5119
Different Tracer Kinetic Models in predicting key molecular marker in adult diffuse Gliomas1Department of Radiology, The Affiliated Drum Tower Hospital of Nanjing University Medical School, Nanjing, China, 2Jiangsu Key Laboratory of Medical Optics, Suzhou Institute of Biomedical Engineering and Technology, Chinese Academy of Sciences, Suzhou, China
Synopsis
Keywords: Tumors (Pre-Treatment), Tumor, DCE-MRI, IDH, Glioma, P53, CDKN2A/B
Motivation: IDH, P53 and CDKN2A/2B are key molecular markers for adult diffuse gliomas.
Goal(s): This study aimed to compare values of conventional and advanced tracer kinetic models based on dynamic contrast enhanced (DCE)-MRI in predicting IDH, P53 and CDKN2A/B status in glioma patinets.
Approach: Patients diagnosed as adult diffuse gliomas were examined using dynamic contrast-enhanced MRI. Imaging data were analyzed using tracer kinetic models.
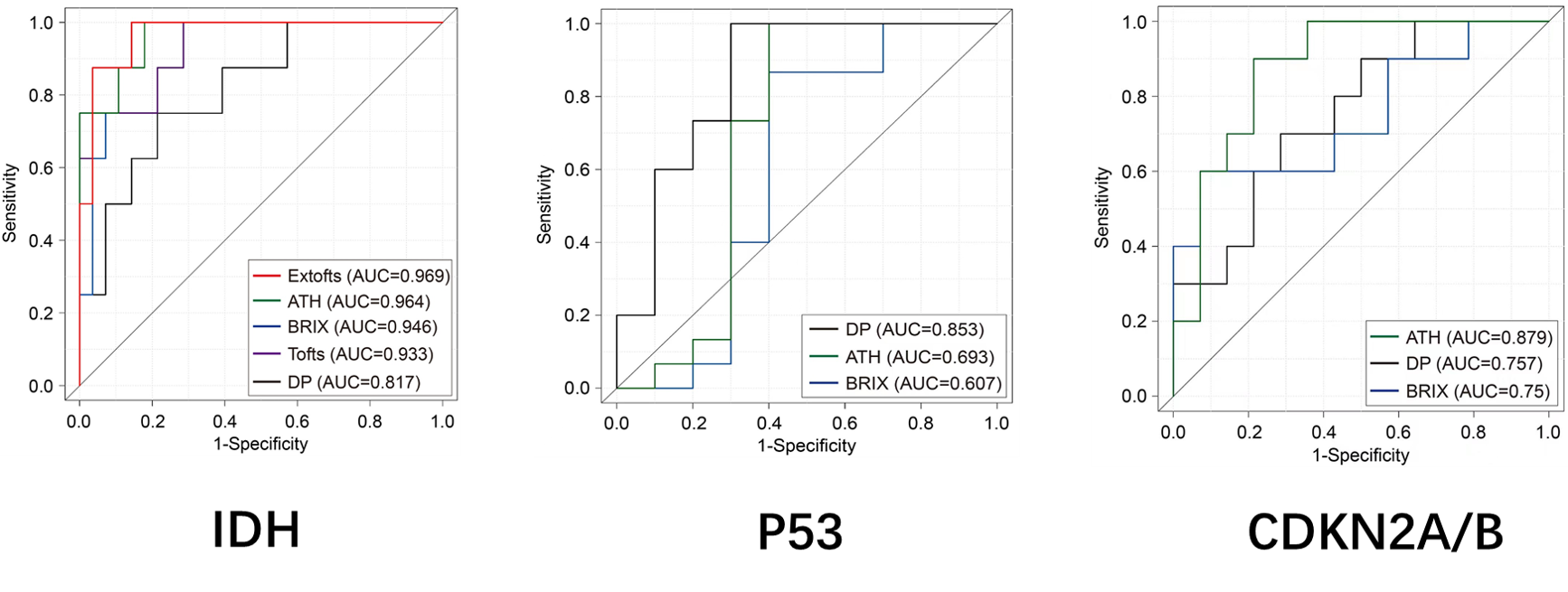
Results: Extofts model attained best performance in predicting IDH mutation.ATH model attained best performance in predicting P53 mutation. DP model attained best performance in predicting CDKN2A/B homozygous deletion.
Impact: Different Tracer Kinetic Models have illustrated excellent performance in predicting different molecular markers in glioma patients.
