5168
The future role of MRI in confirming and monitoring multiple sclerosis diagnosis without intravenous administration of GBCAs.1Faculty of Health and Wellness Sciences, Cape Peninsula University of Technology, Cape Town, South Africa, 2Faculty of Human Biology, University of Cape Town, Cape Town, South Africa, 3Division of Chemical Pathology,Department of Pathology,Faculty of Medicine&Health Sciences, Stellenbosch University, Cape Town, South Africa, 4Department of Medical Imaging & Therapeutic Sciences, Faculty of Health & Wellness Sciences, Cape Peninsula University of Technology, Cape Town, South Africa, 5Medical Imaging, Department of Health and Care Professions, Faculty of health and Life Sciences, University of Exeter, South Cloisters, United Kingdom, 6Department of Human Biology, University of Cape Town, Cape Town, South Africa, 7Division of Chemical Pathology,Department of Pathology,Faculty of Medicine & Health Sciences, Stellenbosch University, Cape Town, South Africa, 8Department of Internal Medicine, Faculty of Medicine & Health Sciences, Stellenbosch University, Cape Town, South Africa, 9Department of Paediatrics & Child Health, Faculty of Medicine & Health Sciences, University of Stellenbosch, Cape Town, South Africa
Synopsis
Keywords:
Motivation: Multiple sclerosis (MS) is a chronic inflammatory disease affecting the central nervous system (CNS). MS diagnosis needs the objective assessment of white matter (WM) lesions as they disseminate both in space and time.
Goal(s): More refined MRI sequences have vastly improved the characterisation of brain volume and focal white matter lesions.
Approach: In this study, MRI scans were obtained of 25 adult females diagnosed with relapsing remitting MS and 25 control subjects without MS.
Results: Data collected shows a clear distinction between the lesion volumes from the two groups and enhances the validity of MRI and its potential clinical applicability.
Impact: The high costs and chance of allergic reactions to GBCAs may impose limitations within the patient’s treatment plan. Our study reaffirms the value of MRI without the use of GBCAs and demonstrates its potential for long-term monitoring of MS.
Introduction
Multiple sclerosis (MS), is a major cause of neurological disability amongst young adults, affecting almost 2.3 million people worldwide, each year (2). Monitoring the disease process over time is challenging, therefore in this context a need arises for a reliable biomarker/ tool such as Magnetic Resonance Imaging (MRI), which aids early diagnosis to enable better disease management, facilitate monitoring disease progression over time, and allows therapeutic intervention when maximum potential impact is possible. This idea has also been endorsed by both the 2015 Magnetic Resonance Imaging in Multiple Sclerosis (MAGNIMS)1,2 and 2016 Consortium of Multiple Sclerosis Centres (CMSC), and further validates MRI’s strength(3). Innovative postprocessing tools, such as lesion inpainting algorithms, regional voxel-wise approaches, and composite MRI scales, enable a better assessment of global and regional white and grey matter damage in MS. These methods offer a new pathway linking MS with its clinical status (4).Gadolinium-based contrast agents
The use of Gadolinium-based contrast agents (GBCAs) is in general considered to be safe, however in 2006 a strong link between Gd(III)-based contrast agents and a devastating disease termed nephrogenic systemic fibrosis (NSF) was identified in a renally impaired patient (5). Recent evidence suggests that GBCAs have a tendency to accumulate within the brain, with associated cognitive deficits especially after repeated exposure to GBCAs (6,7) . Nevertheless, these contrast agents are widely used within both clinical and research settings. During a relapse, the contrast agent gains entry through the blood-brain barrier, and within active lesions the T1 relaxation times of the water protons near the agent are shortened, and images of tissues with a higher concentration are brighter than those with a lower concentration. We aimed to put together an optimized imaging protocol that would enable diagnosis and monitoring of MS lesions without the need for GCBAs.
