5120
Automated MR Spectroscopy single-voxel placement in suspected diffuse glioma based on tumor biology1Department of Radiology and Biomedical Imaging, Yale School of Medicine, New Haven, CT, United States, 2Department of Therapeutic Radiology, Yale School of Medicine, New Haven, CT, United States, 3Center for Outcomes Research and Evaluation (CORE), Yale School of Medicine, New Haven, CT, United States, 4Center for Image Sciences, University Medical Center Utrecht, Utrecht, Netherlands, 5University of Ulm, Ulm, Germany, 6Visage Imaging GmbH, Berlin, Germany
Synopsis
Keywords: Tumors (Pre-Treatment), Software Tools, AI/ML Software; Brain; Machine Learning/Artificial Intelligence;Neuro; Spectroscopy; Tumors
Motivation: Acquiring single-voxel Magnetic Resonance Spectroscopy (MRS) data in clinic currently involves manual voxel placement by technicians without the time capacity to review tumor biology in detail, leading to poor-quality spectra.
Goal(s): To achieve consistent and accurate single-voxel placement to minimize variability in metabolite quantification.
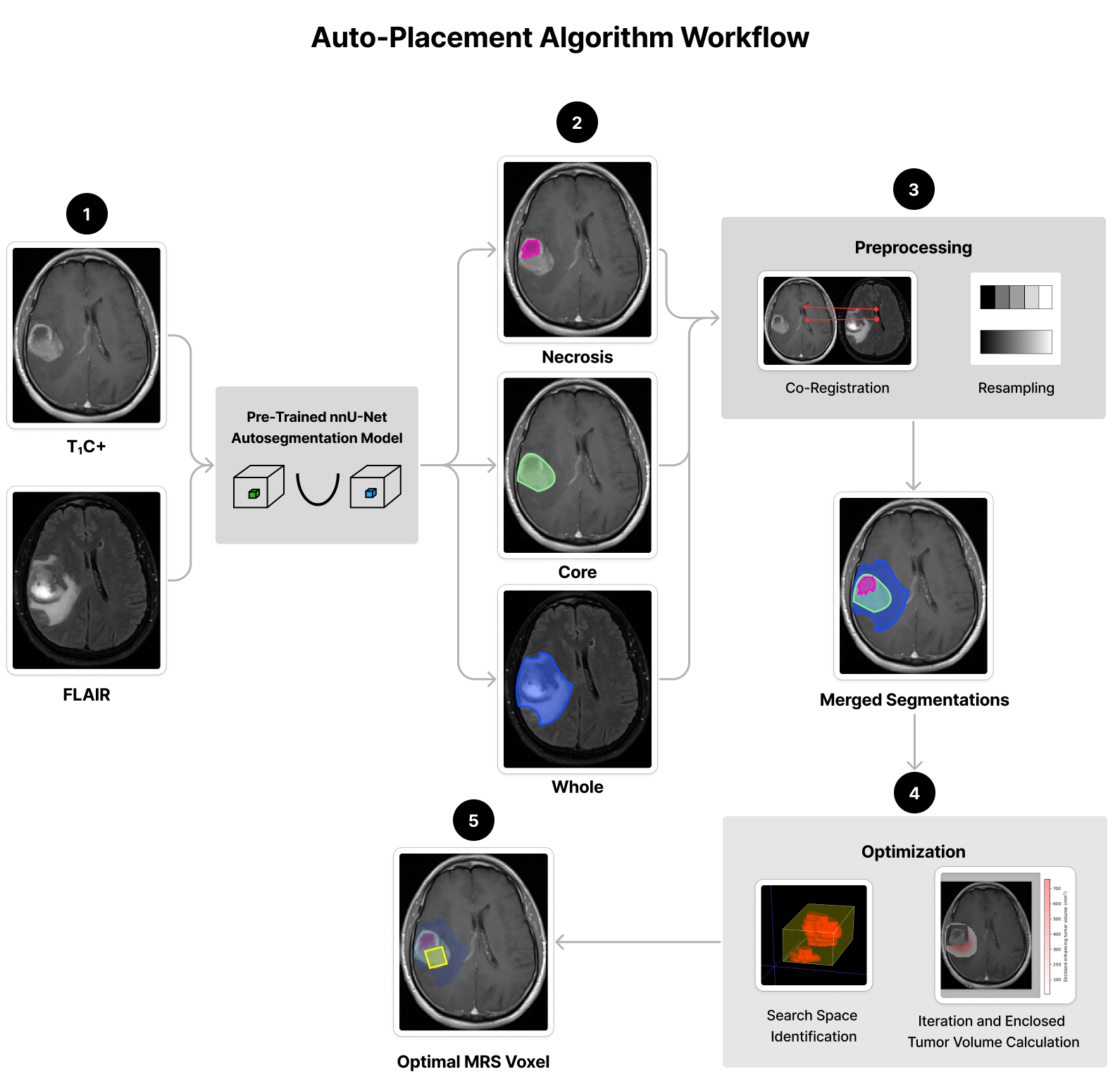
Approach: We developed an auto-placement algorithm that identifies an optimized MRS single-voxel position and rotation based on tumor biology (tumor core, necrosis, and edema) and outputs this voxel as a mask on MR Imaging.