Background and Purpose
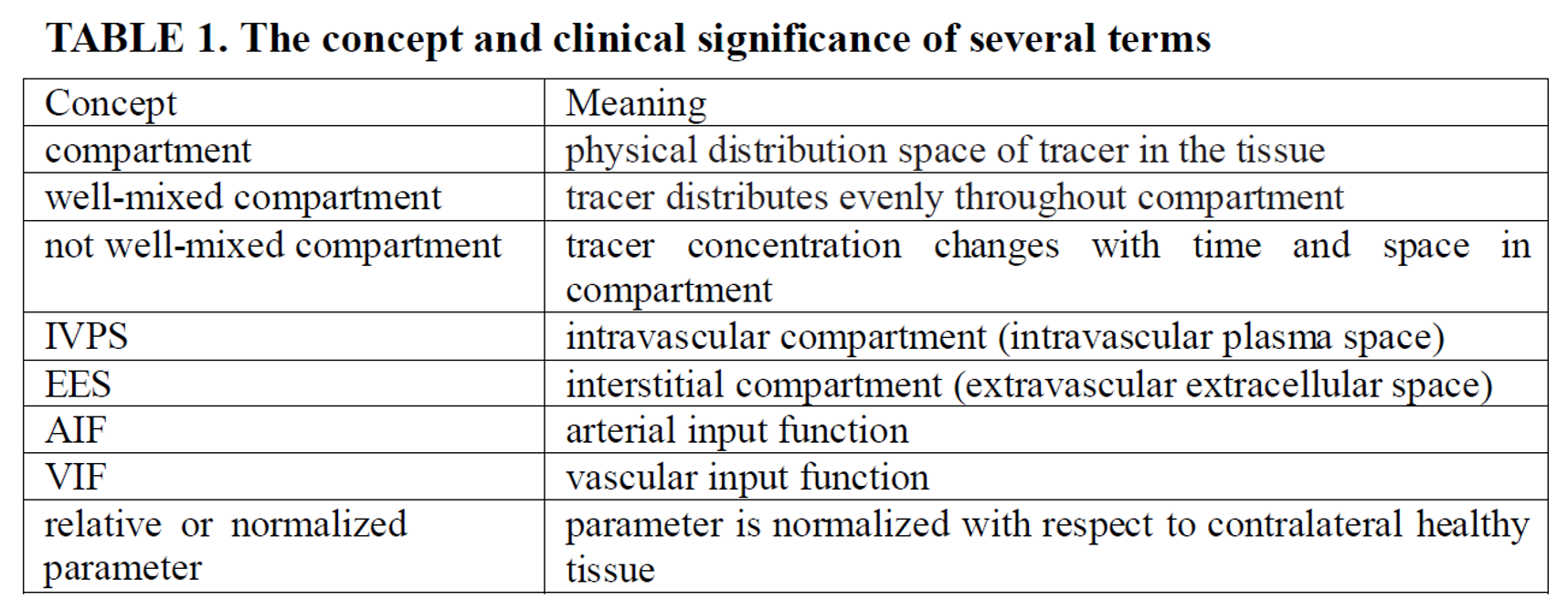
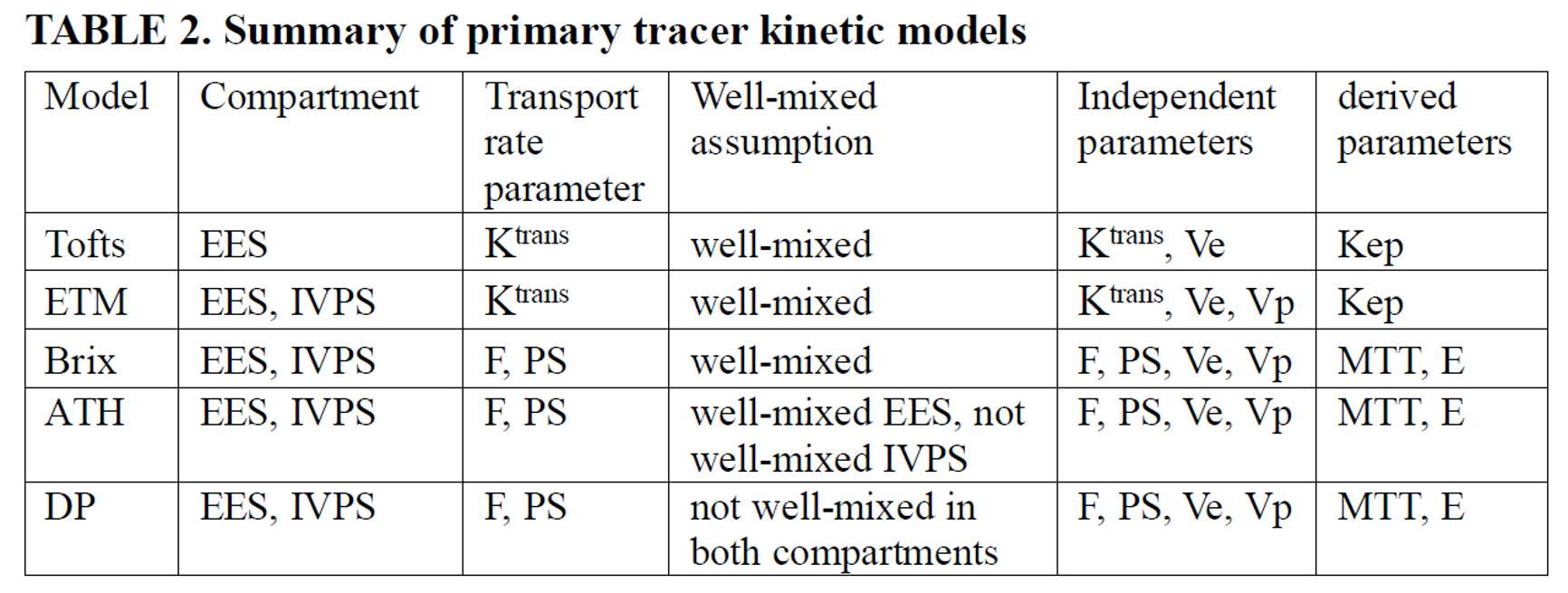
Gliomas are the most common type of primary central nervous system malignancy1. Isocitrate dehydronanse(IDH), P53 and cyclin-dependent kinase inhibitor 2A/B (CDKN2A/B) are key molecular markers in adult diffuse gliomas patients2-3. Given the choice of surgical protocol and the assessment of prognosis, it is important to accurately predict key molecular markers before surgery.Compared with conventional imaging techniques, DCE perfusion has the advantages of higher spatial resolution, better quantification of microvascular leakiness and perfusion, and increased resistance to susceptibility artifacts4-5. DCE imaging data can be quantitatively analyzed using a tracer kinetic model, a mathematical description of tracer molecular transport within the tissue microenvironment that derives quantitative values of various model parameters pertaining to the tissue status. However, the results of conventional tracer kinetic models such as Tofts or Extended-Tofts model have been ambiguous6. The meaning of several terms has been summarized in Table 1. Primary tracer kinetic models have been listed in Table 2.
