5193
Gray blood late gadolinium enhancement based on phase-sensitive inversion recovery for improved detection of myocardial scar and cardiac mass1Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan,Hubei, China
Synopsis
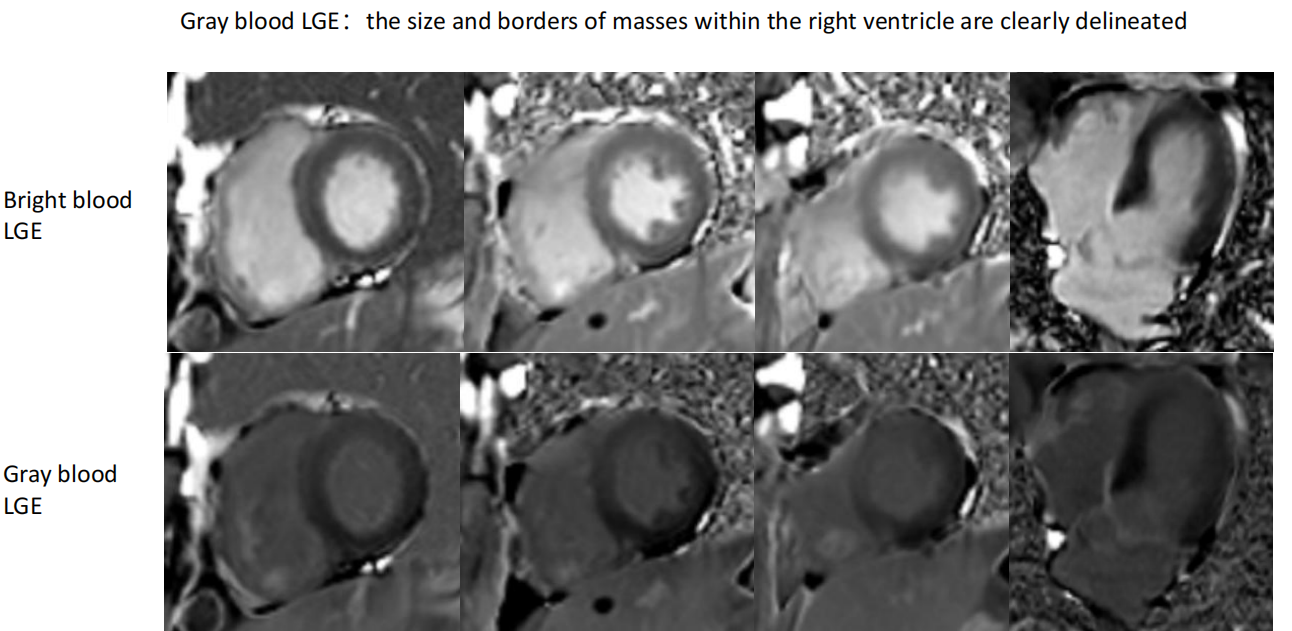
Motivation: During magnetic resonance imaging for myocardial viability, the bright blood within the heart chambers can significantly diminish the apparent volume of myocardial scars or obscure the visualization of cardiac masses.
Goal(s): An imaging technique that can reduce the signal from the blood pool and highlight the signal of the scar tissue or cardiac masses is needed to increase diagnostic accuracy.
Approach: Subjects are randomized to undergo gray blood and bright blood late gadolinium enhancement (LGE) imaging using phase-sensitive inversion recovery technique to compare the diagnostic differences for scar tissue or cardiac masses.
Results: Gray blood LGE reveals more myocardial scars or cardiac masses.
Impact: Gray blood LGE enhances the detection of myocardial scars and intracavitary cardiac masses, especially those showing enhancement after contrast injection, facilitating clinical decisions and improving patient outcomes. Additionally, the PSIR-based gray blood approach offers greater adaptability and ease of use.
