5109
Feasibility and utility of multishell diffusion weighted imaging acquisition is comparable to standard DTI sequences used in clinical settings.1School of Biological and Health Systems Engineering, Arizona State University, Tempe, AZ, United States, 2Vanderbilt University, Nashville, TN, United States, 3Mayo Clinic, Phoenix, AZ, United States
Synopsis
Keywords: Diffusion Acquisition, Diffusion/other diffusion imaging techniques
Motivation: Multi-shell diffusion sequences can support data models that help provide greater specificity to tissue microstructure when standard-of-care clinical diffusion acquisition schemes (using b=0, 1000) fail.
Goal(s): To show that multi-shell acquisitions can produce results comparable to those of standard-of-care clinical acquisitions in addition to supporting the implementation of higher order diffusion models.
Approach: Standard DTI metrics like FA and MD were compared in specific regions of interest in participant data collected using both a, (1) standard diffusion acquisition and (2) multishell diffusion sequence. NODDI metrics were also calculated for our multishell data.
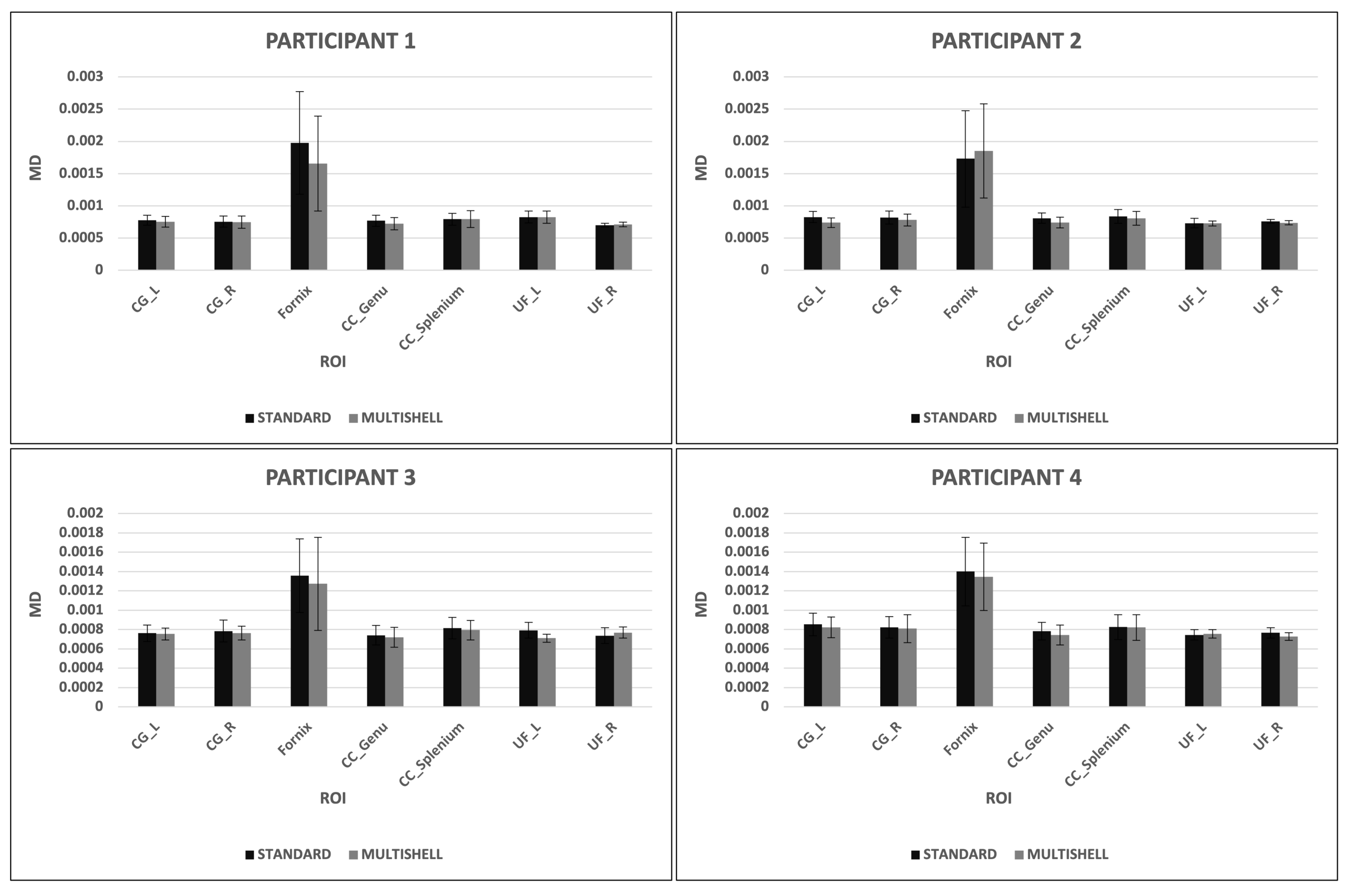
Results: FA and MD metrics obtained from both acquisitions were comparable.
