5188
Exploring the therapeutic benefits of aromatherapy compared traditional medicine for patients undergoing Cardiac Magnetic Resonance Imaging.1Imaging Institute, Cleveland Clinic, Cleveland, OH, United States, 2Cardiovascular Innovation Research Center, Heart Vascular and Thoracic Institute, Cleveland Clinic, Cleveland, OH, United States, 3Cardiovascular Medicine, Cleveland Clinic, Cleveland, OH, United States, 4Cardiovascular Medicine, Heart Vascular and Thoracic Institute, Cleveland Clinic, Cleveland, OH, United States, 5Biomedical Engineering, Case Western Reserve University and Cleveland Clinic, Cleveland, OH, United States
Synopsis
Keywords:
Motivation: Many individuals undergoing MRI scans experience claustrophobia. The resulting anxiety often leads to reduced image quality and even the abandonment of exams.
Goal(s): Our goal is to use aromatherapy in a comprehensive stress reduction approach that we’ve developed to help improve MRI image quality, decrease nursing intervention and improve patient experience.
Approach: More than 300 patients were involved in retrospective and prospective studies offering aromatherapy and alprazolam for anxiety during Cardiac MRI.
Results: Aromatherapy was associated with improved image quality compared to alprazolam and was a strong predictor of reduced scan duration, nursing time, and number of repeat images.
Impact: Aromatherapy has the ability to mitigate anxiety during MRI scans for patients with claustrophobia, yielding improved quality images and reduced scan time. As a result, implementation of aromatherapy has the ability to improve patient experience and clinical outcomes.
Background
Anxiety and claustrophobia affect 12.5% of the population, impacting the ability for patients to tolerate cardiac MRI scans (CMR)1-3. We hypothesized that a comprehensive approach to stress reduction including olfactory system stimulation with lavender oil and aromatherapy relaxation techniques (AROM) would improve scan tolerability compared to