Results: Performance of the automated MRS single-voxel placement rivals clinical placement and integrates with an existing clinically implemented automated brain tumor segmentation workflow.
Impact: Our new algorithm will assist radiology technicians in reliably placing MR Spectroscopy single-voxels with accuracy that rivals clinical placement. This is a primary need for non-invasive diagnosis and management of diffuse gliomas.
Introduction
Diffuse gliomas are characterized by specific dysregulated metabolic pathways, e.g., the production of 2-hydroxyglutarate due to isocitrate dehydrogenase mutations.1,2 Magnetic Resonance Spectroscopy (MRS) can visualize these metabolic pathways for glioma subtype diagnosis and management.3 Acquiring single-voxel MRS data currently involves manual voxel placement, requiring understanding of tumor biology (i.e., tumor core, necrosis, and edema). Inconsistent voxel placement leads to variability in metabolite quantification resulting from partial volume effects. Moreover, in clinic voxel placement is usually carried out by technicians without the time capacity to review tumor biology in detail, leading to poor-quality spectra (Figure 1). Thus, there is a need for consistent and accurate MRS voxel placement.Existing algorithms are for non-tumor4-6 or only low-grade7 diffuse gliomas with whole tumor segmentation on fluid attenuated inversion recovery (FLAIR). We developed an auto-placement algorithm for both suspected low-grade and high-grade diffuse gliomas that identifies an optimized MRS single-voxel position and rotation bases on tumor core, necrosis, and edema, which integrates with an existing clinically implemented automated brain tumor segmentation workflow8.
Methods
nnU-Net Auto-segmentation ModelPatients at the study institution who underwent treatment for histopathologically confirmed diffuse glioma between January 1999 and March 2022 with a pre-treatment T1-weighted contrast-enhanced (T1C+) and/or FLAIR MR study were included. Studies containing motion artifacts were excluded. Tumor core (enhancement) and necrosis on T1C+ as well as whole tumor hyperintensity (including edema) on FLAIR were segmented using a pre-trained UNet-based algorithm.9 Three medical student research fellows corrected the segmentations, which were validated by a board-certified neuroradiologist (M.S.A). These ground-truth segmentations were used to train an nnU-Net auto-segmentation model10.