Introduction
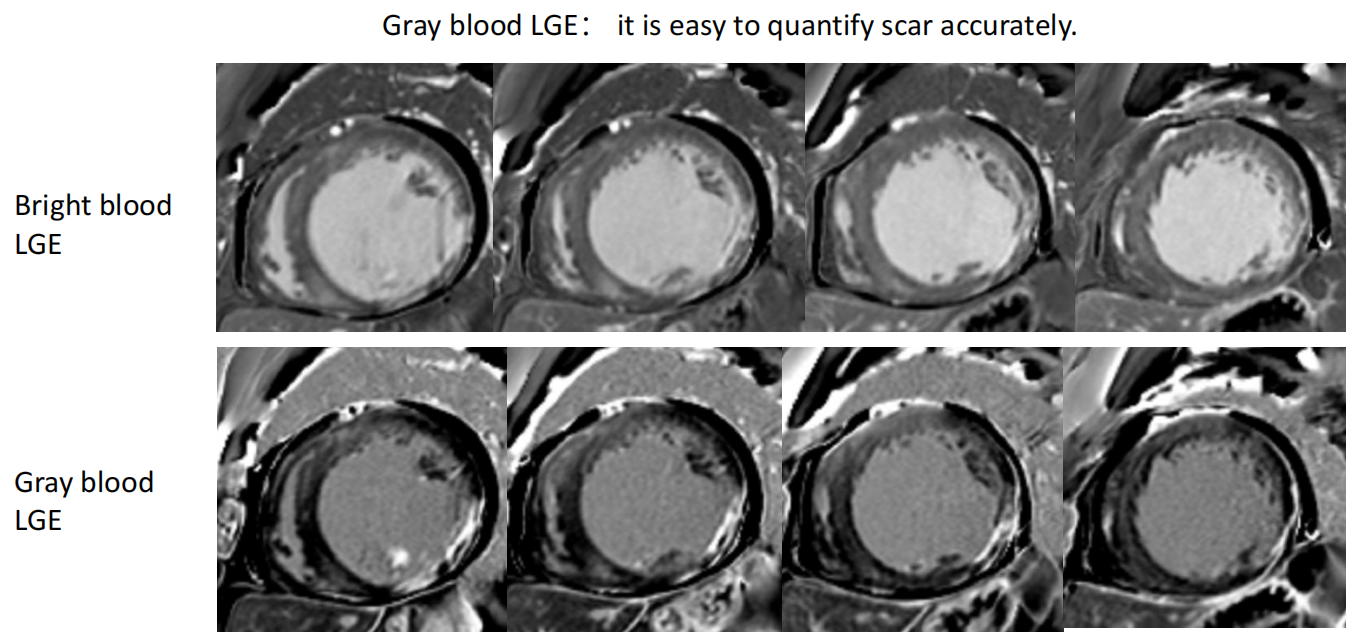
Myocardial scar tissue exhibits enhancement after injection of contrast agents. Although there is good contrast between the scar and normal myocardium, the contrast between the blood pool and myocardial scar may be limited, especially in the presence of subendocardial myocardial scars. This results in uncertainty for physicians regarding the precise location of the scar-blood pool interface, which could affect the evaluation of the transmural extent of the scar. Additionally, regarding intracardiac tumors, the administration of contrast agents can result in enhancement of certain masses, rendering them indiscernible from the blood pool, and potentially leading to underdiagnosis or misdiagnosis.Methods
A cohort of 41 CMR patients, consisting of 28 men and 13 women with an average age of 55 ±9 years, underwent a stepwise scanning protocol. Within 10-20 minutes following the intravenous administration of a gadolinium contrast agent at a dose of 0.2 mmol/kg, they were randomly assigned to undergo either conventional myocardial late gadolinium enhancement (bright blood LGE) scanning or left ventricular blood pool nulling (Gray blood LGE) scanning. The post-contrast injection times at the start of each LGE scan were documented. Prior to LGE scanning, a TI-scout scan was conducted to ascertain the precise TI values that would null the signals of normal myocardium and the left ventricular blood pool. Two CMR technicians independently outlined regions of interest within the ventricular blood pool, normal viable myocardium, and areas of myocardial scar or cardiac mass to obtain signal intensity values. These values were used to assess the relative contrast among the three tissue types, with relative contrast between tissues A and B defined as the mean signal difference between A and B divided by the mean signal of B. The signal intensity for each tissue was determined by the average of the measurements from both technicians, and the consistency of the measurements was evaluated. Independent assessments of bright blood and gray blood LGE images were made by two CMR physicians, using the American Heart Association’s 16-segment model for left ventricular myocardial analysis on short-axis views to identify the presence of LGE. The transmural extent of LGE was evaluated using a 3-point Likert scale: 0 points for no LGE, 1 point for LGE affecting less than 50% of the wall thickness, and 2 points for LGE affecting more than 50% of the wall thickness, to measure the left ventricular scar burden. A binary scale (confident/not confident) was also employed to grade the level of certainty for each LGE observation, and observer consistency was compared.Results