Methods
We enrolled 25 participants with a confirmed diagnosis of MS, and 25 age- and sex-matched healthy controls whom all had a MRI scan using a 3T Siemens Skyra scanner (Erlangen, Germany). Of these, 8 participants (3 MS diagnosed and 5 controls) did not attend their MR scan appointment for various reasons. The protocol used included the Fluid Attenuated Inversion Recovery (FLAIR) in axial and sagittal planes, Proton Density (PD) and T2 imaging (in coronal plane), Magnetisation Prepared Rapid Gradient Echo Imaging (MPRAGE), susceptibility weighted imaging (SWI), Diffusion Tensor Imaging (DTI), and Resolve images were utilised for the lesion count.Results
1.Figure 1a, b, our T1 sequence showed the ability to demonstrate cortical lamination.2.Figure 2a shows improved visibility of MS plaques, and figure 2b demonstrates regions of restricted diffusion as seen on our apparent diffusion coefficient sequence.
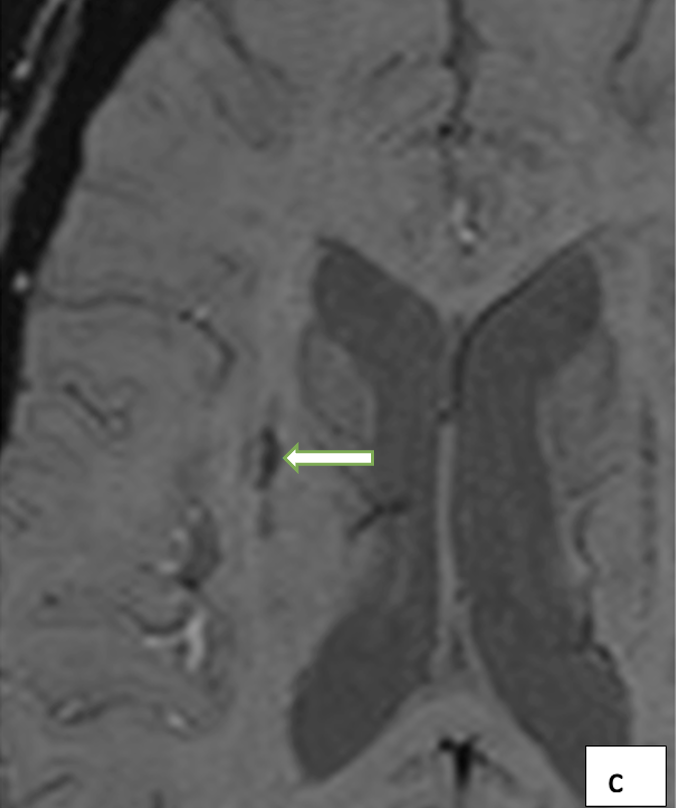
3.Disease activity was demonstrated in a patient who was scanned during a relapse without the need for gadolinium contrast (Figure 1c, d).
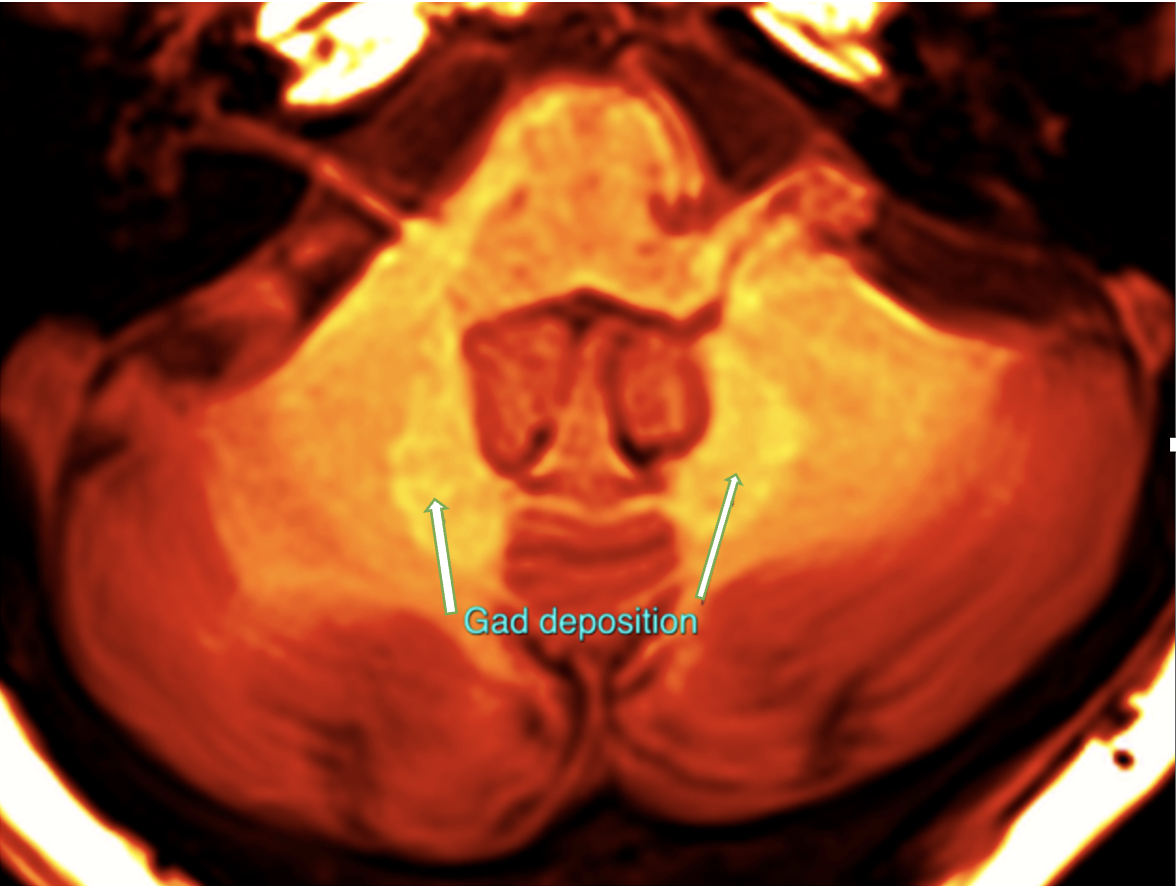
4.One MR image demonstrated gadolinium deposits deep within the brain (Figure 3).
5.Lesions were found in 5 of the controls as well.
Discussion
Our protocol allowed for the following:·Increased spatial resolution, revealing minute differences between adjacent structures on T1-weighted imaging;
A clear delineation between anatomical structures on FLAIR and ADC images;
Excellent contrast between white and grey matter, as well as excellent lesion visibility and conspicuity on FLAIR;
