5139
Evaluation of wave-CAIPI for accelerating MP2RAGE and FLAWS in deep-brain nucleus localization1Department of Radiology, Second Affiliated Hospital of Zhejiang University School of Medicine, Hangzhou, China, 2MR Research Collaboration Team, Siemens Healthineers Ltd., Shanghai, China, 3Siemens Medical Solutions, Boston, MA, USA, Boston, MA, United States, 4Siemens Healthcare, Erlangen, Germany
Synopsis
Keywords:
Motivation: We tested the acceleration method in a clinical setting demanding high-resolution and high-quality structural images.
Goal(s): Deep -brain stimulation requires high-resolution 3D MRI sequences. The Wave CAIPIRINHA (Wave-CAIPI) may be expected to significantly reduce acquisition time while changing tissue contrast.
Approach: We collected scanning data from 5 healthy volunteers, including conventional MP2RAGE and Wave CAIPI research applications (with acceleration factors of 2x2, 2x3, and 3x3, respectively).
Results: Compared with MP2RAGE, the Wave-CAIPI (2Xx2) and Wave-CAIPI (2xX3) sequences provide good tissue contrast while shortening acquisition time.
Impact: This new sequence is helpful to the localization of brain structures for pre-surgical planning.
Introduction
High-resolution 3D MRI sequences play a critical role in the localization of brain structures for pre-surgical planning, especially for deep-brain nuclei such as the internal globus pallidus, substantia nigra, and subthalamic nucleus, crucial for deepMPRAGE and MP2RAGE sequences are commonly used in pre-surgical planning due to their excellent gray matter (GM) and white matter (WM) contrast 4. Additionally, the FLuid And White matter Suppression (FLAWS) imaging technique enhances the visualization of deep brain GM structures 5. Notably, MP2RAGE can be tailored to provide both FLAWS contrast and standard T1 contrast by selecting specific inversion times, offering versatile images for various needs 6. Nevertheless, lengthy scan durations can be intolerable for some patients due to their medical conditions.
The Wave CAIPIRINHA (Wave-CAIPI) method introduces significant acceleration in 3D image acquisition by using a "corkscrew" trajectory instead of a Cartesian read-out and employing under-sampling in two directions 7,8 This study aims to determine whether Wave-CAIPI can significantly reduce the scan duration of MP2RAGE-FLAWS while preserving intricate details of deep brain GM structures crucial for surgical planning.
Methods
MRI experiments were conducted at 3T (MAGNETOM Vida, Siemens Healthcare, Erlangen, Germany) using a 64-receiver channel head/neck matrix coil. Five healthy volunteers participated, and data were collected for each subject, including conventional MP2RAGE and Wave-CAIPI research application (with acceleration factors of 2x2, 2x3, and 3x3). Sequence parameters are summarized in Table 1. Image quality was evaluated subjectively (overall clarity of brain tissue) and objectively (signal contrast of small structures). Six regions of interest (ROIs) in the left and right hemispheres, covering the internal globus pallidus, substantia nigra, and subthalamic nucleus, were assessed for signal contrast on the FLAWS1 image. The signal contrast of each ROI for the five subjects was averaged.Results
Figure 1 displays sagittal brain MR images of healthy volunteers acquired using the MP2RAGE sequence and three Wave-CAIPI sequences with different acceleration factors. These results suggest that obtaining two sets of 3D images, one without gray/white matter signal and the other without cerebrospinal fluid signal, is feasible with a single acquisition.Figure 2 illustrates the visualization of ROIs using these four sequences. Wave-CAIPI (2x2) and wave-CAIPI (2x3) sequences provide good tissue contrast while shortening acquisition time compared to MP2RAGE. Signal contrast measurements indicate that the accelerated Wave-CAIPI sequences maintain acceptable tissue contrast for small structures (Table 2). Notably, the Wave-CAIPI sequence with a 2x2 acceleration factor improves tissue visualization of the right hemisphere's internal globus pallidus compared to MP2RAGE. Additionally, the wave-CAIPI sequence with a 2x3 acceleration factor provides better tissue contrasts (1.703, 1.445, 1.395) for the left hemisphere's substantia nigra and subthalamic nucleus compared to the 2x2 acceleration factor (1.603, 1.380, 1.366). The tissue contrast for the left hemisphere's substantia nigra is similar to that of MP2RAGE (1.807).