This study was aimed to explore different dynamic contrast-enhanced (DCE) MRI tracer kinetic models in predicting IDH, P53 and CDKN2A/B in adult diffuse Glioma patients.
Materials and Methods
Patients diagnosed as adult diffuse gliomas between 2022 and 2023 were included. All patients underwent examination before surgery in a 3.0T MR scanner (uMR770, United Imaging Healthcare). DCE-MRI was performed after Gadodiamide injection (0.2mL/kg, 3.5mL/s). DCE images were analyzed using MItalytics software (FISCA Healthcare, Singapore). Tofts, Extended-Tofts, approximated tissue homogeneity (ATH), Brix, and distributed parameter (DP) models were employed for quantitative analysis of DCE data, leading to the following parameters: Ktrans (Tofts, ExTofts), Ve (all), CBV (all), Kep (=Ktrans/Ve; Tofts, ExTofts); CBF, MTT, PS and E for ATH, Brix and DP.Region-of-interests of tumor, edema and normal white matter (nWM) were delineated manually. IDH and P53 mutation status was determined by next generation sequencing. CDKN2A/B homozygous deletion status was determined by Fluorescence in situ hybridization. Parameter values were normalized by nWM. Mann-Whitney U test was utilized to compare the difference between groups. Performance of differential diagnosis was quantified using area under ROC curve (AUC). Parameters with P<0.05 were selected and fused using Logistic regression method.
Results
Thirty-six patients were included, with twenty-eight IDH-wildtype and eight IDH-mutant, ten P53-wildtype and fifteen P53-mutant, fourteen CDKN2A/B-intact and ten CDKN2A/B-homozygous deleted.As illustrated in figure1, model-wise AUCs for IDH mutation were 0.969 (ExTofts), 0.964 (ATH), 0.946 (Brix), 0.933(Tofts) and 0.817 (DP) respectively. Model-wise AUCs for P53 mutation were 0.853 (DP), 0.693(ATH) and 0.607 (Brix) respectively. Tofts and Extofts model showed no efficacy in predicting P53 mutation. Model-wise AUCs for CDKN2A/B homozygous deletion were 0.879 (ATH), 0.757(DP) and 0.750 (Brix) respectively. Tofts and Extofts model showed no efficacy in predicting CDKN2A/B homozygous deletion status.
Conclusion
Extofts moddel achiedve best performance in predicting IDH mutation.DP model achiedve best performance in predicting P53 mutation. ATH model achiedve best performance in predicting CDKN2A/B homozygous deletion. Different Tracer Kinetic Models have shown great potential in predicting key molecular markers in adult diffuse glioma.Acknowledgements
No acknowledgement found.References
1. SHOBEIRI P, SEYEDMIRZAEI H, KALANTARI A, et al. The Epidemiology of Brain and Spinal Cord Tumors [J]. Adv Exp Med Biol, 2023, 1394: 19-39.
2. Huang LE. Impact of CDKN2A/B Homozygous Deletion on the Prognosis and Biology of IDH-Mutant Glioma. Biomedicines. 2022 Jan 24;10(2):246.
3. Ludwig K, Kornblum HI. Molecular markers in glioma. J Neurooncol. 2017 Sep;134(3):505-512.
4. Cha S. Update on brain tumor imaging: from anatomy to physiology. AJNR Am J Neuroradiol. 2006 Mar;27(3):475-487.
5. Essig M, Shiroishi MS, Nguyen TB, et al. Perfusion MRI: the five most frequently asked technical questions. AJR Am J Roentgenol. 2013 Jan;200(1):24-34.
6. Kickingereder P, Wiestler B, Sahm F, et al. Primary central nervous system lymphoma and atypical glioblastoma: multiparametric differentiation by using diffusion-, perfusion-, and susceptibility-weighted MR imaging. Radiology. 2014 Sep;272(3):843-850.
Figures