Impact: Our study shows that a multishell diffusion sequence is suitable to meet standard clinical outcomes but is also capable of greater data acquisition (within regular scan time) which enables complex diffusion model implementations and hence, quantify tissue microstructure more precisely.
Introduction
Multi-shell diffusion acquisition schemes and advanced biophysical models of diffusion in tissue are tools of growing importance to the non-invasive quantification of physiologic structure and function. Despite this, such acquisitions are not widely used in clinical settings, in part because: (i) they have typically required longer than acceptable scan times and (ii) single-shell-based diffusion tensor imaging (DTI) metrics like fractional anisotropy (FA) and mean diffusivity (MD) have become established as standard-of-care in the clinic. Advances in parallel and sparse acquisition methods have greatly reduced scan times and brought these methods within an acceptable scan time (<15 minutes), however, transition from standard-of-care DTI-based metrics to more advanced model-based biophysical metrics will require significant investigation and validation; as such, we have developed a multi-shell sequence to support both standard DTI and multiple investigational biophysical models of diffusion. Such a sequence will allow concurrent clinical and investigative work and eliminate the need for a sperate standard-of-care DTI sequence. Here, we show that comparable DTI-based metrics can be calculated from our multi-shell diffusion dataset as compared to a standard-of-care single-shell DTI sequence, suggesting that this sequence can reliably replace the DTI acquisition in the standard clinical workflow.Methods
