5190
Combining 7T and 3T MRI in Epilepsy Diagnosis: A Collaborative Approach to Enhance Surgical Decision-Making1Translational Imaging Center, Houston Methodist Hospital, Houston, TX, United States, 2MRI Core Laboratory, Houston Methodist Hospital, Houston, TX, United States, 3Department of Radiology, Houston Methodist Hospital, Houston, TX, United States, 4Department of Neurology, Houston Methodist Hospital, Houston, TX, United States
Synopsis
Motivation: Epilepsy can be imaged at 3T utilizing typical imaging sequences, but improved quality and resolution can be achieved using 7T, enabling better detection of lesions and subsequently better chances of a successful treatment outcomes.
Goal(s): Provide higher quality images for patients with epilepsy on 7T.
Approach: 146 patients were evaluated for epilepsy using 7T MRI. Among these, 117 patients also had prior 3T MRI for comparison.
Results: Combining 3T and 7T MRI has demonstrated promise in improving the diagnostic and surgical decision-making process for epilepsy patients for our neurologists and neurosurgeons.
Impact: In conjunction with 3T imaging, our findings at 7T consistently detect a greater number of lesions in epilepsy patients, resulting in greater confidence in localizing and characterizing lesions that were questionable or not identified at 3T.
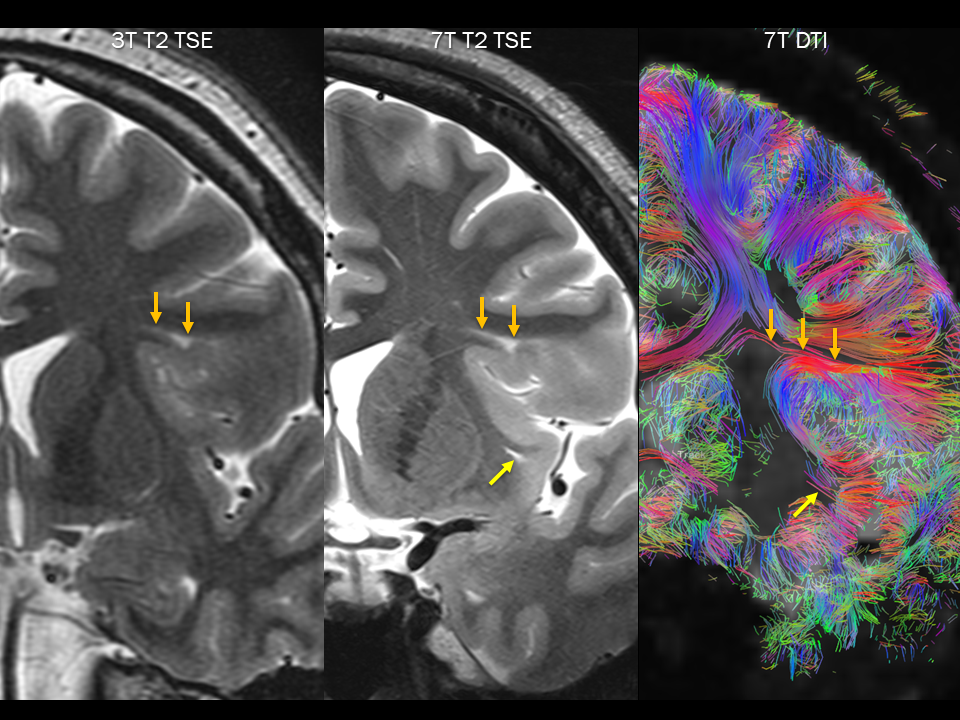
Method: Between September 2019 and October 2023, 146 patients (ages 20-84, M:F 0.46) evaluated for epilepsy had brain MRI using 7T clinical scanner (Siemens MAGNETOM Terra) with 1Tx/32Rx head coil (Nova Medical). Among these, 117 patients also had prior brain MRI using 3T clinical scanner (mostly GE Discovery MR750 or Siemens MAGNETOM Skyra) available for comparison. Sequences used for 7T brain MRI include sagittal 3D T1 MP2RAGE, axial pre- and postcontrast 3D T1 MPRAGE, axial and coronal T2 TSE, axial and coronal T2 FLAIR, axial T2* SWI, sagittal 3D T2 SPACE, sagittal 3D T2 FLAIR SPACE, and axial DTI with 30 diffusion gradient directions. Acquired voxel size was sub-mm in-plane and 2-mm slice thickness for 2D sequences and 0.7-mm all dimensions for 3D sequences. Images from all sagittal-acquired 3D sequences were reformatted into axial and coronal planes with 0.7-mm isometric voxel size. Total scan time was approximately 1hour. Images were visually evaluated for artifacts, spatial resolution, SNR, CNR, conspicuity and characterization of lesions, cortical and subcortical structures including hippocampal anatomy, and overall image quality.
Results: Our findings indicate that 7T MRI, when used in conjunction with 3T MRI, consistently helps to detect a greater number of lesions in epilepsy patients. Lesions detected include mesial temporal sclerosis, focal cortical dysplasia, subependymal and subcortical heterotopia, polymicrogyria, low-grade glial and glioneuronal tumors such as DNET and MVNT, abnormal brain iron accumulation, microhemorrhage from various etiologies, cavernous and other vascular malformations. Spatial resolution, SNR, conspicuity and characterization of most lesions, and evaluation of cortical and subcortical structures including hippocampal anatomy are vastly superior with 7T MRI, resulting in greater confidence in localizing and characterizing lesions that were questionable on 3T MRI and finding additional lesions not identified on 3T MRI. MP2RAGE on 7T MRI is particularly helpful in evaluating gyral pattern, cortex, gray-white matter interface, gray matter heterotopia. SWI on 7T MRI is extremely sensitive for detecting abnormal brain iron accumulation, microhemorrhage, vascular malformations. However, 7T MRI with 1Tx/32Rx head coil consistently showed artifacts with signal loss along the ventral temporal lobes, inferior brainstem, cerebellum, and surrounding skull base structures, limiting lesion detection in these regions, such as temporal encephaloceles, which are better visualized on 3T MRI. Some T2 FLAIR hyperintense lesions on 3T MRI, most notably involving cortices, are less conspicuous with lower CNR on 7T MRI. Despite some of these limitations, results from 7T MRI did not produce false-positive findings and in most cases helped to enhance the reliability of the diagnostic process.
Conclusion: Combining 7T and 3T MRI has demonstrated promise in improving the diagnostic and surgical decision-making process for epilepsy patients for our neurologists and neurosurgeons. By accurately identifying and characterizing lesions and minimizing false positives, this approach offers a greater opportunity for success in surgical interventions. Nevertheless, the ongoing challenge of signal loss along the ventral temporal lobes, inferior brainstem, cerebellum, and surrounding skull base structures as well as decreased conspicuity of some T2 FLAIR hyperintense lesions underscores some limitations of 7T MRI at its present state of development.
Acknowledgements
No acknowledgement found.References
De Ciantis, A., Barba, C., Tassi, L., Cosottini, M., Tosetti, M., Costagli, M., ... & Guerrini, R. (2016). 7T MRI in focal epilepsy with unrevealing conventional field strength imaging. Epilepsia, 57(3), 445-454.
Opheim, G., van Der Kolk, A., Bloch, K. M., Colon, A. J., Davis, K. A., Henry, T. R., ... & Guye, M. (2021). 7T epilepsy task force consensus recommendations on the use of 7T MRI in clinical practice. Neurology, 96(7), 327-341.
Figures