Good contrast; and cortical lamination on T1-weighted MPRAGE;
Ability to image an active lesion during a relapse without gadolinium contrast using SWI.
Conclusion
MRI is continuously evolving and has proven to be a modality that plays an integral and pivotal role in the diagnosis and monitoring of pathologies in the brain.Acknowledgements
I would like to acknowledge Dr. Coenie Hattingh, who helped to get this project going and thanking him for always being available to assist me with any queries.References
References
1. Cahalane AM, Kearney H, Purcell YM, McGuigan C, Killeen RP. MRI and multiple sclerosis––the evolving role of MRI in the diagnosis and management of MS: the radiologist’s perspective. Ir J Med Sci. 2018;187(3):781–7.
2.Sormani MP, De Rossi N, Schiavetti I, Carmisciano L, Cordioli C, Moiola L, et al. Disease-Modifying Therapies and Coronavirus Disease 2019 Severity in Multiple Sclerosis. Ann Neurol. 2021 Apr 1;89(4):780–9.
3.Wattjes MP, Steenwijk MD, Stangel M. MRI in the Diagnosis and Monitoring of Multiple Sclerosis: An Update. Clin Neuroradiol. 2015 Oct 30;25:157–65.
4.Ceccarelli A, Bakshi R, Neema M. MRI in multiple sclerosis: A review of the current literature. Curr Opin Neurol. 2012;25(4):402–9.
5.Wahsner J, Gale EM, Rodríguez-Rodríguez A, Caravan P. Chemistry of MRI contrast agents: Current challenges and new frontiers. Vol. 119, Chemical Reviews. American Chemical Society; 2019. p. 957–1057.
6.Gulani V, Calamante F, Shellock FG, Kanal E, Reeder SB. Gadolinium deposition in the brain: summary of evidence and recommendations [Internet]. Vol. 16, Personal View Lancet Neurol. 2017. Available from: www.thelancet.com/neurology.