Discussion
This study explored the impact of Wave-CAIPI on visualizing deep brain GM structures. Compared to routine MP2RAGE with a 3-fold acceleration, an acceleration rate of 4 (2x2) was achievable while maintaining sufficient tissue contrast. In some cases, an acceleration factor of 6 (2x3) also produced satisfactory images.MRI acquisition acceleration is a recent research focus. While high acceleration is attainable theoretically, real clinical imaging scenarios require validation to assess the applicability of different methods. Wave-CAIPI is an acceleration method based on novel k-space acquisition schemes and parallel imaging 9.
In this study, we tested the acceleration method in a clinical setting demanding high-resolution and high-quality structural images. A reduction of 50~75% in acquisition time was achieved without significant compromise in deep GM structural details. Variations among subjects may be due to head size and tissue contrast differences related to aging and other factors. Limitations include a relatively small sample size and the absence of patient data. However, most PD patients do not exhibit significant pathological changes in these deep brain GM structures, so we do not anticipate major changes in image quality for patients.
Conclusion
The Wave-CAIPI technique shows promise for accelerating high-resolution MP2RAGE imaging, aiding in the visualization of deep brain structures. Even with an acceleration factor of 4, structural details are well preserved. In situations requiring even shorter acquisition times, an acceleration factor of 6 may be considered a viable option. Nevertheless, exceeding this acceleration factor may result in images not meeting the required quality standards.Acknowledgements
No acknowledgement found.References
References
1 Pinsker MO, Volkmann J, Falk D, et al. Deep brain stimulation of the internal globus pallidus in dystonia: target localisation under general anaesthesia. Acta Neurochir (Wien) 2009;151:751–758.
2 Wider C, Pollo C, Bloch J, Burkhard PR, Vingerhoets FJ. Longterm outcome of 50 consecutive Parkinson’s disease patients treated with subthalamic deep brain stimulation. Parkinsonism Relat Disord 2008;14:114–119.
3 Vasques X, Cif L, Hess O, Gavarini S, Mennessier G, Coubes P.Stereotactic model of the electrical distribution within the internal globus pallidus during deep brain stimulation. J Comput Neurosci 2009;26:109–118.
4. Jack CR Jr, Bernstein MA, Fox NC, et al. The Alzheimer’s Disease Neuroimaging Initiative (ADNI): MRI methods. J Magn Reson Imaging. JMRI 2008;27:685–691.
5. Redpath TW, Smith FW. Technical note: use of a double inversion recovery pulse sequence to image selectively grey or white brain matter. Br J Radiol 1994;67:1258–1263.
