5192
MRI Features of Stroke in Tuberculous Meningitis: a case report1Human Biology, University of Cape Town, Cape Town, South Africa, 2Francis Crick Institute, London, United Kingdom, 3Infectious Disease, Imperial College London, London, United Kingdom, 4Centre for Infectious Disease Research in Africa, Institute of Infectious Disease and Molecular Medicine, Cape Town, South Africa, 5Radiology, Groote Schuur Hospital, Cape Town, South Africa
Synopsis
Keywords:
Motivation: TBM is the most severe form of tuberculosis and often leads to death or neurological sequelae. Inflammation caused by a dysregulated inflammatory response can cause stroke, a frequent cause of morbidity and mortality in TBM.
Goal(s): To accurately identify areas affected by stroke in TBM.
Approach: MRI brain scan was performed on 1.5 Tesla, Skyra scanner equipped with an 20 channel coil and parameters were derived from the following acquisitions: 3D T1-MPRAGE pre- and post-gadolinium enhancement imaging; DWI and ADC map, FLAIR, and GRE.
Results: MRI is reliable in identifying stroke features and the imaging findings were pivotal to prompt treatment of TBM.
Impact: 14-year-old with a left CNVI palsy and lower limb weakness, was admitted due to onset of seizure. Tuberculous meningitis complicated by stroke was diagnosed as the cause. The incidence, consequences and MRI features of TBM are discussed in this report.
Background
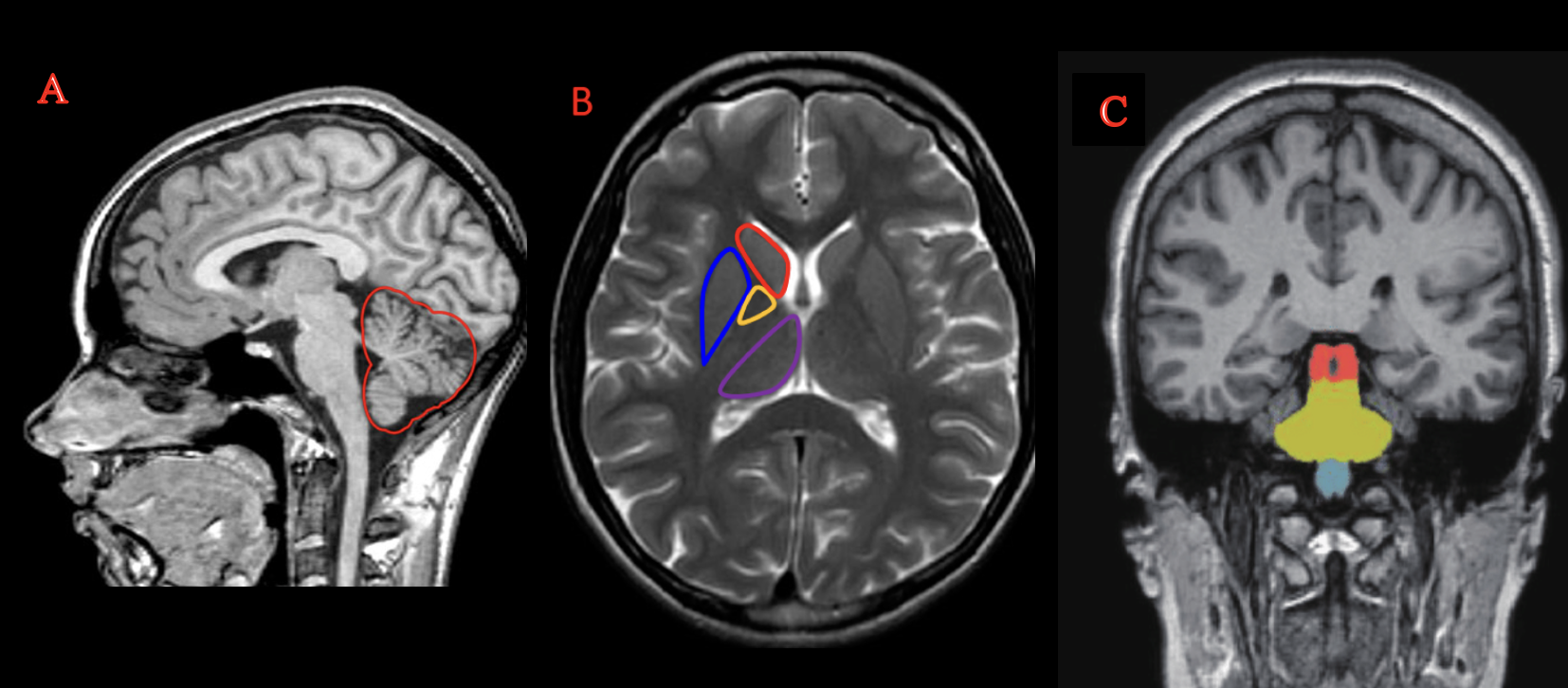
Tuberculosis (TB) is a significant public health problem and is associated with an increased social burden, health care expenses, mortality and morbidity. Mycobacterium tuberculosis (M. tuberculosis) is a slow growing aerobic intra-cellular bacillus, which initially infects the lungs. M. tuberculosis enters the human body via the respiratory tract and travels through the bloodstream into the central nervous system 1. Recent epidemiological work revealed that TBM is the most devastating form of TB, accounting for 1% to 2% of patients with active TB in South Africa 2. Complications of Tuberculous Meningitis (TBM) that confer a poor clinical outcome include stroke, tuberculomas and hydrocephalus 3. Stroke is the most reported complication and occurs in 15-57% of cases with TBM 4. Many patients experience neurologic deficits with cranial