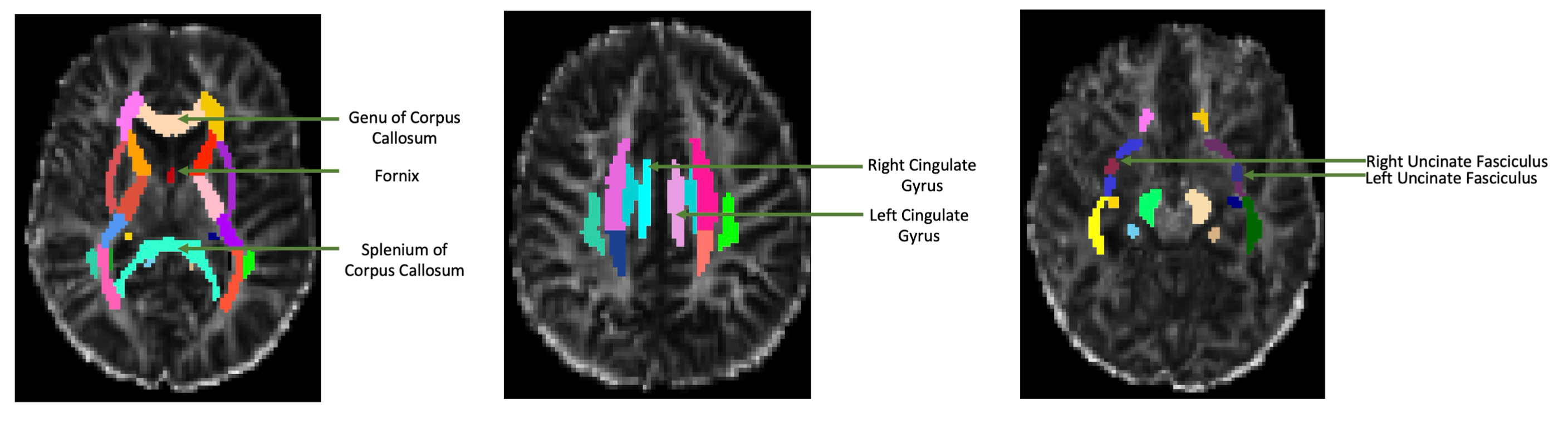
Four participants were analyzed for this study. Data acquisition: Imaging data were acquired on a 3T Siemens scanner using a 20-channel coil. The following neuroimaging scans were collected for clinical assessment: (i) MPRAGE T1-w image (TR/TE 1900/2.02 ms, 208 slices), (ii) standard-of-care diffusion-weighted acquisitions with b-value= 1000 s/mm2 with 30 directions (TR/TE 10000/71 ms, 31 slices) and a b= 0 s/mm2 image at the beginning of the acquisition; flip-angle = 90°; acquisition time ~7 mins and, (iii) multi-shell diffusion-weighted acquisitions with the following parameters: b-values= 100, 200, 300, 500, 750, 1000, 1500, 2000 & 2500 s/mm2; 6 directions at b=100-500, 12 directions at b=700, 18 directions at b=1000, 24 directions at b=1500, 30 directions at b=2000 and 36 directions at b=2500 (TR/TE 3664/95.6 ms, 185 slices) and a b= 0 s/mm2 image at the beginning of the acquisition; flip-angle = 90°; acquisition time ~14 mins; an acceleration factor of 2 each, using SMS[1] and iPAT[2] technologies was applied. Data processing: b=0, 1000 volumes were extracted from multi-shell diffusion data to ensure that the data from both acquisitions (standard and multi-shell) fit the DTI calculation. The ICBM DTI-81 atlas[3][4] was used for region