Compared to bright blood LGE, gray blood LGE significantly improved the relative contrast between the scarred myocardium or cardiac mass and the left ventricular blood pool (p < 0.001). It also significantly increased the relative contrast between the blood pool and normal myocardium (p < 0.001). However, there was no significant difference in the relative contrast between the scar tissue or cardiac mass and normal myocardium. Gray blood LGE detected more positive cases of LGE than bright blood LGE and showed higher diagnostic confidence in identifying myocardial scar or cardiac mass, with the difference being statistically significant (p < 0.05). The interobserver consistency was good for both gray blood LGE and bright blood LGE (both with ICC > 0.75).Conclusion
Compared to bright blood LGE, gray blood LGE identified a higher number of myocardial scars or cardiac masses, improving the detection rate of scarred myocardium or cardiac mass and boosting the observers' confidence. Furthermore, gray blood LGE does not require additional magnetization preparation pulses, allowing for its clinical application on existing MR systems without the need for extensive optimization, software updates, or extra training.Acknowledgements
No acknowledgement found.References
1. Eitel I, Gehmlich D, Amer O, Wohrle J, Kerber S, Lauer B, et al. Prognostic relevance of papillary muscle infarction in reperfused infarction as visualized by cardiovascular magnetic resonance. Circ Cardiovasc Imaging. 2013;6(6):890–8.
2. Kim RJ, Wu E, Rafael A, et al. The use of contrast-enhanced magnetic resonance imaging to identify reversible myocardial dysfunction. N Engl J Med. 2000;343(20):1445–53.
3. Francis R, Kellman P, Kotecha T, Baggiano A, Norrington K, Martinez-Naharro A, Nordin S, Knight DS, Rakhit RD, Lockie T, Hawkins PN, Moon JC, Hausenloy DJ, Xue H, Hansen MS, Fontana M. Prospective comparison of novel dark blood late gadolinium enhancement with conventional bright blood imaging for the detection of scar. J Cardiovasc Magn Reson. 2017;19:91.
4. Briasoulis A, Mallikethi-Reddy S, Palla M, Alesh I, Afonso L. Myocardial fibrosis on cardiac magnetic resonance and cardiac outcomes in hypertrophic cardiomyopathy: a meta-analysis. Heart. 2015;101(17):1406–11.
5. Bulluck H, Yellon DM, Hausenloy DJ. Reducing myocardial infarct size: challenges and future opportunities. Heart. 2016;102(5):341–8.
6. Kim RJ, Fieno DS, Parrish TB, Harris K, Chen EL, Simonetti O, Bundy J, Finn JP, Klocke FJ, Judd RM. Relationship of MRI delayed contrast enhancement to irreversible injury, infarct age, and contractile function. Circulation. 1999; 100:1992–2002.
Figures