Input and Pre-Processing
T1C+ and FLAIR images are used as input for the auto-placement algorithm. nnU-Net segmentations are then predicted for tumor core (enhancement), necrosis and/or whole (tumor hyperintensity). When present, the FLAIR image and whole segmentation are co-registered to the T1C+ image. All images are resampled to 1mm isotropic voxel size. (Figure 2)
Optimization
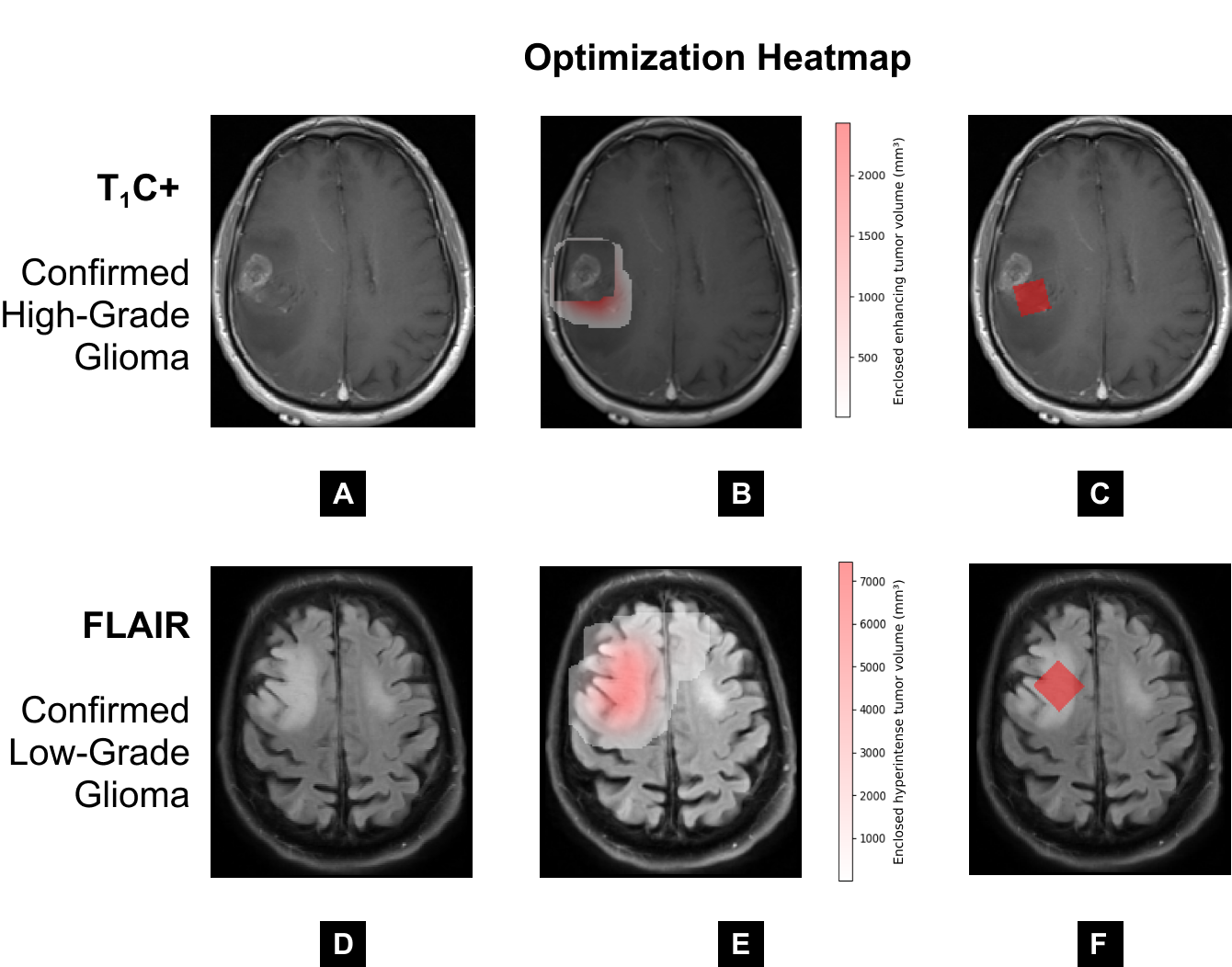
A bounding box around the tumor core, padded by 2√3cm, represents the search space for the center of the optimal MRS voxel. During optimization, a 2x2x2cm isotropic (as used in clinic) MRS voxel mask is iteratively positioned at 1mm intervals within the search space and rotated from 0-90 degrees along the x, y, and z axes. For each orientation tested, the mask is intersected with the core, necrosis, and whole segmentations to calculate the different enclosed volumes (Figure 2). Enclosed core volume is maximized without enclosing any necrosis, as shown in the heatmap in Figure 3B. If multiple voxel orientations enclose equivalent core volume, whole is maximized. Figure 3C shows an example of an MRS voxel identified to be the optimal solution. In suspected low-grade gliomas without enhancement, only the FLAIR image and whole segmentation are used. For these cases, the algorithm maximizes enclosed hyperintensity (Figure 3E).
The pipeline was written in Python (version 3.10). Image pre-processing was done using SimpleITK11 (version 2.2.1) and TorchIO (version 0.19.1)12. Optimization used TorchIO 12, SciPy (version 1.11.2)13, and NumPy (version 1.25.2)14.
