5146
3DMRCP Quantitative Image Quality: A Comparison Between CS-SENSE And SENSE And Its Acquisition Time1Diagnostic Radiology, Tan Tock Seng Hospital, Singapore, Singapore
Synopsis
Keywords:
Motivation: Upgrading of MR scanner with compressed sensing (CS) could reduce acquisition time. Image quality of 3DMRCP with CS, however, need to be assessed quantitatively to ensure its standard despite of acceleration.
Goal(s): We aimed to prove that 3DMRCP with CS can be employed in clinical practice with comparable quantitative image quality to SENSE and with shorter acquisition time.
Approach: Quantitative image quality (signal intensity, noise, SNR and CNR) of 3DMRCP with CS and SENSE of the same subject that acquired at two different timepoints were compared retrospectively.
Results: 3DMRCP with CS have maintained the quantitative image quality and has a shorter scan duration.
Impact: 3DMRCP with CS only not can achieve higher spatial resolution but also with a shorter acquisition time while maintaining its quantitative image quality. Therefore, 3DMRCP with CS is recommended to be adopted in daily clinical practice.
Background
Compressed sensing (CS) is a relatively new strategy for scan acceleration in MRI which initiated by the concept that no important information is lost on a compressed image. Thus, it is unnecessary to fully sample all data points because some of these are negligible. This idea is then applied reversely, whereby image reconstruction is performed on a compressed k-space data.1-2 For successful CS application, there are three requirements to be fulfilled, which are transform sparsity, incoherence of undersampling artefact and application of iterative reconstruction.2 As MRCP representation is sparse in pixel domain, CS application in MRCP is hence possible to reduce imaging time via balance variable density data undersampling followed by a non-linear reconstruction.3-5 A drop in acquisition time has a positive impact in minimising the presence of respiratory and motion artefacts, which improve image quality eventually. Therefore, this study is carried out to compare quantitative image quality of respiratory triggered 3DMRCP with SENSE (s3DMRCP) and CS (cs3DMRCP). We hypothesize that cs3DMRCP is able to maintain or improve image quality compared to s3DMRCP with shorter acquisition time.Methodology
Both cs3DMRCP and s3DMRCP sequences were performed on 1.5T MR scanner (Ingenia, Philips Healthcare) with 16-channel body coil and built-in spine coil. A total of 50 subjects (24 males and 26 females) with mean age of 74±10 years old who underwent s3DMRCP from April 2017 to December 2022 were identified. Second set of data was collected from March to July 2023 when these patients presented for follow-up scans with cs3DMRCP. Retrospective comparison was made between s3DMRCP and cs3DMRCP of the same subject that was acquired at different time points by using the same scanner.MR acquisition
Both 3DMRCP sequences were respiratory triggered and acquired at the end of respiratory phase with a trigger delay of 200ms. Three-dimensional turbo spin echo (3DTSE) pulse sequence was applied in coronal oblique plane. cs3DMRCP was acquired with FOV 360x320mm, pixel size 1x1mm, matrix 360x320, slice thickness 2.6mm, TR 1362ms, TE 600ms and CS-SENSE factor 4, while s3DMRCP was acquired with FOV 350x310mm, pixel size 1.1x1.1mm, matrix 320x282, slice thickness 2.6mm, TR 1362-2030ms, TE 600ms and SENSE factor 2.Quantitative image quality analysis
Quantitative image quality parameters were measured for all subjects on both images by using Centricity Universal Viewer (General Electric Healthcare, the USA). A single radiographer with 5 years of working experience in MRI had performed all the quantitative measurements. One circular region-of-interest (ROI) was placed in the centre of CBD to encompass the whole duct while ROI of the periductal tissue was placed next to the ROI of CBD. (Figure 1) All ROI placements were made in the region that appears homogeneous, artefact- and pathology-free. Quantitative image quality, including signal intensity, noise, signal noise ratio (SNR) and contrast noise ratio (CNR) were quantified. Signal intensity and noise were defined as the mean and standard deviation (SD) of the ROI, respectively. SNR and CNR were calculated by using the formulas $$$SNR = \frac{Signal Intensity_{CBD}}{Noise_{CBD}}$$$ and $$$CNR = \frac{Signal Intensity_{CBD}-SignalIntensity_{PeriductalTissue}}{Noise_{CBD}}$$$.Statistical analysis