benzodiazepines4. The sedative effect of benzodiazepines can decrease the ability for patients to perform adequate breath holding, often leading to repeat image acquisitions5. Additional monitoring is also required5. We sought to determine the impact of AROM on scan time, repeat image acquisitions, early scan termination, and nursing monitoring time.Methods
We conducted prospective and retrospective studies in patients undergoing CMR scans on Philips 1.5 and 3T scanners and receiving anxiolytic therapy (AROM, alprazolam (ALP), or a combination of AROM plus ALP (COMBO)). The retrospective and prospective studies were conducted on 145 and 155 patients, respectively, with approval of the Cleveland Clinic IRB. Patients receiving aromatherapy underwent personalized coaching and lavender oil, while patients receiving alprazolam were medicated prior to scanning. Participants in the prospective study completed a survey regarding their anxiety level and experience. In the retrospective study, image quality was rated from 1-4 (1=poor, 2=fair, 3=good, 4=excellent) by an experienced level III trained cardiovascular radiologist blinded to the type of anxiolytic therapy. For both studies, a multiple-variable linear regression determined predictors of scan duration. In the prospective study, multiple-variable ordinal and linear regression models were used to determine independent predictors of repeat image acquisitions and nursing time.Results
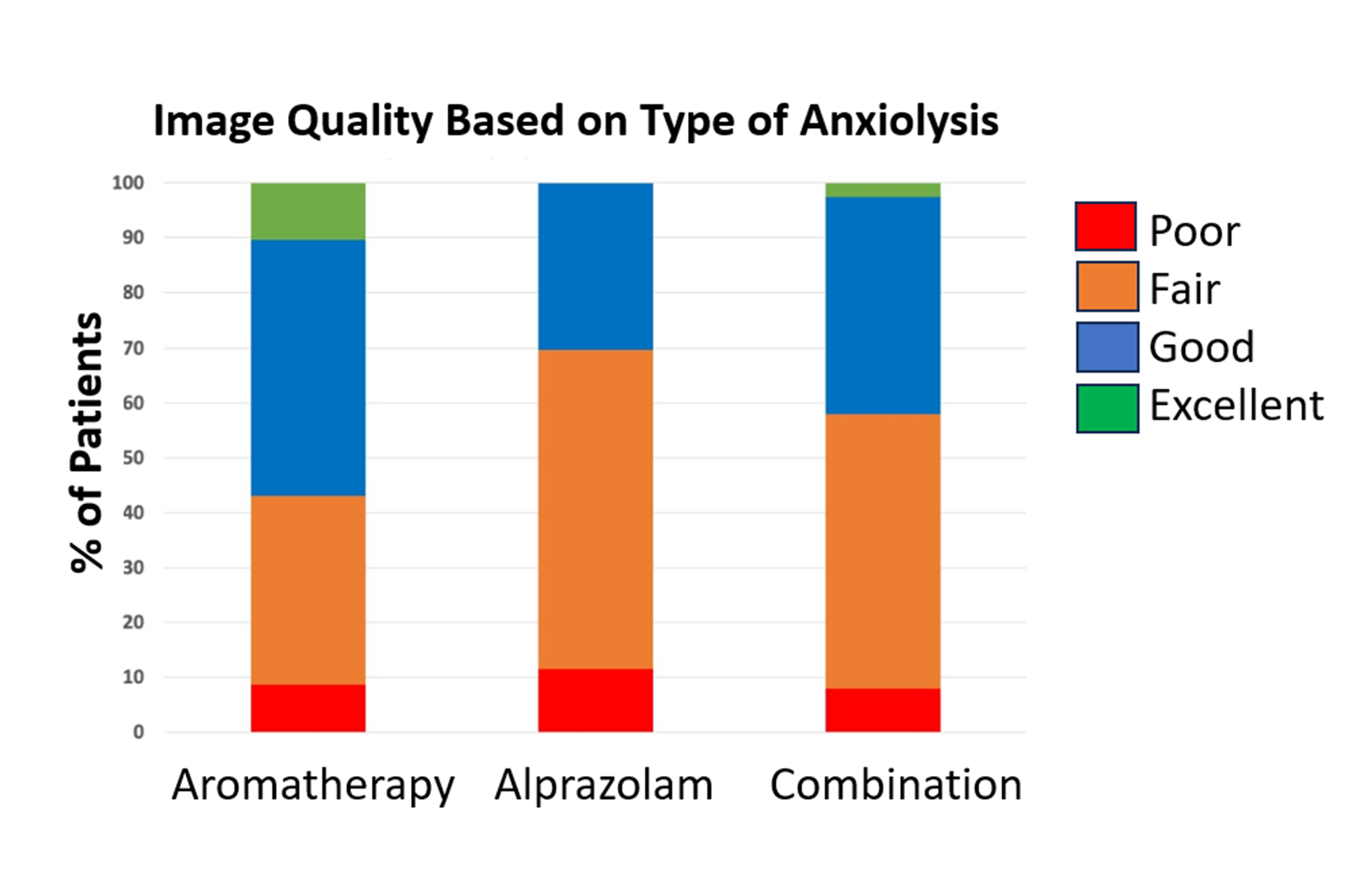
Retrospective Study:Mean age differed significantly across groups receiving anxiolysis (p=0.001): 49.5±18.2 years old (N=61, aromatherapy), 60.2±14.9 (N=45, alprazolam), and 60.3±13.7 (N=39, combined). There were no statistically significant differences in the three groups based on sex, race, or BMI. Figure 1 displays image quality scores categorized by type of intervention received. The aromatherapy group had the highest percentage of cases with good-to-excellent scores, and the lowest percentage of cases with poor scores.
