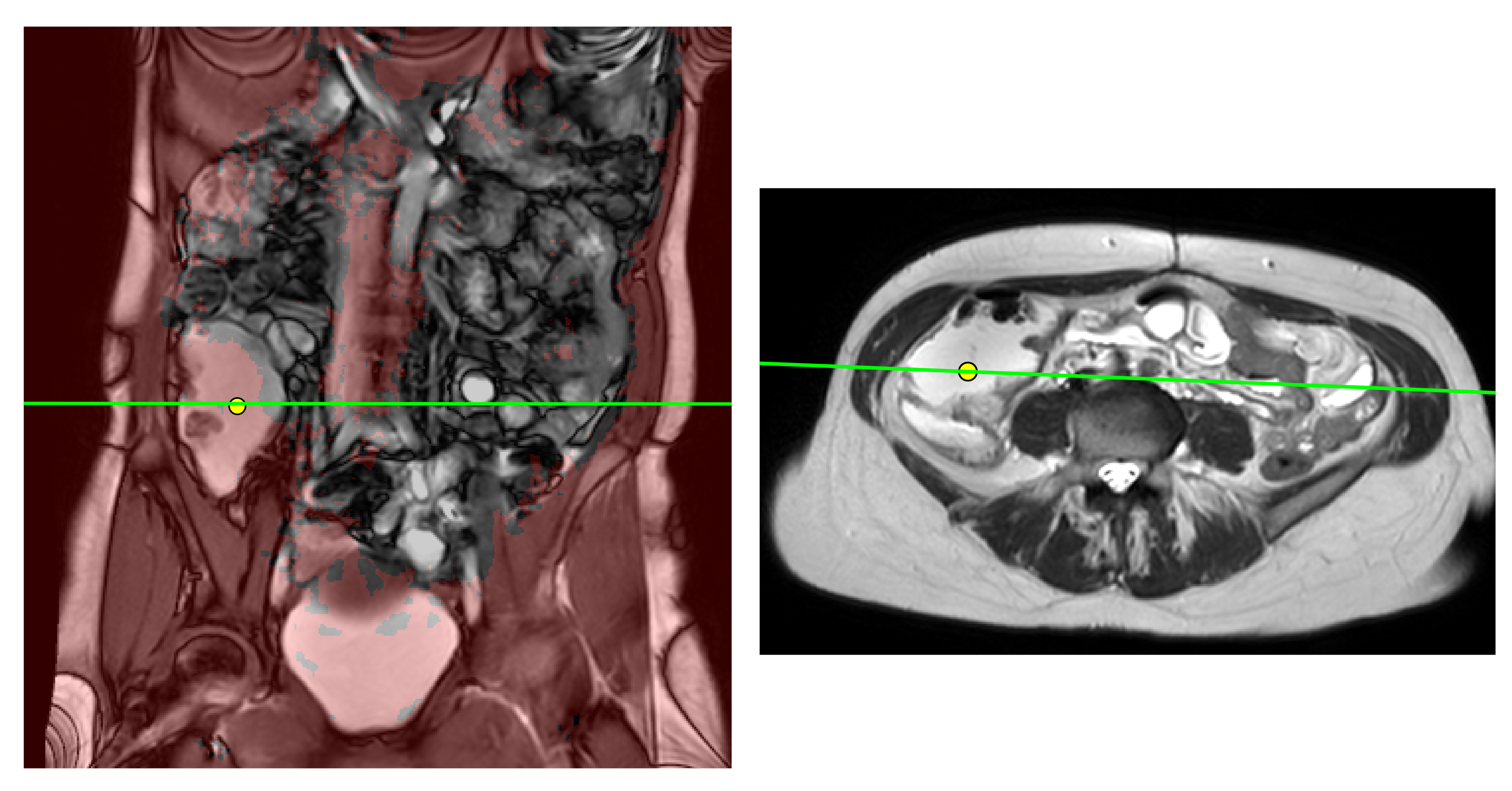
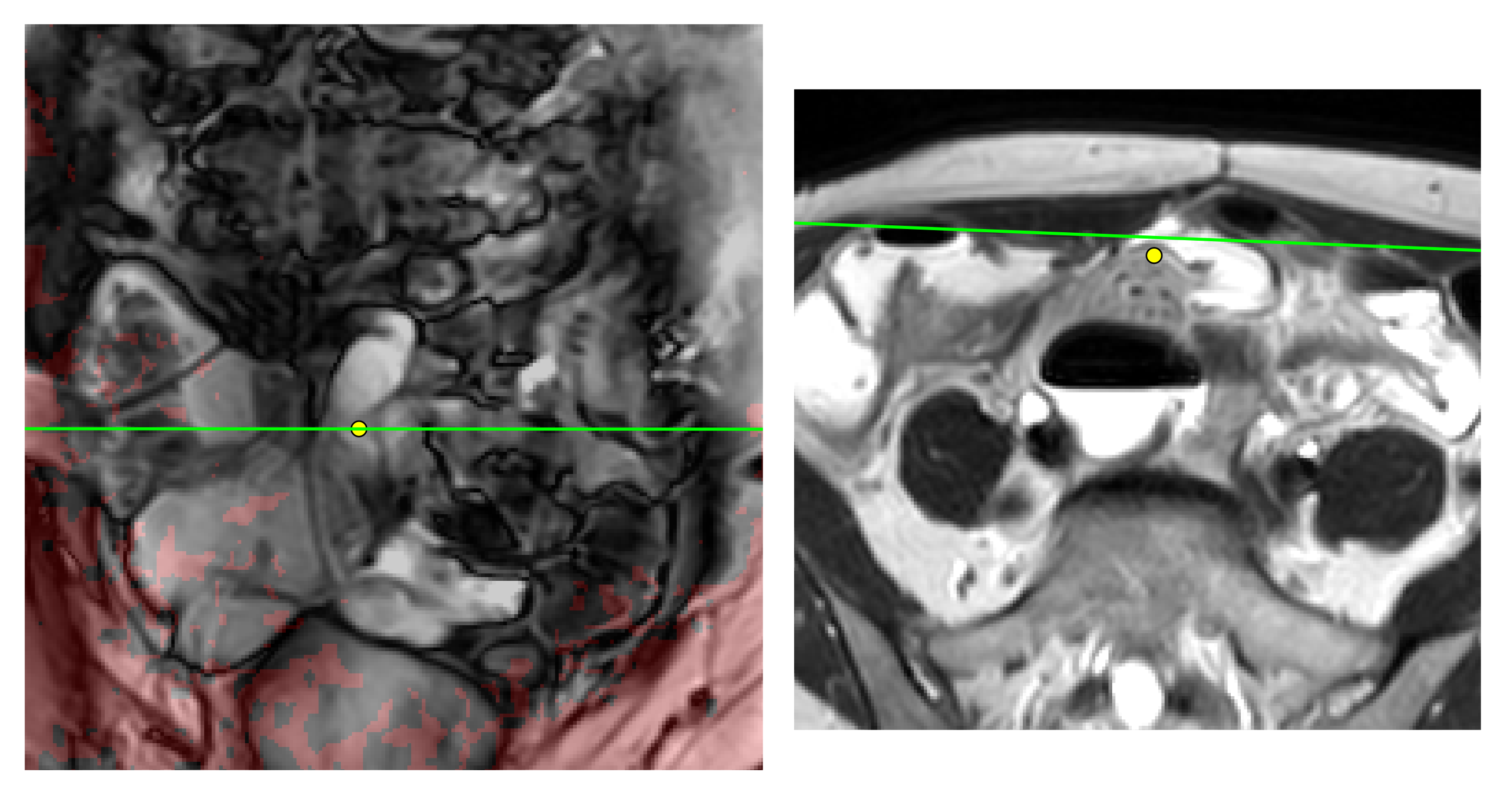
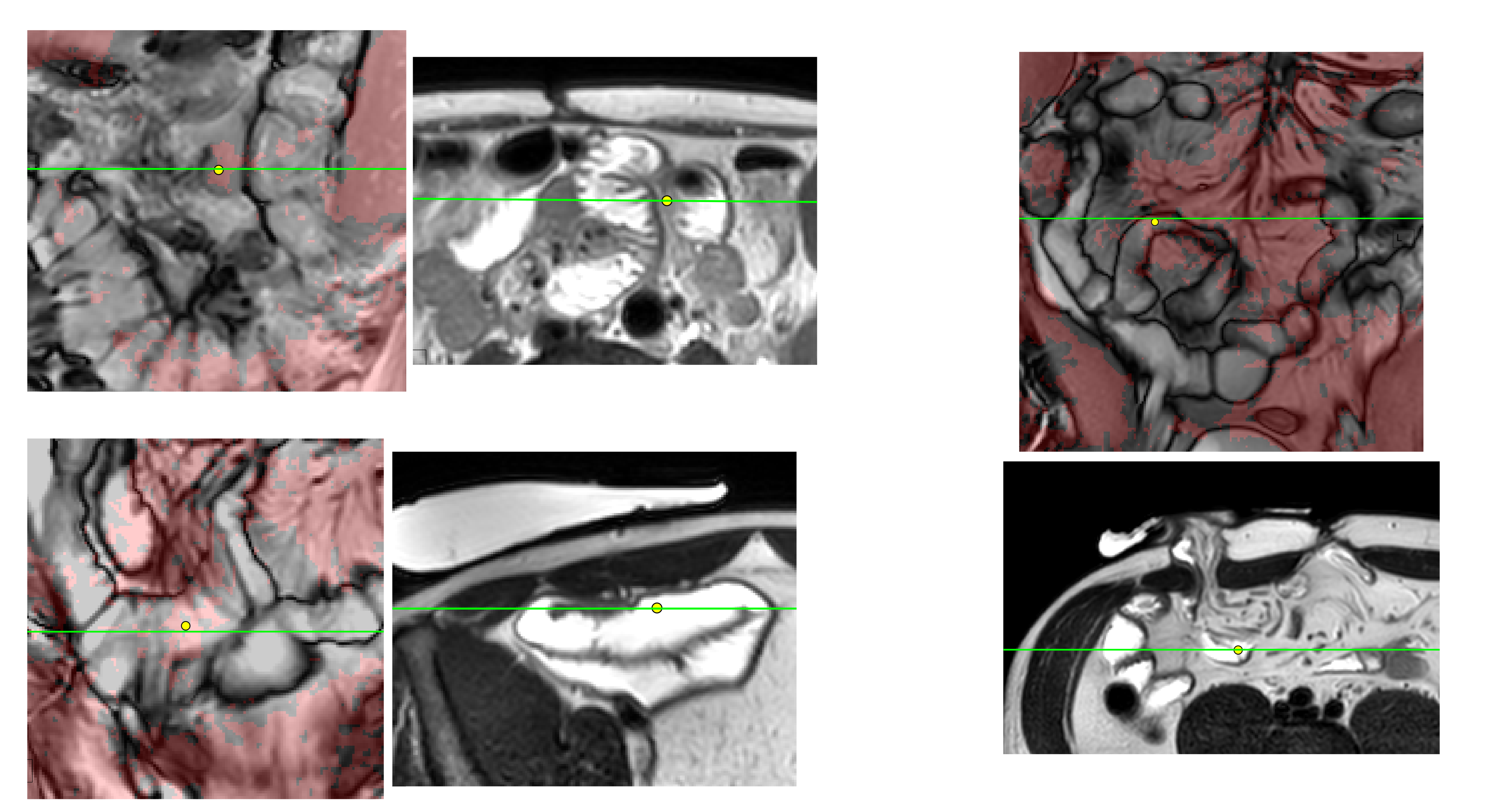
Data sets from patient small bowel examinations where adhesions were mentioned in the radiological report were processed. The single-slice 16s coronal cine images were processed as described previously [1]. Additionally, a two breath-hold fast spin echo axial sequence from the standard protocol was loaded into the software (developed in MATLAB). This is used here to provide structural information. The software user interface allows the cine scan to be scrolled in time and slice, with the red overlay varying only with each slice. The position of the intersection between the coronal and axial scan planes is shown as green lines and the closest slice in the coronal and axial orientations is displayed as the cursor is moved. The corresponding position of the cursor in 3D is shown as yellow dots. This facilitates 3D spatial navigation through the data, for example to see if a red overlay region in the coronal data corresponds to an angulated bowel loop in the structural axial data.Results: Examples with descriptive narratives are presented in Figures 1-4.
