SHA LIU1, NAN SUN1, ZHEN GUAN1, XIAO TING LI1, YU XIN YANG2, and KE XUE2
1Peking University Cancer Hospital & Institute, BEI JING, China, 2MR Collaboration, United Imaging Research Institute of Intelligent Imaging, BEI JING, China
Synopsis
Keywords:
Motivation: Torso enhanced CT is the standard method for colon cancer staging. MRI is a complimentary method. Our purpose is to develop a MR Colon cancer scanning method with simple process and short scan time.
Goal(s): develop a new T2WI breath-hold scanning technique that eliminates the need for bowel preparation and reduces scan time
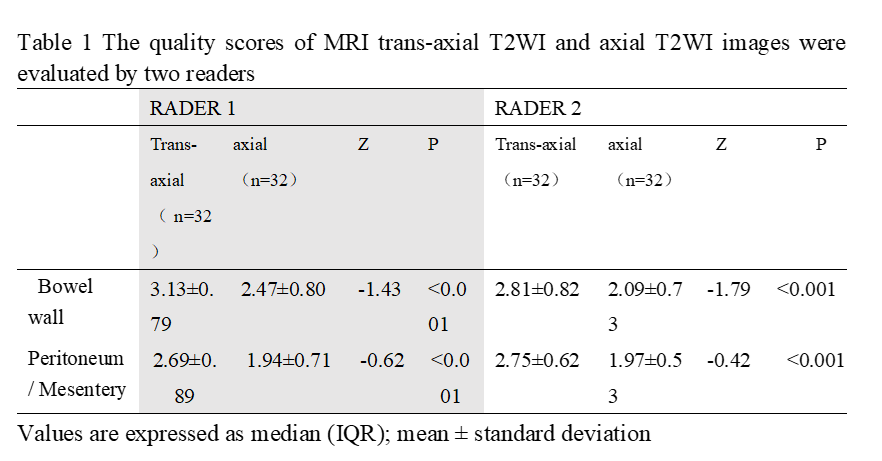
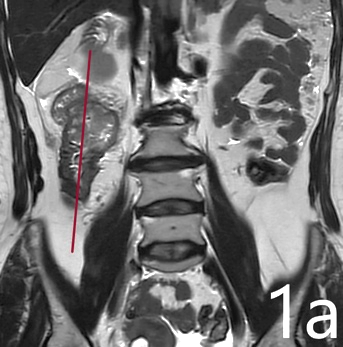
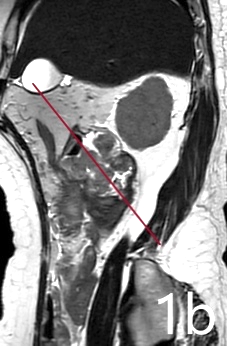
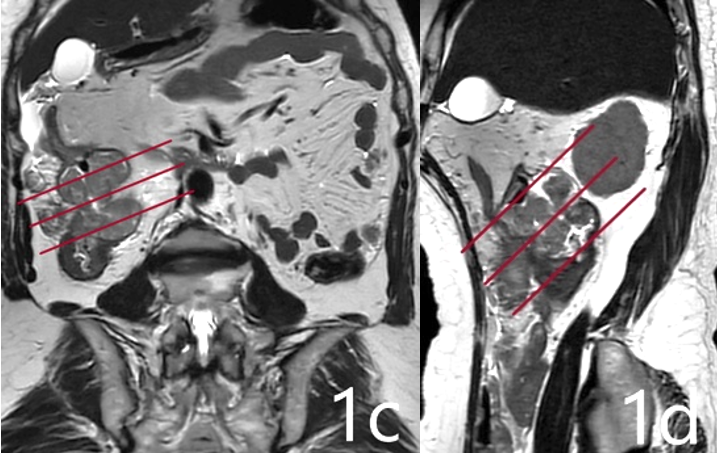
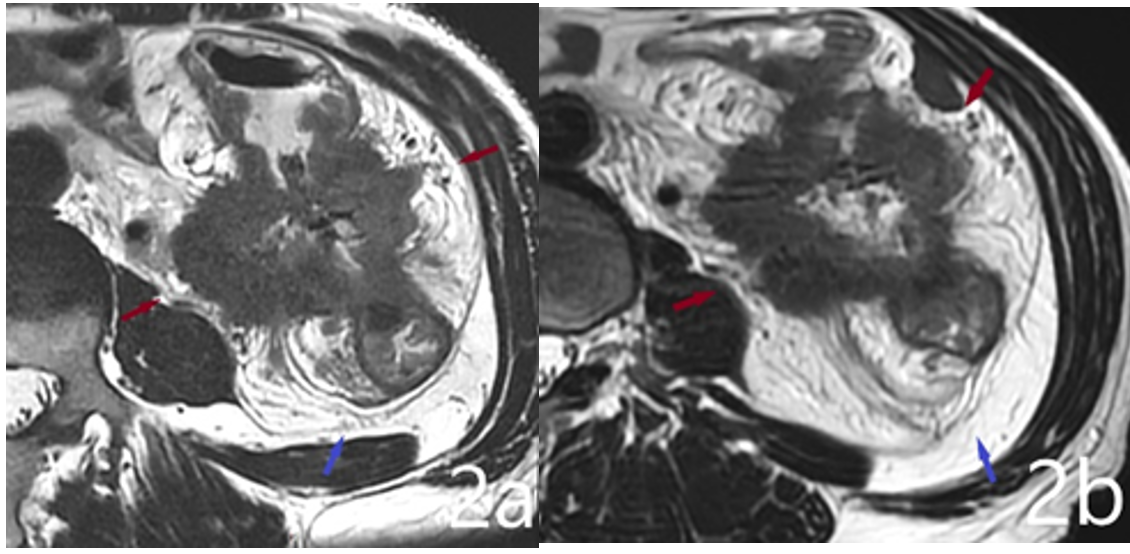
Approach: compared the image quality between trans-axial T2WI and axial T2WI in visualization of anatomical structure
Results: Patient examination time for our colon MRI is less than 10min, compared with conventional MRI, our approach offered a simplified and expedited means of visualizing lesion details with superior clarity.
Impact: Our
research focused on MRI scan optimization. Without bowel preparation, using
breath-hold, our creative trans-axial imaging plan becomes highly manageable
and enables efficient repetition of the entire process.
Acknowledgements
No acknowledgement found.References
[1]Soo Yeun Park,Seung
Hyun Cho,Min A.Lee Ghilsuk YoonY, et al. Diagnostic performance
of MRI- versus MDCT-categorized T3cd/T4 for identifying high-risk stage II or
stage III colon cancers: a pilot study. Abdominal Radiology(2019) 44:1675-1685doi:
https://doi.org/10.1007/s00261-018-1822-7.
[2]Seren R Rafaelsen ,
Claus Dam , Chris Vagn-Hansen, et al. CT and 3 Tesla MRI in
the TN Staging of Colon Cancer: A Prospective, Blind Study. European Journal of
Radiology 121 (2019) 108741:2022, 29(2), 1069-1079;doi:
https://doi.org/10.3390/curroncol29020091.