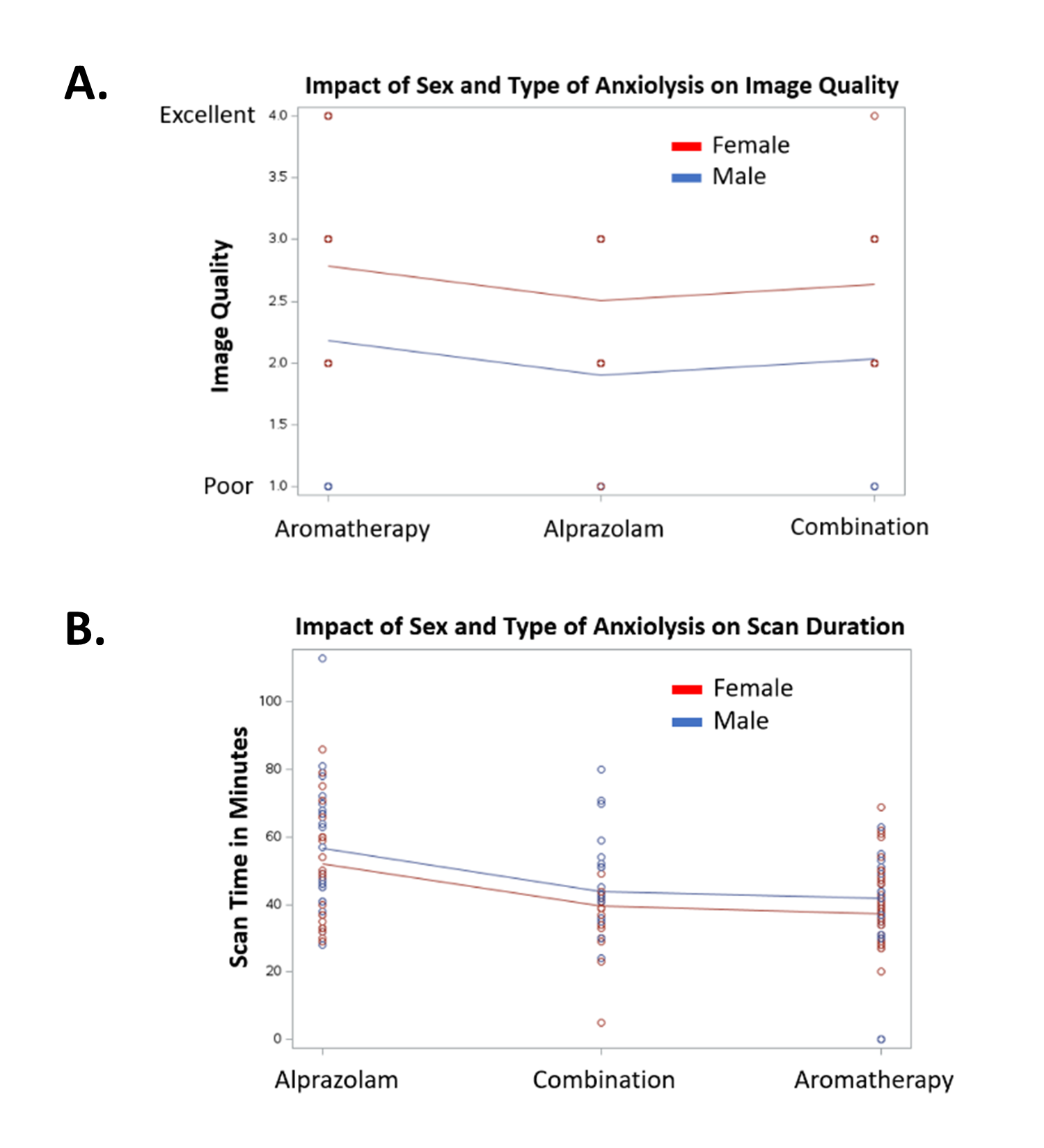
The impact of sex and type of anxiolysis on image quality and scan duration are presented in Figure 2. BMI (p=0.222) was not a significant predictor of image quality. Female sex was a significant independent predictor of higher image quality (p<0.001) and tended to result in lower scan time (p=0.094). There was a trend for better image quality for younger patients (p=0.065). After adjusting for age, sex, and BMI, type of anxiolysis was not a significant predictor of image quality (p=0.460), but aromatherapy and combination therapy were predictive of significantly shorter scan times (p<0.001)
Prospective Study:
Mean age differed significantly across the groups receiving anxiolytics (p=0.03): 51.4±16.8 years old (N=107, AROM), 65.9±11.9 (N=7, ALP), and 57.3±12.3 (N=21, COMBO). There were no statistically significant differences in the three groups based on sex or BMI.