nerve (CN) palsies due to persistent inflammation 5. MRI is the gold standard for assessment of structural changes and is highly sensitive in detecting stroke. The common stroke areas are shown in Figure 1.Case report
A 14-year-old boy previously well presented at the local clinic with reduced level of consciousness preceded by a seizure. He was referred to our hospital for evaluation of a possible post traumatic space occupying lesion. He reported a history of a collapse whilst playing football and subsequently began bed wetting and had intermittent blurry vision and behavioural changes. On physical examination, his pulse was 86 beats per minutes, in sinus rhythm and blood pressure was 146/69 mmHg. His temperature was 38.8°C. There was clinical evidence of a lateral rectus (CNVI) palsy in his left eye, reduced cognitive function, and left lower limb weakness.His white cell count was 18.71 x109/L (normal range 3.6-11.0 x109/L). A lumber puncture was M. tuberculosis GeneXpert positive. A chest x-ray revealed miliary nodules. On a head computerized tomography (CT) scan, there was diffuse sulcal effacement in keeping with cerebral eodema and raised intracranial pressure, hypodense changes in the left basal ganglia, left frontal and right parietal lobes. MRI was performed for further assessment. The patient was transferred to the rehabilitation center for continuity of care on ceftriaxone, anti-tuberculous therapy (Rifafour) and prednisone treatment.
Methods
The patient underwent an MRI brain on a 1.5 Tesla, Siemens Magnetom Skyra scanner equipped with an 20 channel coil in the head-first supine position. MRI sequence parameters were derived from the following acquisitions: three-dimensional (3D) T1 magnetization-prepared rapid gradient-echo (MPRAGE) axial pre- and post- gadolinium (GAD) enhancement imaging (TR/TE = 2000/3.24, voxel size = 0.5 x 0.5 x 1.0 mm); diffusion weighted imaging (DWI) and apparent diffusion coefficient (ADC) mapping (TR/TE = 5310/76, voxel size = 1.7 x 1.7 x 5.0 mm, b-value 0 &1000 s/mm), fluid attenuated inversion recovery (FLAIR) (TR/TE = 9000/92, voxel size = 0.5 x 0.5 x 5.0 mm), gradient echo (GRE) (TR/TE = 6120/75, voxel size = 0.7 x 0.7 x 5.0 mm).Findings
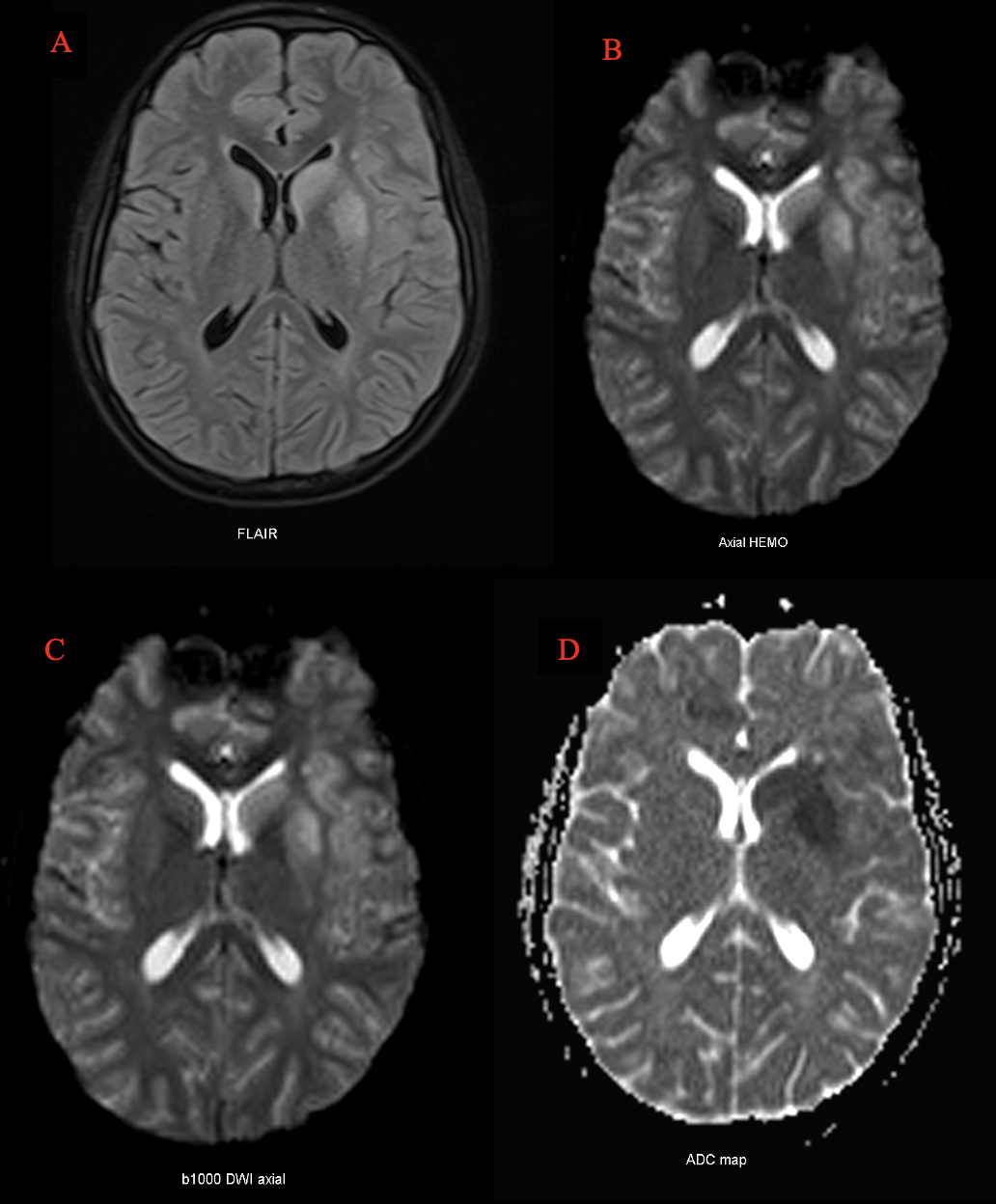
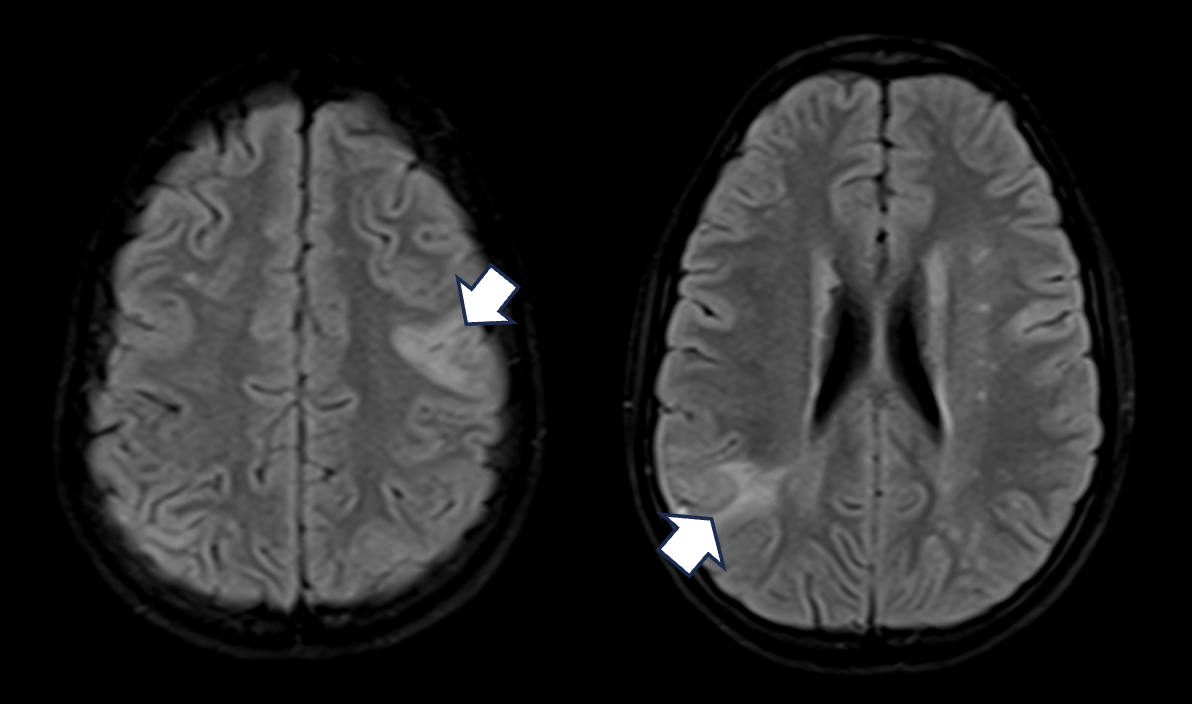