Discussion
Some of the requested 'must have' and 'nice to have' features specified in the Challenge are not met in this proposal. However, the scans used here come from our current clinical small bowel imaging protocol and are readily achievable on a modern commercial scanner. There is also an argument that in the context of the whole patient visit (including fasting, drinking oral contrast, changing), spending time on highly informative sequences makes more sense than a very rapid scan with reconstructions reliant on generic prior knowledge.Our cine assessment has some limitations. The registration is performed on 2D cine frames and so is not equally sensitive to motion in all three directions. Through-plane motion may still be detectable because the bowel loop will appear to change in size due to motility but also in a confounding way due to breathing. The threshold for the red overlay was set by manual observation (but has been fixed throughout this work). Regions of homogeneous intensity, for example in distended bowel, do not register well and so can present as lacking motion. Regions that are tethered but still moving significantly may not be highlighted. These regions may be functioning adequately at the time of the scan, but potentially could lead to obstructions in the future. For this reason, we would only recommend using the color overlay as an addition to current radiological practice. The presented examples are subject to biases - only patients where adhesions were mentioned in the report were examined and examples were hand-picked.
Validation is challenging because the presence, or absence, of adhesions can only be verified at surgery. The MR sequences are readily available but the calculations, presentation and linked orthogonal scrolling may not be available on current PACs systems. We suggest the next steps are to record radiological reporting opinions of the technique, and, verification of predictions with findings from patients undergoing surgery or adhesiolysis.