of interest (ROI) estimation and masking. White matter ROIs used were: the white matter of the left and right cingulate gyrus, corpus callosum genu and splenium, left and right uncinate fasciculus and, the fornix [see Fig. 1]. Diffusion images underwent brain extraction (to estimate regions only containing brain tissue and excluding the outer skull surface) and a brain mask was obtained. The DTI calculation was performed on each acquisition to obtain FA and MD maps (using FSL[5]) and neurite orientation dispersion and density imaging (NODDI)[6] parameters, including neurite density index (NDI) and orientation distribution index (ODI) were calculated (using Matlab[7]). Resultant FA, MD, NDI, and ODI maps were then both linearly (to obtain the affine transformation matrix) and non-linearly co-registered to the ICBM FA template space because it is critical that images being analyzed are in the same coordinate space. Since ROIs are in template space, data needed to be warped and transformed from native space to template space. Voxel-wise FA, MD, NDI and ODI values in the selected ROIs were extracted for standard and multi-shell acquisitions and compared.Results
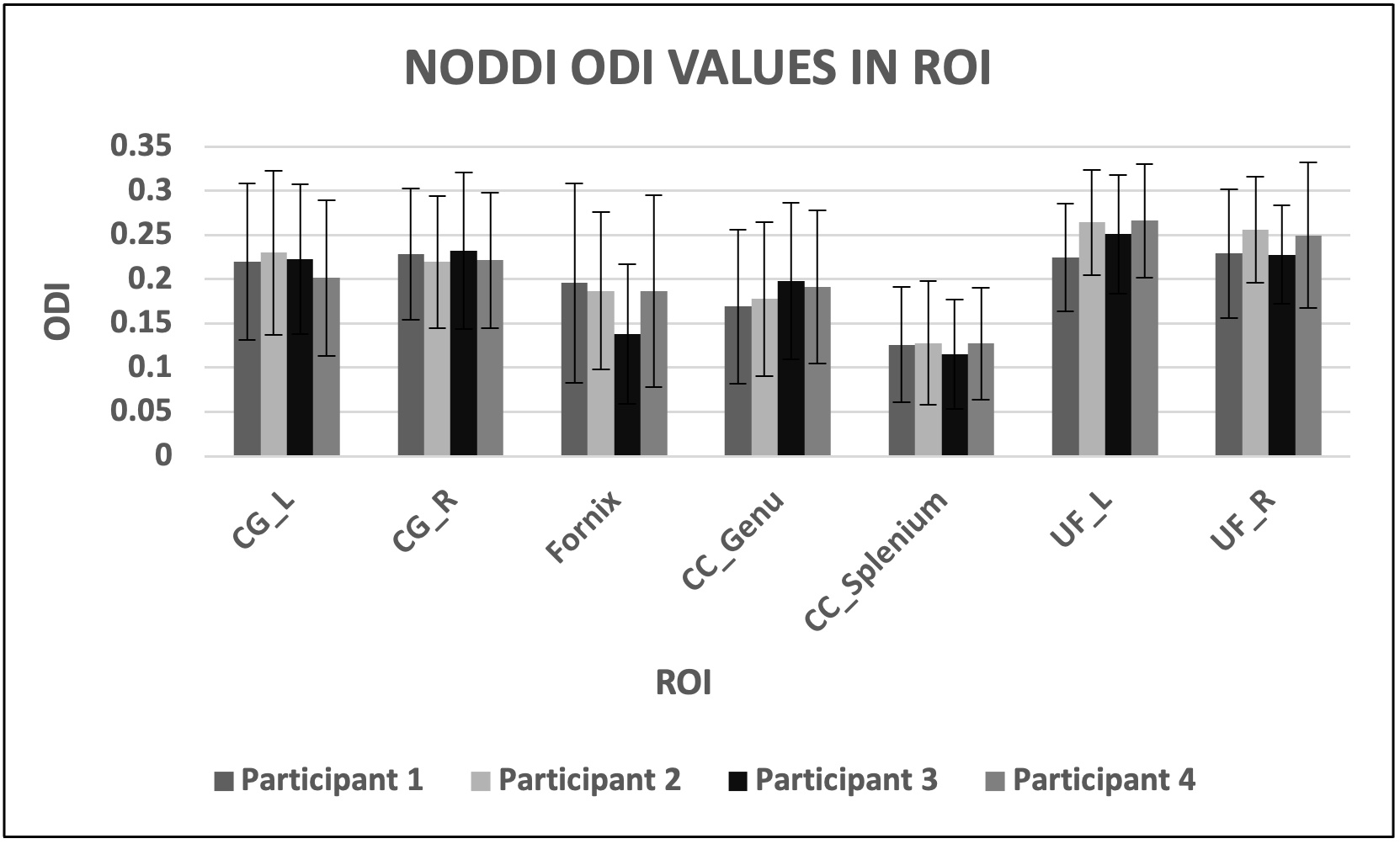
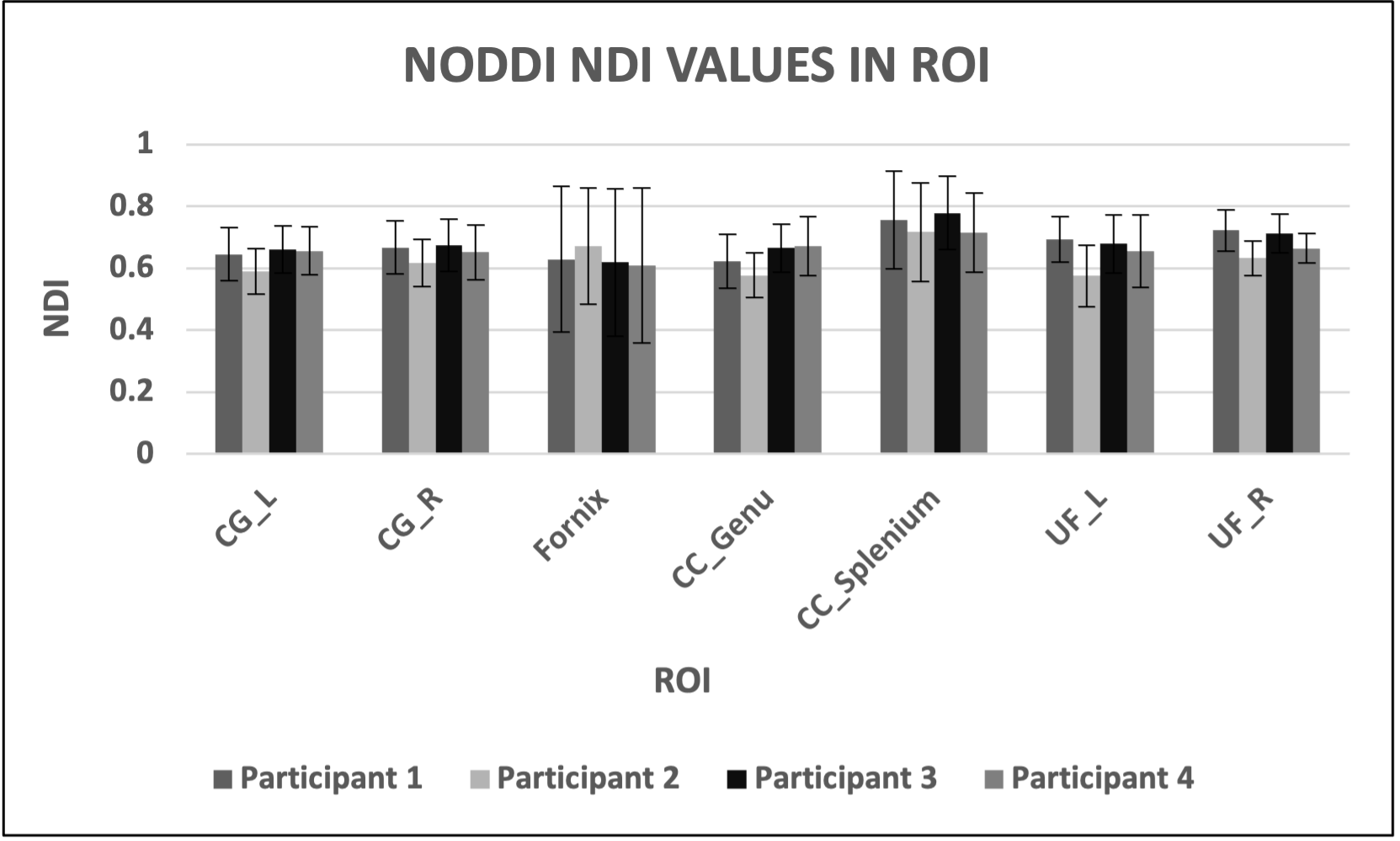
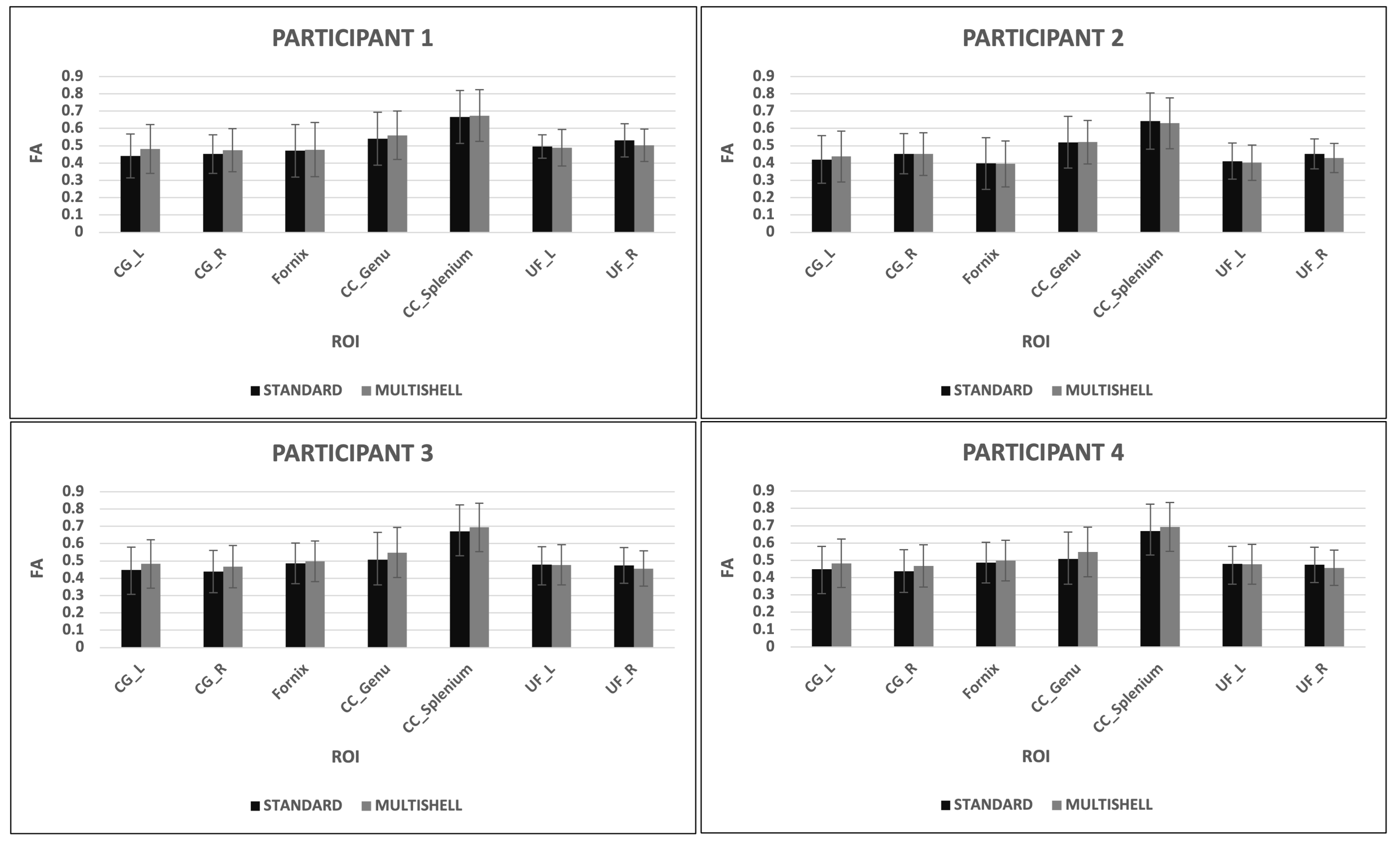