7.Forslin XY, Shams XS, Hashim XF, Aspelin XP, Bergendal XG, Martola XJ, et al. Retention of Gadolinium-Based Contrast Agents in Multiple Sclerosis: Retrospective Analysis of an 18-Year Longitudinal Study. [cited 2021 May 31]; Available from: http://dx.doi.org/10.3174/ajnr.A5211.
Figures
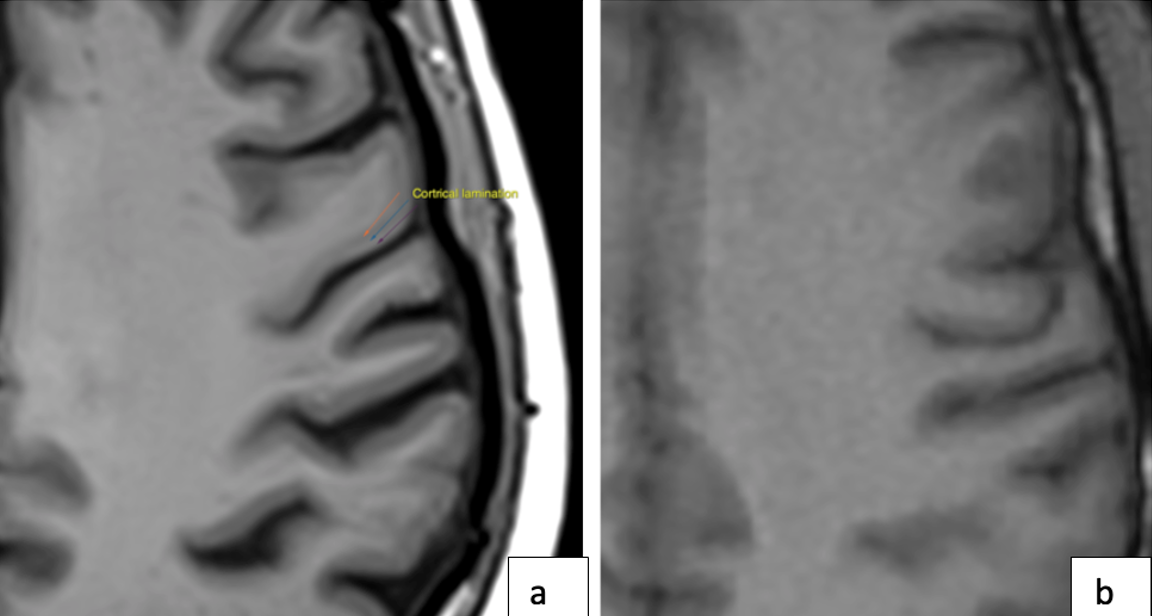
Figure 1a:Our T1 sequence approaches MR microscopy with its ability to demonstrate cortical lamination.
Figure 1b:Conventional T1 sequence.