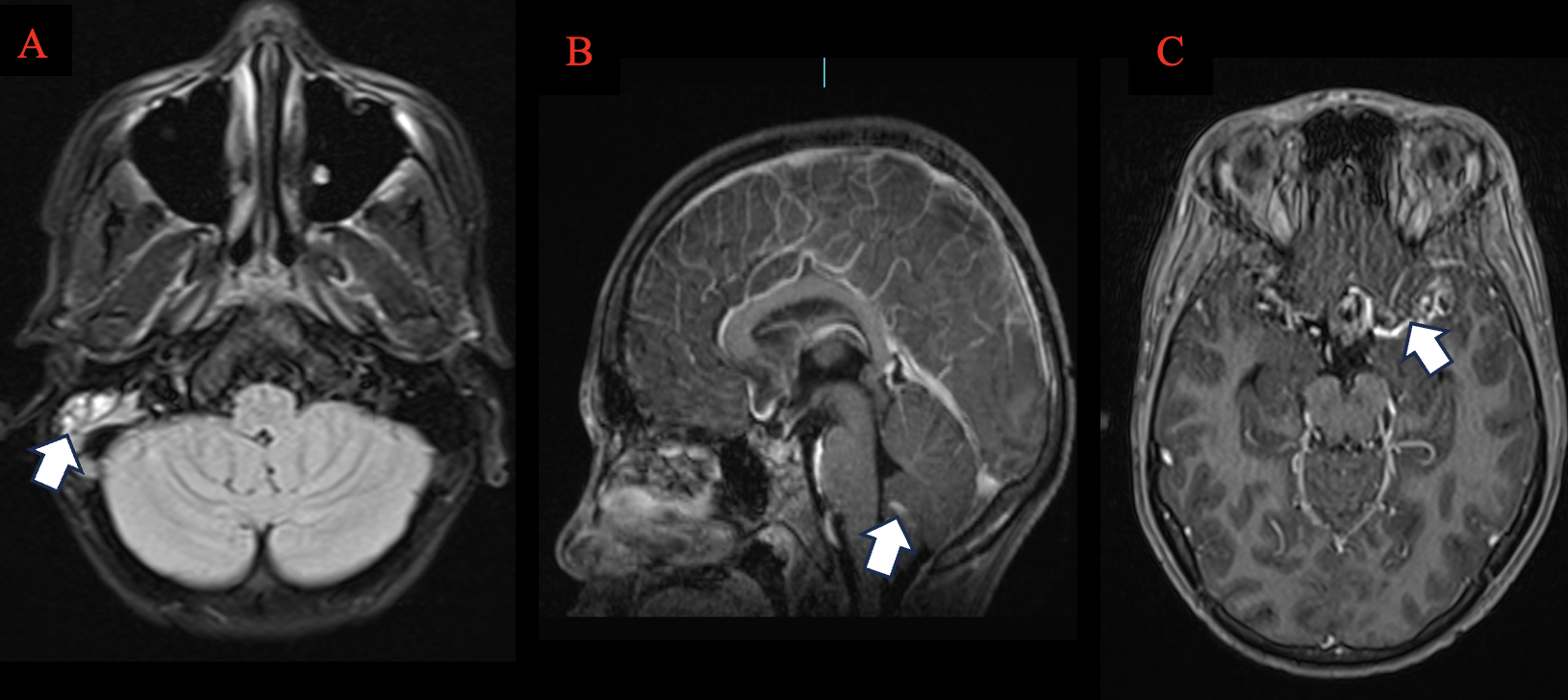
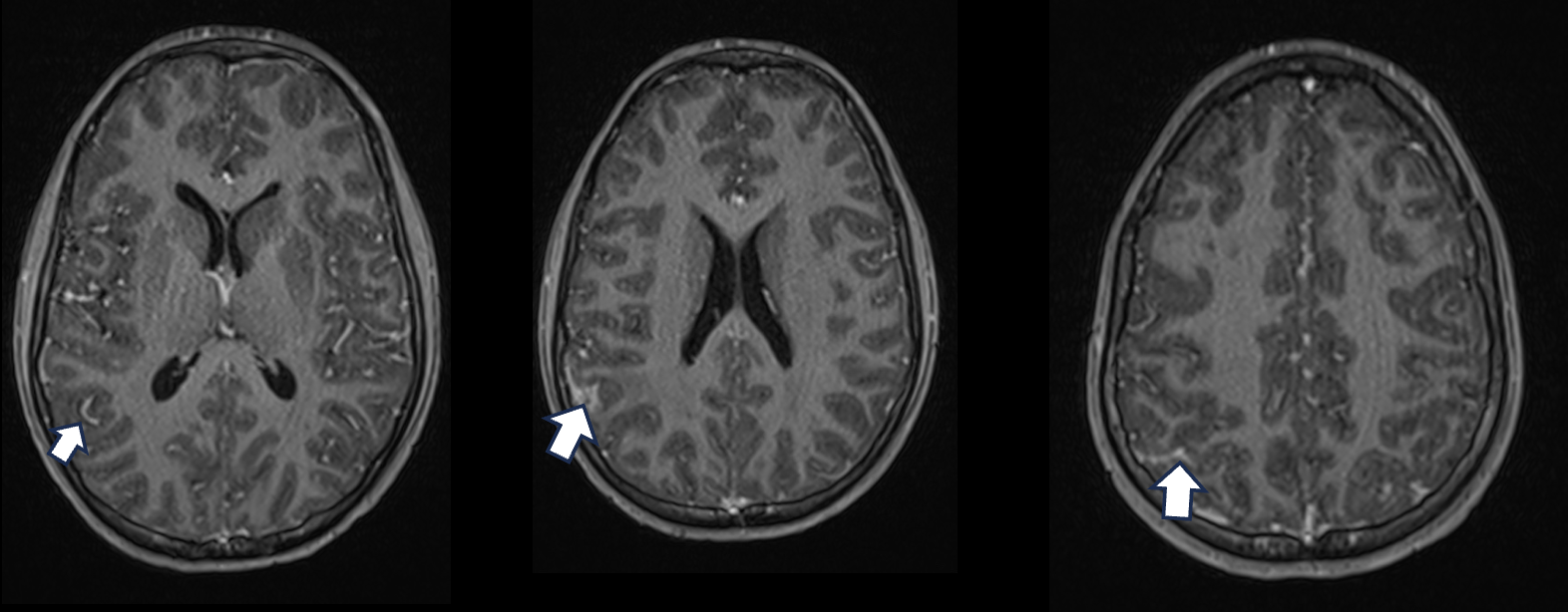
MRI confirmed a left basal ganglia infarct involving the head of caudate and lentiform nucleus. High signal on b1000 DWI with low signal on ADC mapping was in keeping with acute infarct (Figure 2). Additionally, wedge shaped FLAIR high signal was noted in the cortex of the left frontal and right perieto-occipital lobes (Figure 3), which may indicates additional cortical infarcts. Also, high signal in the right mastoid was seen (Figure 4a). Marked basal leptomeningeal enhancement and thickening was noted, more pronounced in the left MCA cistern (Figure 4c). Moreover, patchy leptomeningeal enhancement was also noted in the sulci (Figure 5), particularly in the right perieto-occipital region and left parietal lobe. However, no blood was detected on GRE sequence, excluding sub-arachnoid haemorrhage.Teaching points
- CT brain is very useful as the first examination of choice to identify complications of TB meningitis. However, subtle infarcts and leptomeningeal changes can be difficult to identify and further assessment with MR may be required 6.