Quality Assessment
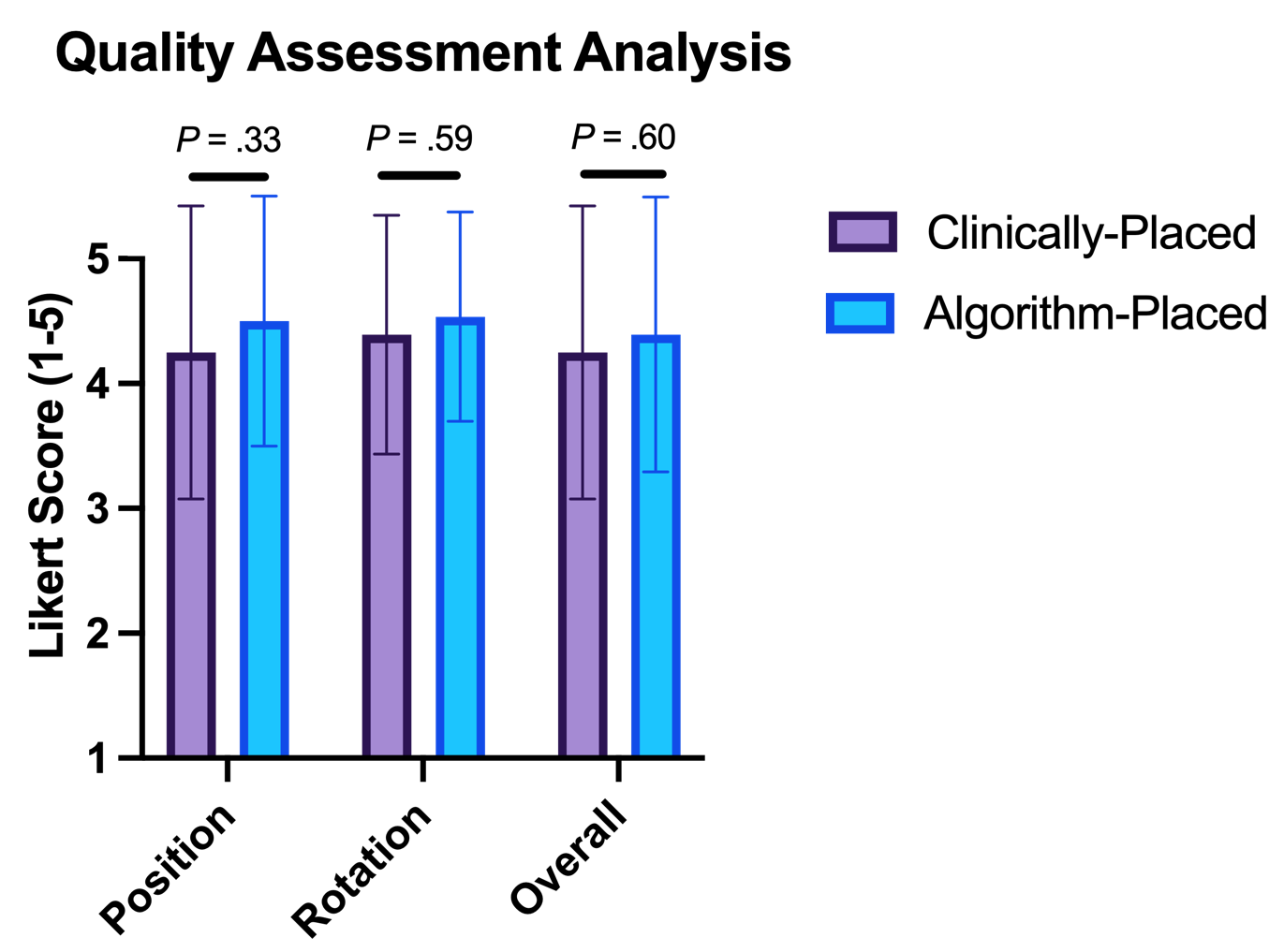
Patients at the study institution who underwent single-voxel MRS between 1998 and 2023 with suspected diffuse glioma and historical images of clinically-placed voxels were included. Two board-certified neuroradiologists (M.S.A.; F.M.) evaluated the quality of clinically-placed (overall, position, and rotation) versus algorithm-placed voxels on a 5-point Likert scale (1 = poor quality; 5 = strong quality). A paired t-test was used to compare mean Likert scores between the two groups. P < .05 was considered statistically significant.