6. Marques JP, Kober T, Krueger G, van der Zwaag W, Van de Moortele PF, Gruetter R. MP2RAGE, a self bias-field corrected sequence for improved segmentation and T1-mapping at high field. NeuroImage 2010;49:1271–1281.
7. Bilgic B, Gagoski BA, Cauley SF, Fan AP, Polimeni JR, Grant PE, Wald LL, Setsompop K. Wave-CAIPI for highly accelerated 3D imaging. Magn Reson Med 2015;73:2152-2162.
8. Polak D, Setsompop K, Cauley SF, Gagoski BA, Maier F, Backert P, Wald LL, Bilgic B. Wave-CAIPI for Highly Accelerated MP-RAGE Imaging. Magn Reson Med, 2017; DOI: 10.1002/mrm.26649.
9. Cauley SF, Setsompop K, Bilgic B, Bhat H, Gagoski B, Wald LL. Autocalibrated wave-CAIPI reconstruction; Joint optimization of k-space trajectory and parallel imaging reconstruction. Magn Reson Med 2016; DOI:10.1002/mrm.26499
Figures
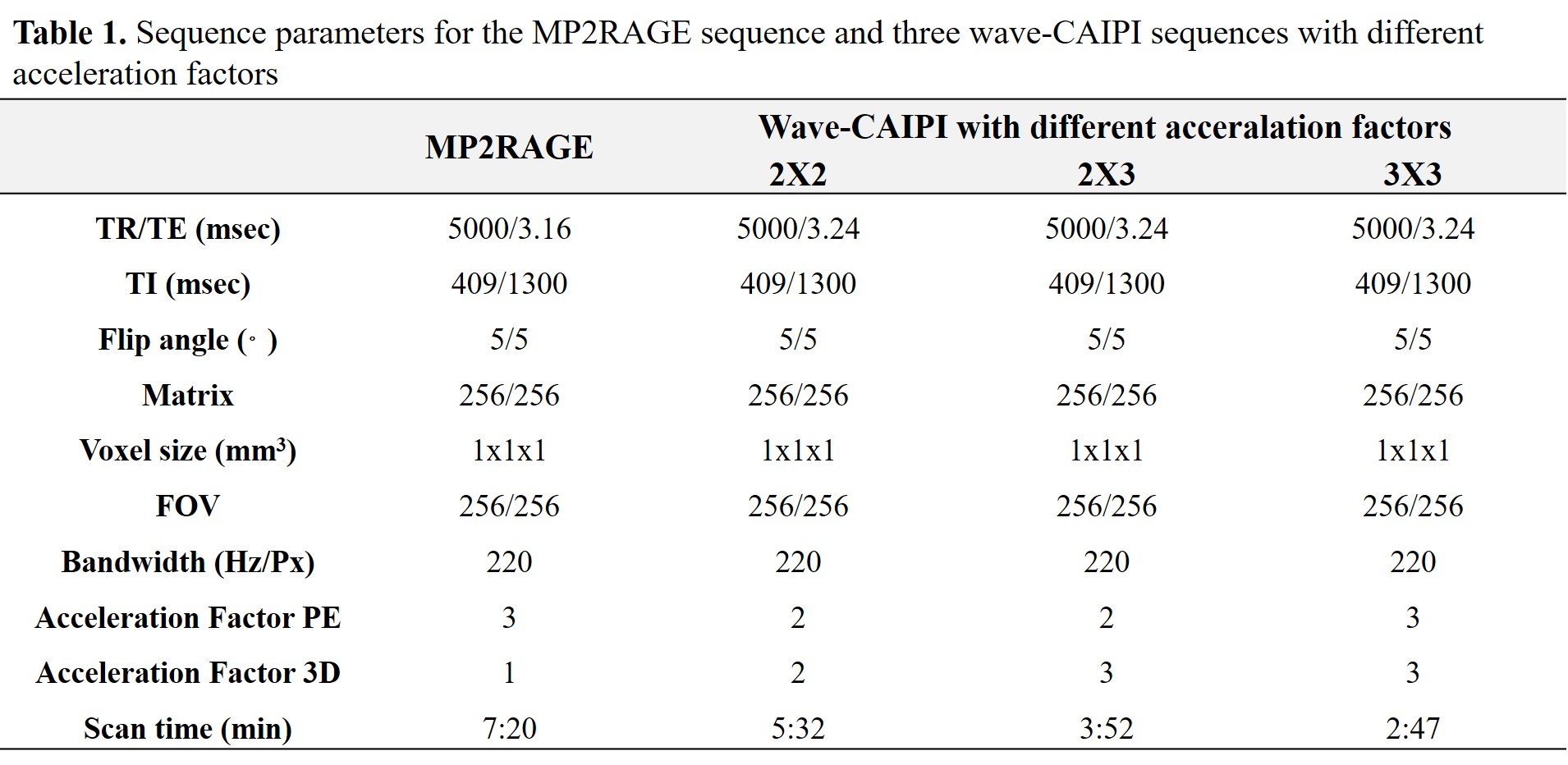
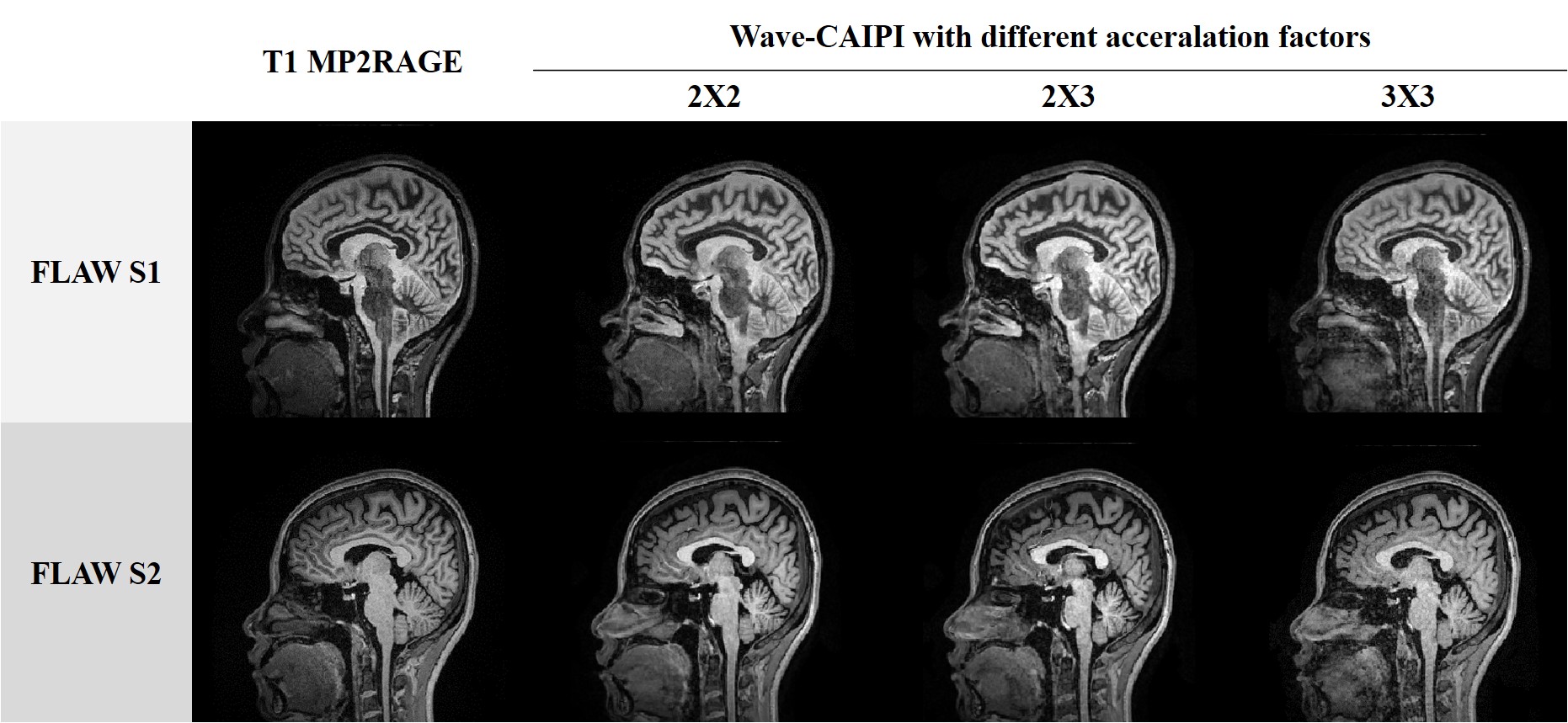
Figure 1. Overview of sagittal brain MR images of a healthy volunteer acquired with the MP2RAGE sequence and three wave-CAIPI sequences with different acceleration factors.
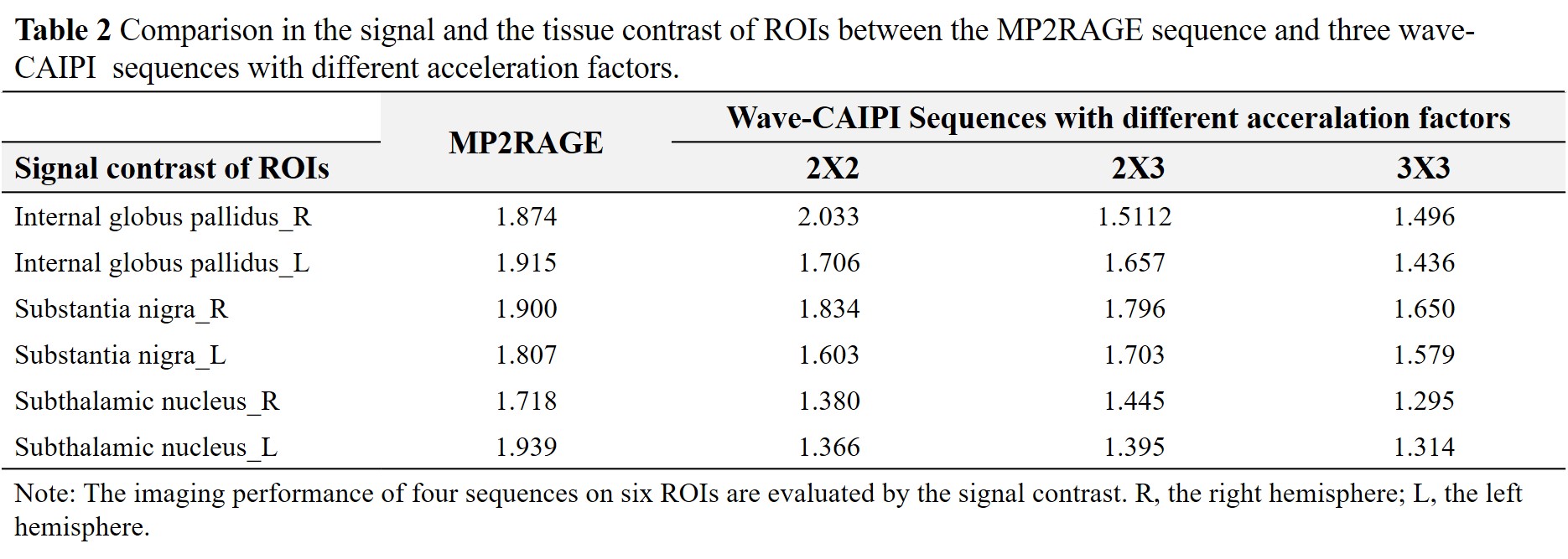
Table 2. Comparison in the signal and the tissue contrast of ROIs between the MP2RAGE sequence and three wave-CAIPI sequences with different acceleration factors.