- 3D T1-MPRAGE pre- and post-gadolinium sequencing accurately identifies basal leptomeningitis 6.
- T2 FLAIR, DWI and ADC map are useful to identify basal and cortical infarcts as well as differentiate acute from chronic infarcts 7.
- GRE sequencing can be used to demonstrate haemorrhage because it is necessary in the diagnosis of changes in the deep nuclei due to sensitivity to magnetic susceptibilities 8.
Conclusion
This case merits discussion as the early signs of TBM related vasculitis ischemia were initially attributed to the head injury, and prompt treatment of TBM imaging pickup on MRI.Acknowledgements
We thank Zanele Mlilo a Radiographer and Sally Rothemeyer a medical specialist division of neurosurgery from Groote Schuur Hospital, Observatory, Cape Town for support and guidance.References
- Cresswell F V, Davis AG, Sharma K, et al. Recent Developments in Tuberculous Meningitis Pathogenesis and Diagnostics. Wellcome Open Research. Oct 31, 2019;4:164. https://wellcomeopenresearch.org/articles/4-164/v12. Accessed October 31, 2023.
- Thwaites GE, Duc Bang N, Huy Dung N, et al. Dexamethasone for the Treatment of Tuberculous Meningitis in Adolescents and Adults. New England Journal of Medicine. 2004;17. www.nejm.org3. Accessed October 31, 2023.
- Zhang H, Zhang H, Zhang Y, et al. Deep Learning Radiomics for the Assessment of Telomerase Reverse Transcriptase Promoter Mutation Status in Patients With Glioblastoma Using Multiparametric MRI. Journal of Magnetic Resonance Imaging. Nov 1, 2023:4.
- Rohilla R, Shafiq N, Malhotra S. Efficacy and safety of aspirin as an adjunctive therapy in tubercular meningitis: A systematic review and meta-analysis. EClinicalMedicine. Apr 1, 2021:34.
- Wilkinson RJ, Rohlwink U, Misra UK, et al. Tuberculous meningitis. Nature Reviews Neurology. Nature Publishing Group. 2017(13):581-98.
- Jeevanandham B, Kalyanpur T, Gupta P, et al. Comparison of post-contrast 3D-T1-MPRAGE, 3D-T1-SPACE and 3D-T2-FLAIR MR images in evaluation of meningeal abnormalities at 3-T MRI. British Journal of Radiology. 2017;90(1074).
- Schmahmann J.D, Smith E.E, Eichler F.S, et al. Cerebral White Matter. Ann New York Academy Science. 2008;1142:266-309.
- Huang P, Chen K, Liu C, et al. Visualizing Cerebral Small Vessel Degeneration During Aging and Diseases Using Magnetic Resonance Imaging. Journal of Magnetic Resonance Imaging. John Wiley and Sons Inc; 2023.
- Paprocka J, Machnikowska-Sokołowska M, Gruszczyńska K, et al. Neuroimaging of basal ganglia in neurometabolic diseases in children. Brain Sciences. MDPI AG; 2020; 10:116.
Figures