Our sequence is also able to support application of the NODDI model as seen in Figs. 2 and 3. Reported values were comparable to those cited in literature[8][9]. No significant differences were found between DTI metrics obtained from standard and multi-shell sequences [see Figs. 4 and 5], suggesting that our multi-shell diffusion sequence can support standard clinical implementations of DTI, such as neurosurgical planning or fiber tract generation.Discussion and Conclusions
Multi-shell diffusion and biophysical model-based quantification of tissue microstructure hold significant promise for improved diagnosis and monitoring of disease, particularly those of the brain. However, DTI is the current standard-of-care and transition to biophysical model-based metrics will require substantial validation. Here, we show that our multi-shell acquisition scheme can be used for standard-of-care DTI mapping of FA and MD while also supporting modern biophysical models, represented here by NODDI. Future work will focus on establishing normative biophysical model parameter values in the clinical setting and comparing them against concurrent DTI values. This will be the first step towards transition from DTI to biophysical models in our clinical setting.Acknowledgements
No acknowledgement found.References
iPAT Extensions. (n.d.). Siemens Healthineers. Retrieved November 8, 2023, from https://www.siemens-healthineers.com/en-us/magnetic-resonance-imaging/options-and-upgrades/clinical-applications/ipat-extensions
Simultaneous Multi-Slice. (n.d.). Siemens Healthineers. Retrieved November 8, 2023, from https://www.siemens-healthineers.com/en-us/magnetic-resonance-imaging/options-and-upgrades/clinical-applications/simultaneous-multi-slice