Results
OutputOf 1033 segmented diffuse glioma cases, 699 were used for the nnU-Net. Dice scores for nnU-Net predictions were 80% for core segmentation, 81% for whole, and 71% for necrosis.
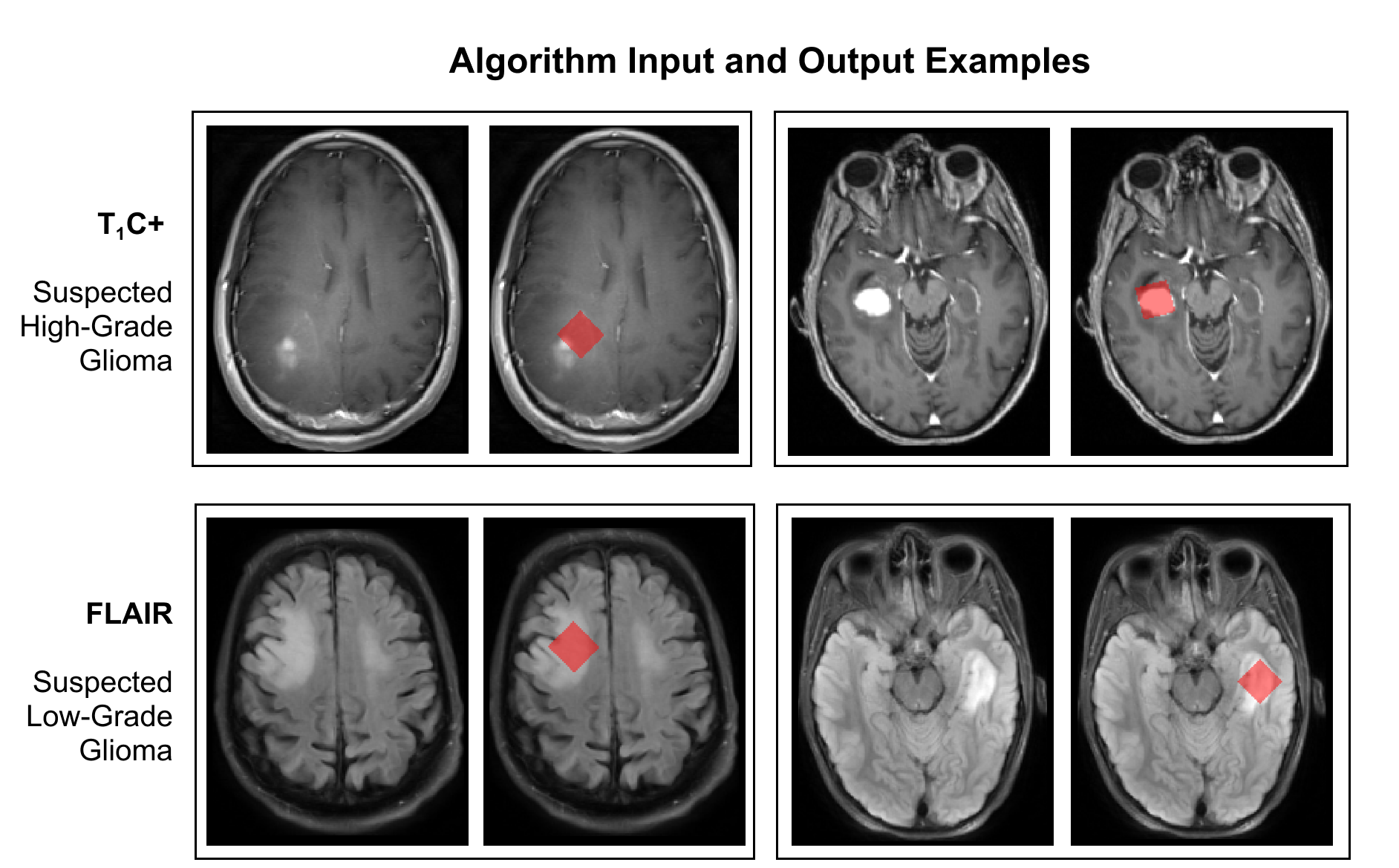
14 cases were selected for quality assessment, of which 8 demonstrated FLAIR hyperintensity without enhancement. Figure 4 shows example inputs and outputs.