All statistical analyses were performed using SPSS software version 28.0 (SPSS Inc., the USA). Median of quantitative image quality parameters and acquisition time were presented. Wilcoxon signed-rank test was performed for comparison of signal intensity, noise, SNR, CNR, and acquisition time between cs3DMRCP and s3DMRCP. p-value of <0.05 was considered statistically significant.Results
There were no significant differences in all quantitative image quality. Both s3DMRCP and cs3DMRCP had almost identical signal intensity on CBD (cs3DMRCP: 2023.00 vs. s3DMRCP: 2028.00, p=0.675). However, s3DMRCP had slightly higher CBD noise compared to cs3DMRCP (cs3DMRCP: 240.00 vs. s3DMRCP: 291.50, p=0.342). This led to a marginally higher SNR in cs3DMRCP due to higher noise in s3DMRCP (cs3DMRCP: 8.10 vs. s3DMRCP: 7.26, p=0.466). A higher CNR was also observed in cs3DMRCP (cs3DMRCP: 7.64 vs. s3DMRCP: 6.68, p=0.484). Regarding acquisition time, a significant difference between the two sequences (p-value <0.001) was observed, with cs3DMRCP and s3DMRCP recorded a median time of 90s and 129s, respectively.Discussion
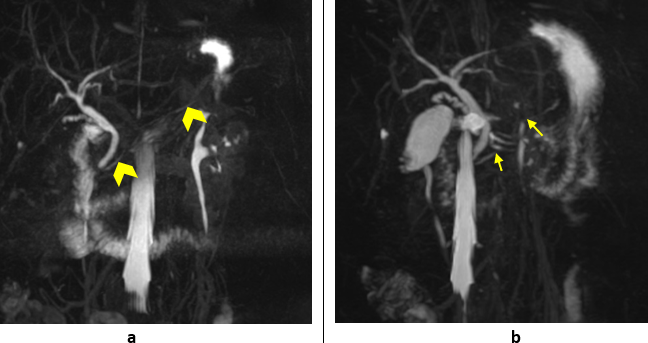
Critically ill patients are commonly associated with motion artefacts due to long scan duration caused by irregular respiration and result in degraded image quality,6 thus cs3DMRCP with shorter acquisition time would be advantageous for these patients. (Figure 2) Additionally, higher spatial resolution imaging with shorter scan time allows radiologists to rule out pathology precisely and prevent patients from unnecessary follow-up. (Figure 3)Conclusion
Current study showed that respiratory triggered cs3DMRCP has an improved image quality in terms of spatial resolution with comparable quantitative image quality with s3DMRCP. It is recommended that CS-SENSE be employed in clinical practice for 3DMRCP acquisition due to its fast acquisition speed.Acknowledgements
No acknowledgement found.References
1. Geethanath S, Reddy R, Konar AS, Imam S, Sundaresan R, DR RB, et al. Compressed sensing MRI: a review. Critical Reviews™ in Biomedical Engineering. 2013;41(3):183-204.
2. Lustig M, Donoho DL, Santos JM, Pauly JM. Compressed sensing MRI. IEEE signal processing magazine. 2008;25(2):72-82.
3. Feng L, Benkert T, Block KT, Sodickson DK, Otazo R, Chandarana H. Compressed sensing for body MRI. Journal of Magnetic Resonance Imaging. 2017;45(4):966-87.
4. Lustig M, Donoho D, Pauly JM. Sparse MRI: The application of compressed sensing for rapid MR imaging. Magnetic Resonance in Medicine: An Official Journal of the International Society for Magnetic Resonance in Medicine. 2007;58(6):1182-95.
5. Yoon JH, Lee SM, Kang H-J, Weiland E, Raithel E, Son Y, et al. Clinical feasibility of 3-dimensional magnetic resonance cholangiopancreatography using compressed sensing: comparison of image quality and diagnostic performance. Investigative radiology. 2017;52(10):612-9.
6. Kwon H, Reid S, Kim D, Lee S, Cho J, Oh J. Diagnosing common bile duct obstruction: comparison of image quality and diagnostic performance of three-dimensional magnetic resonance cholangiopancreatography with and without compressed sensing. Abdominal Radiology. 2018;43:2255-61
Figures
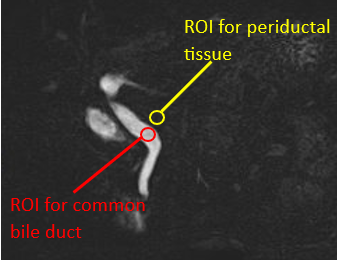
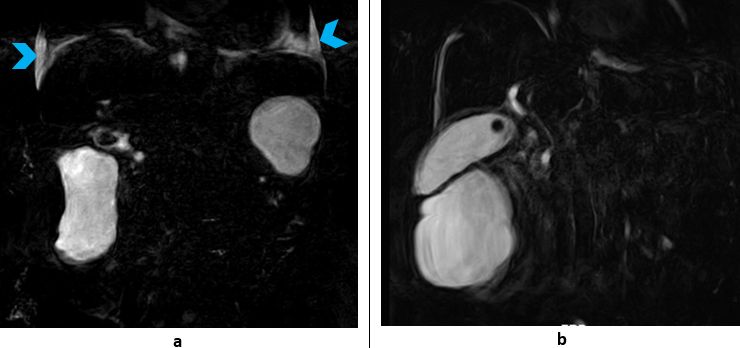
Figure 2. A patient (86 years old, female) with her 3DMRCP done with compressed sensing (a) in 2023 and with SENSE (b) in 2017. It was apparent that the patient had breathing complications during the imaging of cs3DMRCP based on the presence of bilateral pleural effusions (blue arrowhead) and the scan was completed in one minute. Compared to the scan duration of two minutes with SENSE, the degradation of image quality due to motion artefact in both sequences was comparable despite different patient conditions. Image could be further degraded when the scan time is longer.