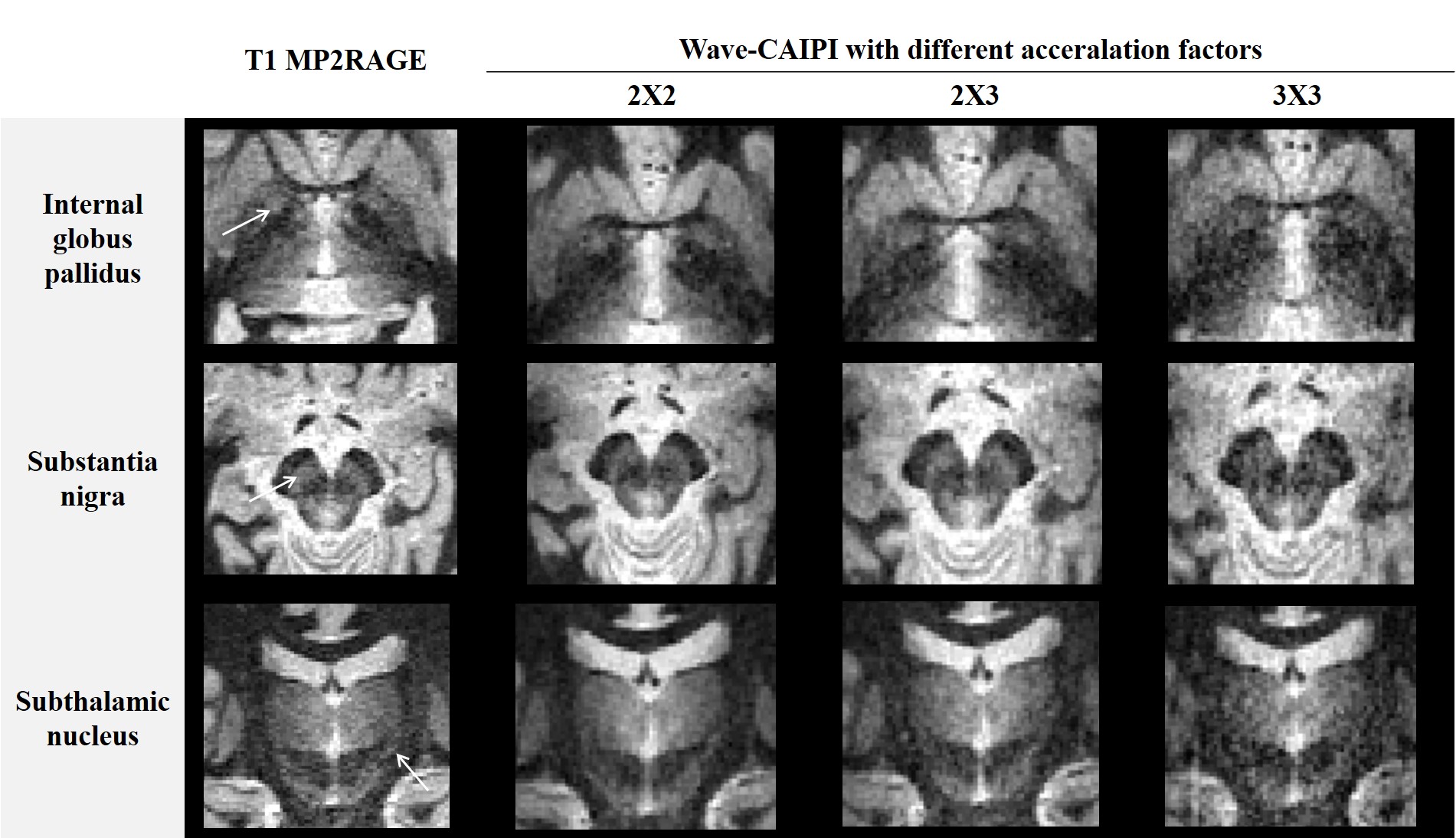
Figure 2. The visualization of ROIs using the MP2RAGE sequence and three wave-MP2RAGE sequences with different acceleration factors.