Quality Assessment
An expert assessment revealed that algorithmic voxel placement was comparable to superior compared to clinical, with no statistically significant differences between the two groups (Figure 5).
Discussion
Our tumor biology-driven algorithm for automated MRS single-voxel placement in suspected diffuse glioma rivals clinical placement. In this work, for instant clinical application and validation, we chose to keep the same voxel size as used in clinic. As only axial slices were evaluated for now, the next step would be to evaluate in all three image directions. We would also like to further optimize the algorithm with different voxel sizes and setting limits for distance to skull and ventricles to limit artifacts. Nonetheless, expert evaluation demonstrated strong performance of our algorithm and its promising applications in computer-aided MRS single-voxel placement.Acknowledgements
No acknowledgement found.References
- Louis DN, Perry A, Reifenberger G, von Deimling A, Figarella-Branger D, Cavenee WK, et al. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: a summary. Acta Neuropathol (Berl). 2016 Jun;131(6):803–20.
- Louis DN, Perry A, Wesseling P, Brat DJ, Cree IA, Figarella-Branger D, et al. The 2021 WHO Classification of Tumors of the Central Nervous System: a summary. Neuro-Oncol. 2021 Aug 2;23(8):1231–51.
- Padelli F, Mazzi F, Erbetta A, et al. In vivo brain MR spectroscopy in gliomas: clinical and pre-clinical chances. Clin Transl Imaging. 2022;10(5):495-515. doi:10.1007/s40336-022-00502-y
- Park YW, Deelchand DK, Joers JM, Hanna B, Berrington A, Gillen JS, et al. AutoVOI: real-time automatic prescription of volume-of-interest for single voxel spectroscopy. Magn Reson Med. 2018 Nov;80(5):1787–98.
- Bishop JH, Geoly A, Khan N, Tischler C, Krueger R, Keshava P, et al. Real-Time Semi-Automated and Automated Voxel Placement using fMRI Targets for Repeated Acquisition Magnetic Resonance Spectroscopy. J Neurosci Methods. 2023 May 15;392:109853.
- Dou W, Speck O, Benner T, Kaufmann J, Li M, Zhong K, et al. Automatic voxel positioning for MRS at 7 T. Magma N Y N. 2015 Jun;28(3):259–70.
- Bolan PJ, Branzoli F, Di Stefano AL, Nichelli L, Valabregue R, Saunders SL, et al. Automated Acquisition Planning for Magnetic Resonance Spectroscopy in Brain Cancer. Med Image Comput Comput-Assist Interv MICCAI Int Conf Med Image Comput Comput-Assist Interv. 2020 Oct;12267:730–9.
- Aboian M, Bousabarah K, Kazarian E, Zeevi T, Holler W, Merkaj S, et al. Clinical implementation of artificial intelligence in neuroradiology with development of a novel workflow-efficient picture archiving and communication system-based automated brain tumor segmentation and radiomic feature extraction. Front Neurosci. 2022;16:860208.
- Aboian M, Bousabarah K, Kazarian E, Zeevi T, Holler W, Merkaj S, et al. Development of a workflow efficient PACS based automated brain tumor segmentation and radiomic feature extraction for clinical implementation (N2.003). Neurology [Internet]. 2022 May 3 [cited 2023 Nov 5];98(18 Supplement). Available from: https://n.neurology.org/content/98/18_Supplement/3146
- Isensee F, Jaeger PF, Kohl SAA, Petersen J, Maier-Hein KH. nnU-Net: a self-configuring method for deep learning-based biomedical image segmentation. Nat Methods. 2021 Feb;18(2):203–11.
- Beare R, Lowekamp B, Yaniv Z. Image Segmentation, Registration and Characterization in R with SimpleITK. J Stat Softw. 2018 Sep 4;86:1–35.
- Pérez-García F, Sparks R, Ourselin S. TorchIO: A Python library for efficient loading, preprocessing, augmentation and patch-based sampling of medical images in deep learning. Comput Methods Programs Biomed. 2021 Sep;208:106236.
- Virtanen P, Gommers R, Oliphant TE, Haberland M, Reddy T, Cournapeau D, et al. SciPy 1.0: fundamental algorithms for scientific computing in Python. Nat Methods. 2020 Mar;17(3):261–72.
- Harris CR, Millman KJ, van der Walt SJ, Gommers R, Virtanen P, Cournapeau D, et al. Array programming with NumPy. Nature. 2020 Sep;585(7825):357–62.