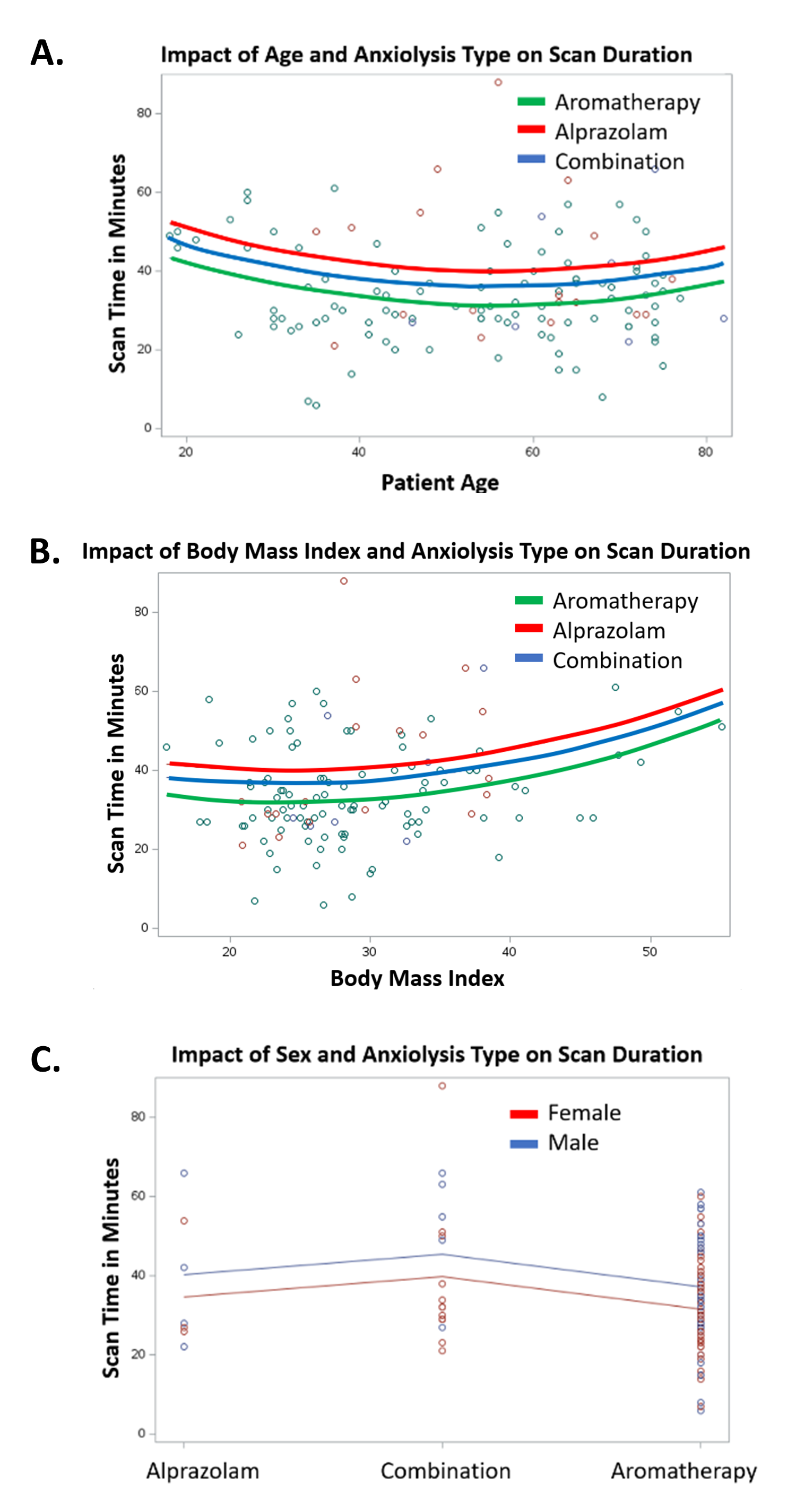
Female sex (p=0.028) and lower BMI (p=0.012) were significantly associated with shorter scan times. After adjusting for age, sex, and BMI, there was a significant reduction in scan time for AROM compared to COMBO (p=0.01) (See Figures 3A-C).
Early termination of CMR due to anxiety occurred in 4 patients and was not significantly associated with anxiolysis type (p=0.810). Repeat images were required as follows: AROM n=25 (26.6%), ALP n=5 (71.4%) and COMBO n=4 (20%). BMI (p=0.386), age (p=0.337), and sex(p=0.269) were not significant predictors of repeat imaging, but AROM and COMBO were significantly associated with decreased repeat imaging compared to ALP (p=0.041).