Acknowledgements
No acknowledgement found.References
[1] Atkinson D. and Taylor CS. Visualisation of shear from cine MRI: towards detection of gastrointestinal adhesions. ISMRM 2024, submission number 265.Figures
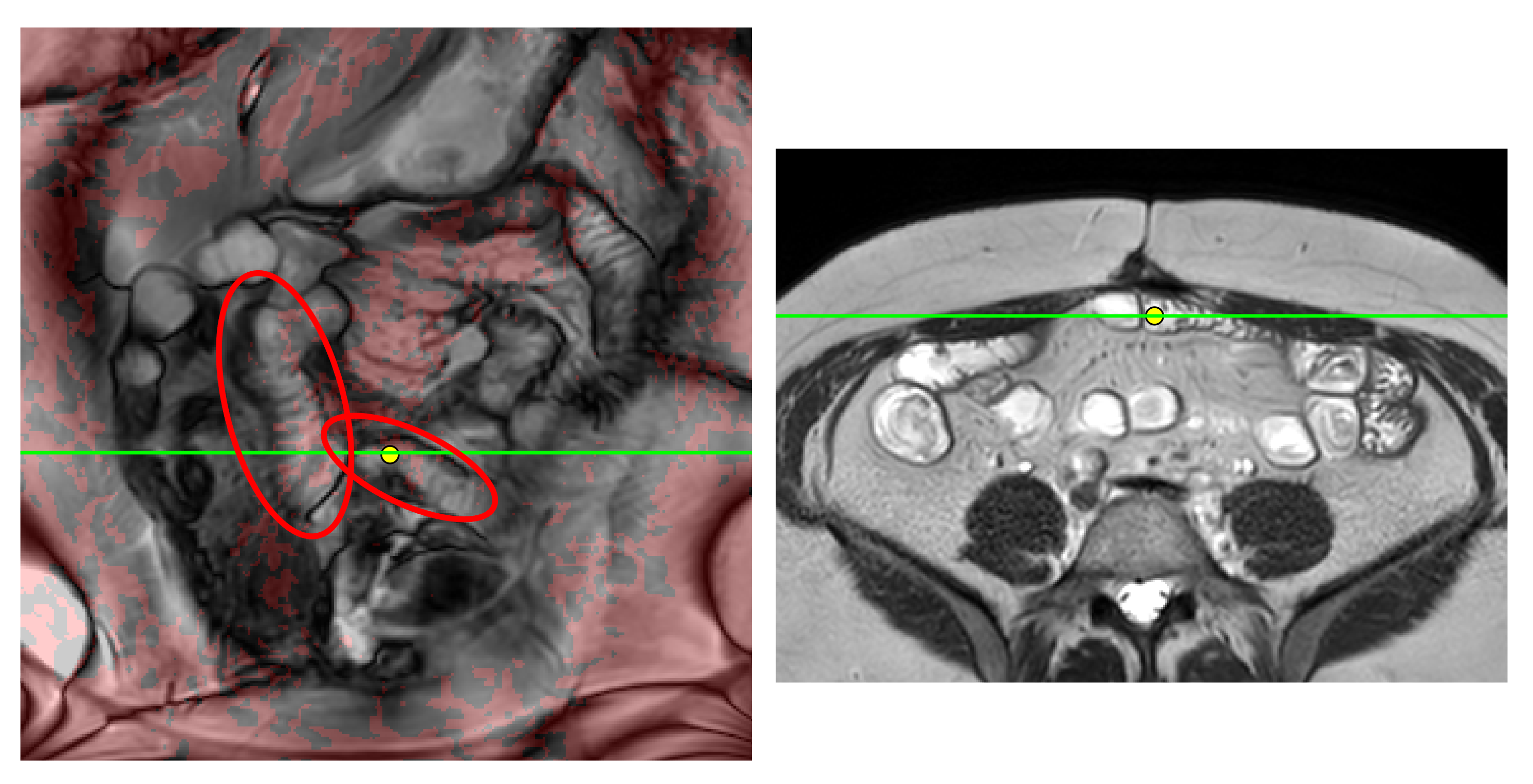
Left, example cine frame (grayscale) from free-breathing scan with overlay shown in red for regions calculated to have low shear. Right, axial slice from breath-hold scan. Red ovals highlight bowel regions with low shear. Cine frames can be played as a movie but the overlay is a static summary, hence there may be small positional mismatches between the overlay and both individual cine frames, and the breath-hold sequences. Green lines show intersecting slice positions, yellow dots are at the same 3D position in each image.