Mori et al., MRI Atlas of Human White Matter. Elsevier, Amsterdam, The Netherlands (2005)
Atlases - FslWiki. (2023, August 22). FSL - FslWiki. Retrieved November 7, 2023, from https://fsl.fmrib.ox.ac.uk/fsl/fslwiki/Atlases.
FMRIB, Oxford, UK [Behrens 2003a] T.E.J. Behrens, M.W. Woolrich, M. Jenkinson, H. Johansen-Berg, R.G. Nunes, S. Clare, P.M. Matthews, J.M. Brady, and S.M. Smith. Characterization and propagation of uncertainty in diffusion-weighted MR imaging. Magn Reson Med, 50(5):1077-1088, 2003. https://fsl.fmrib.ox.ac.uk/dti
Zhang, H., Schneider, T., Wheeler-Kingshott, C. A., & Alexander, D. C. (2012). NODDI: practical in vivo neurite orientation dispersion and density imaging of the human brain. Neuroimage, 61(4), 1000-1016.
Microstructure Imaging Group | NODDI Matlab toolbox. (2021, November 29). UCL Microstructure Imaging Group. Retrieved November 7, 2023, from http://mig.cs.ucl.ac.uk/index.php?n=Tutorial.NODDImatlab
Pieri, V., Sanvito, F., Riva, M., Petrini, A., Rancoita, P. M., Cirillo, S., ... & Falini, A. (2021). Along‐tract statistics of neurite orientation dispersion and density imaging diffusion metrics to enhance MR tractography quantitative analysis in healthy controls and in patients with brain tumors. Human Brain Mapping, 42(5), 1268-1286.
Wen, Q., Kelley, D. A., Banerjee, S., Lupo, J. M., Chang, S. M., Xu, D., ... & Nelson, S. J. (2015). Clinically feasible NODDI characterization of glioma using multiband EPI at 7 T. NeuroImage: Clinical, 9, 291-299.
Figures