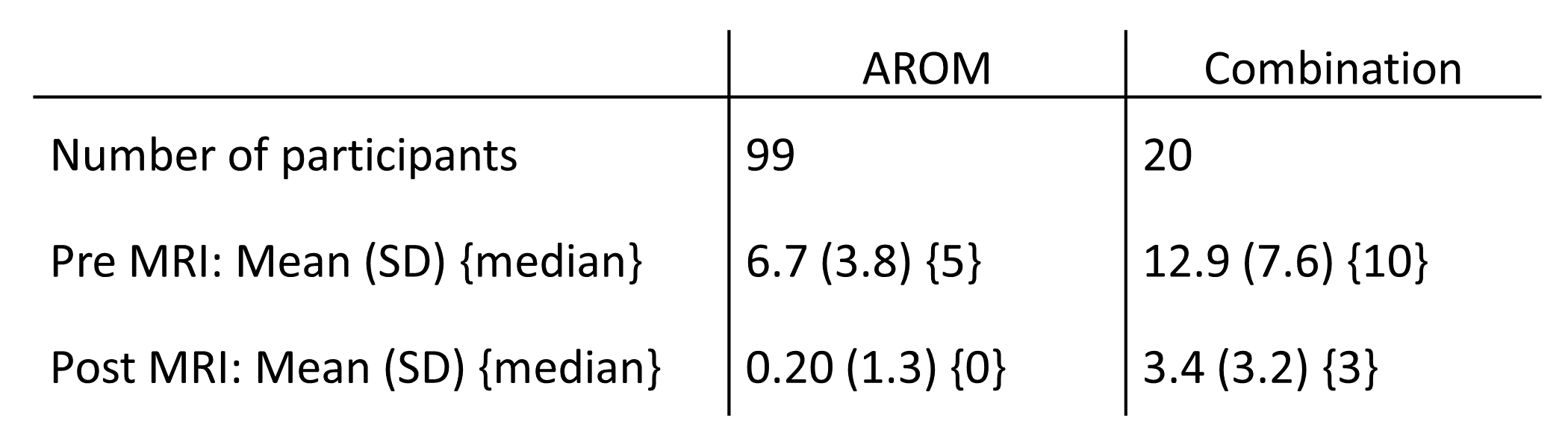
Duration of nursing time monitoring patients pre and post MRI based on anxiolysis type is listed in Table 1. BMI (p=0.474), age (p=0.364), and gender (p=0.703) were not significant predictors of nursing time, but AROM was a significant predictor of decreased nursing time (p<0.001).
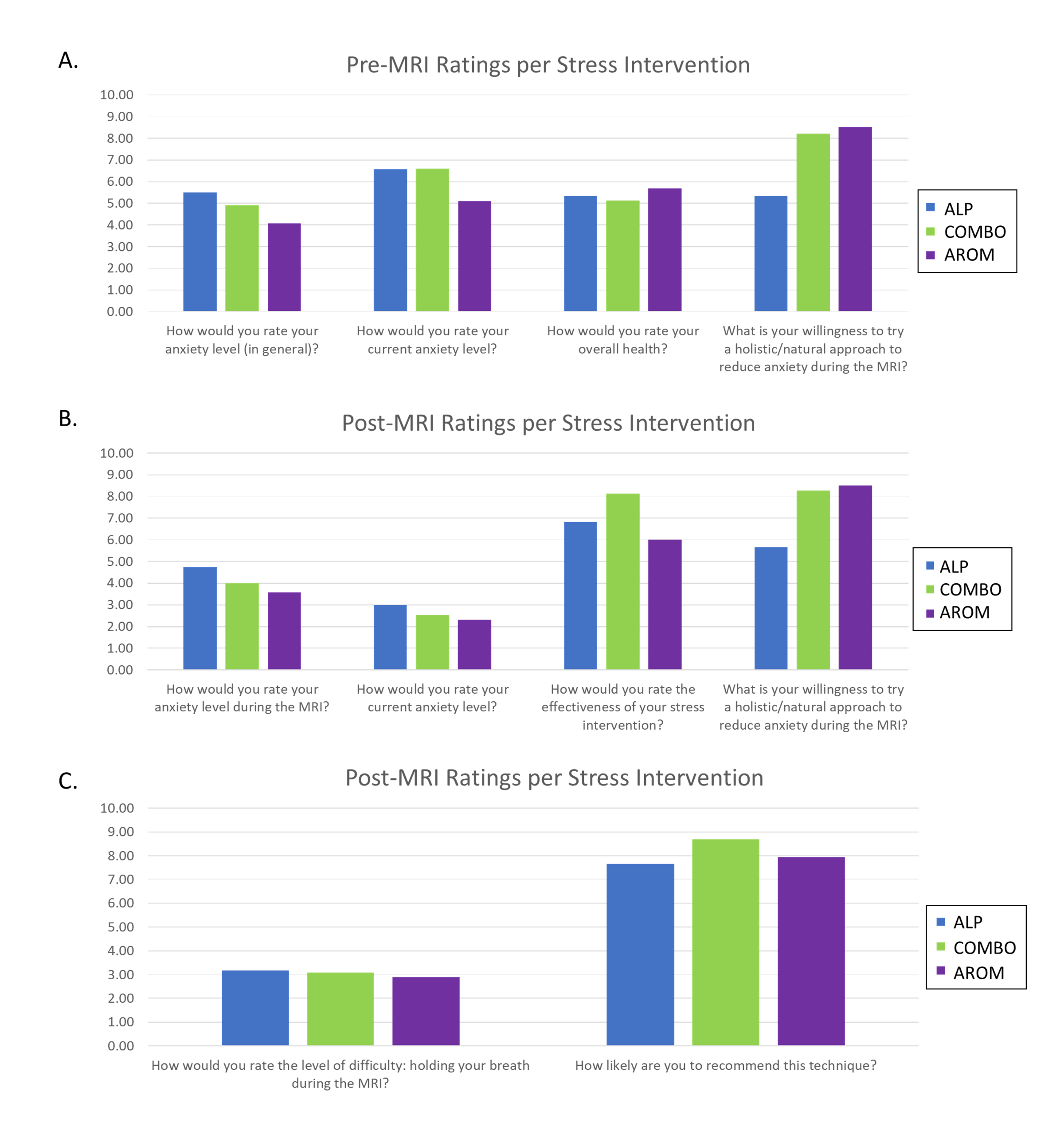
The results of the patient experience survey are presented in Figure 4. Before and during the MRI, patients that opted for ALP generally rated their anxiety level highest , while patients that opted for AROM generally rated their anxiety level lowest. All anxiolytic therapies were rated as effective, with average scores of 6 or greater out of 10, and COMB patients rating their therapy as most effective.
Conclusion
Our study suggests that AROM is an effective non-sedating anxiolytic, with comparably low rates of early CMR termination compared to ALP. AROM showed significant associations with a reduced number of repeat imaging compared to ALP, and shorter scan time and nursing monitoring time compared to COMBO. Our findings highlight the potential benefits of AROM on operational throughput and nursing interventions. While aromatherapy was associated with improved image quality in univariate analysis, female sex was the strongest predictor of higher image quality. AROM remained a strong predictor of shorter scan duration.Acknowledgements