Figures
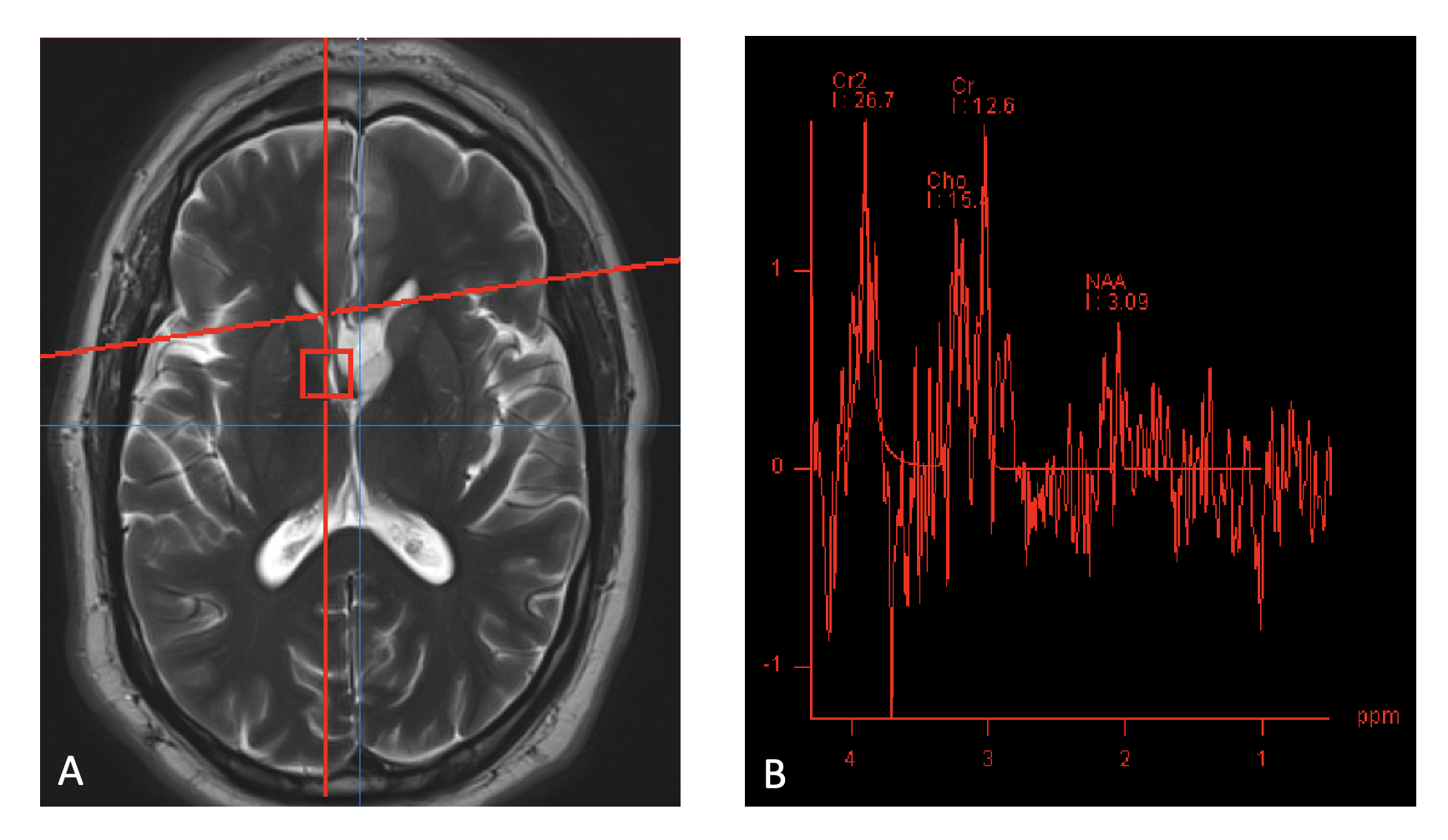
(A) Example of an incorrectly placed voxel (red box) partially in the ventricles with no enclosed hyperintensity on fluid attenuated inversion recovery (FLAIR) and (B) subsequent very noisy spectrum acquired on a 3T Siemens MRI scanner, model Verio, with a spin echo single voxel sequence with a TE of 135 ms.