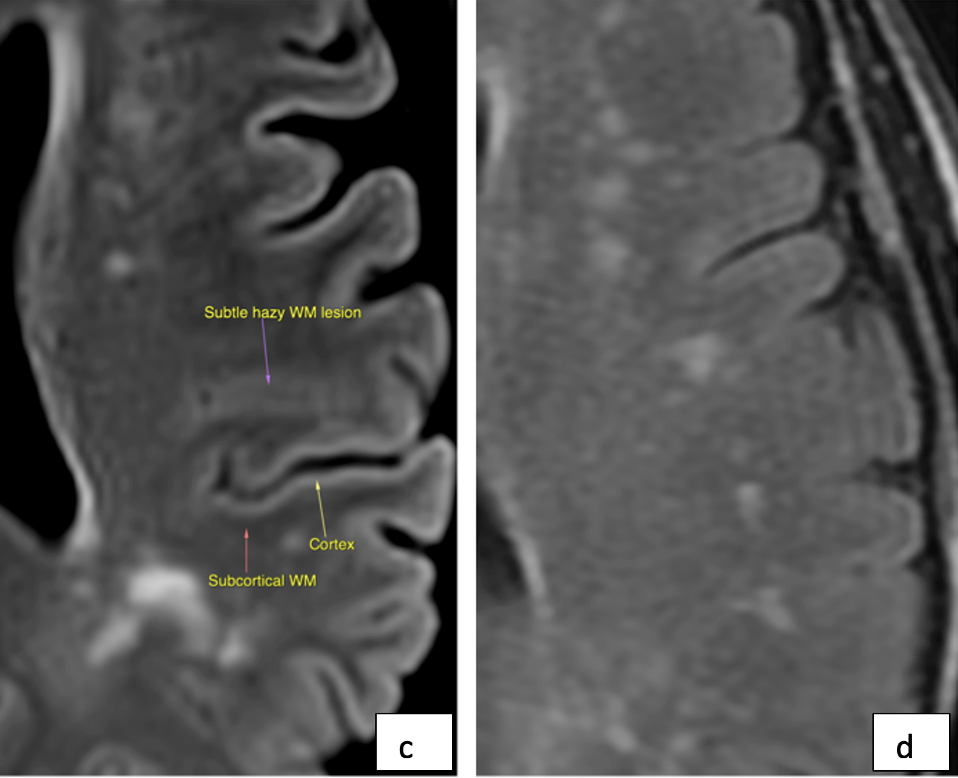
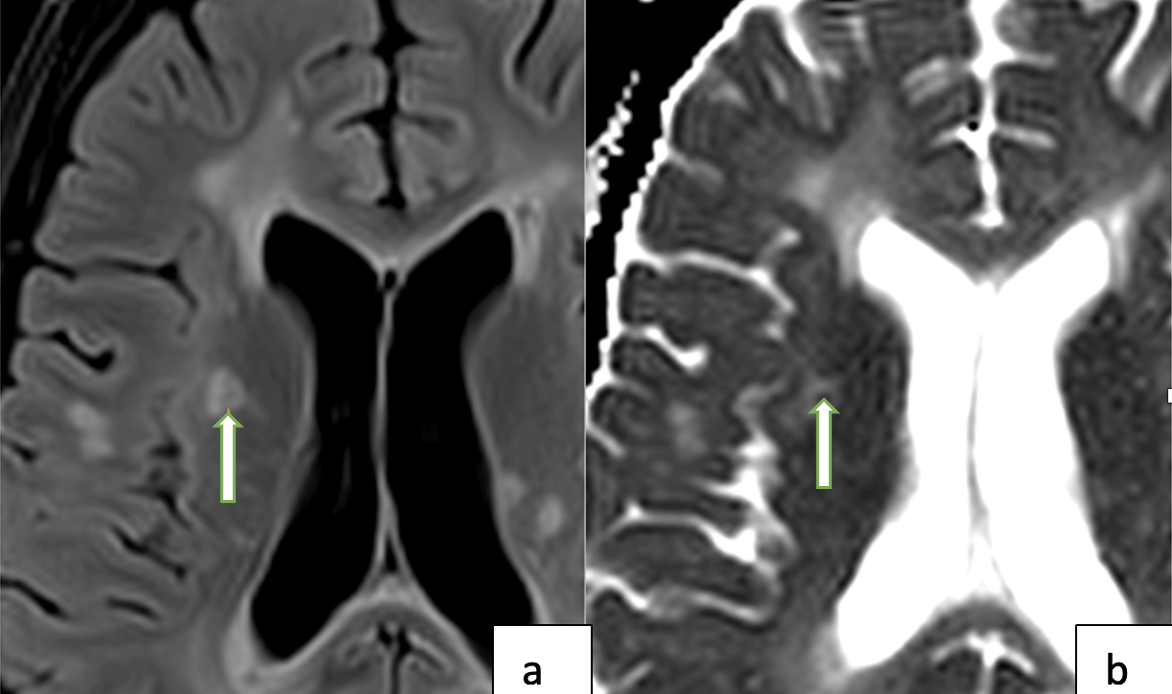
Figure 2a: Our FLAIR sequence demonstrates the appearance of MS plaques.
Figure 2b: Our apparent diffusion coefficient sequence shows a central region of restricted perfusion as seen on.The central low signal region is associated with active inflammation and consequent cellular swelling.