I wanted to take a moment to express my sincere gratitude for the support from the Imaging Institute and funding from the Catalyst grant.References
1. Francis JM, Pennell DJ. Treatment of claustrophobia for cardiovascular magnetic resonance: use and effectiveness of mild sedation. J Cardiovasc Magn Reson. 2000;2:139-141. doi: 10.3109/10976640009148683
2. Hudson DM, Heales C, Vine SJ. Radiographer Perspectives on current occurrence and management of claustrophobia in MRI. Radiography (Lond). 2022;28:154-161. doi: 10.1016/j.radi.2021.09.008
3. Madl J, Janka R, Bay S, Rohleder N. MRI as a Stressor: The Psychological and Physiological Response of Patients to MRI, Influencing Factors, and Consequences. J Am Coll Radiol. 2022;19:423-432. doi: 10.1016/j.jacr.2021.11.020
4. Gong M, Dong H, Tang Y, Huang W, Lu F. Effects of aromatherapy on anxiety: A meta-analysis of randomized controlled trials. J Affect Disord. 2020;274:1028-1040. doi: 10.1016/j.jad.2020.05.118
5. Hirschtritt ME, Olfson M, Kroenke K. Balancing the Risks and Benefits of Benzodiazepines. JAMA. 2021;325:347-348. doi: 10.1001/jama.2020.22106
Figures