5108
Accelerating high-resolution microstructure mapping based on multi-shell diffusion MRI for acute ischemic stroke1Academy of Medical Engineering and Translational Medicine, Tianjin University, Tianjin, China, 2Tianjin Key Laboratory of Brain Science and Neuroengineering, Tianjin, China, 3Haihe Laboratory of Brain-Computer Interaction and Human-Machine Intepration, Tianjin, China, 4Department of Medical Imaging, Tianjin Huanhu Hospital, Tianjin University, Tianjin, China, 5Department of Biomedical Engineering, Tsinghua University, Beijing, China
Synopsis
Keywords: Microstructure, Stroke
Motivation: The long scanning time of multi-shell diffusion MRI precludes many promising microstructural models to be applied in acute diseases.
Goal(s): To achieve high-resolution microstructural mapping in acute ischemic stroke.
Approach: We fine-tuned the previously proposed DeepHIBRID method with a multi-shell protocol of 5-minute constraint.
Results: 14 maps from 4 diffusion models were obtained, with whole brain coverage and 1.3mm isotropic voxel size. Preliminary results showed decent contrasts to reveal lesions, and the microstructural information indicated was in agreement with the expected pathologies for both chronic and acute cases.
Impact: High-resolution microstructural mapping based on multi-shell diffusion MRI should be now feasible for acute diseases, which is rarely possible either with compromised spatial resolution or brain coverage.
Introduction
Diffusion MRI enables non-invasive probing of the microstructure of biological tissue and was commonly adopted in clinical examinations. However, the requirements of long acquisition time for many promising microstructural models based on multi-shell diffusion MRI preclude their application in clinical settings, especially for acute diseases. In previous work, we proposed the DeepHIBRID method1, which takes 10 diffusion-weighted images as input that were acquired with a designed sampling pattern in the k-q space to ensure balanced SNR and outputs 14 maps of microstructural metrics from 4 diffusion models2–5, by leveraging the redundancy in both image domain and diffusion metrics domain (Fig. 1). In this study, we aim to examine the feasibility and sensitivity of DeepHIBRID method in reflecting the pathological alterations in the clinical scenarios with tight time constraints, such as acute ischemic stroke.Methods
Participants: Two patients diagnosed with ischemic stroke were enrolled in this study and underwent an MRI examination on a 3T SIEMENS Prisma scanner in Tianjin Huanhu Hospital. With the confirmed diagnosis from the clinical standard examinations (Fig. 2), the DeepHIBRID acquisition protocol described below was administered. Patient one is a 65-year-old male who was in the acute period of the ischemic stroke, while patient two is a 72-year-old male in the chronic period of ischemic stroke.Data Acquisition: Three different b-values with different resolutions for each b-value were comprised in the DeepHIBRID acquisition protocol namely: 1.3mm iso. for b=1000 s/mm2, 1.8mm iso. for b=2000 s/mm2, 2.5mm iso. for b=3000 s/mm2. For each resolution, three b0 images, three diffusion-weighted images with orthogonal diffusion-weighting directions, and one b0 image with reversed phase encoding direction were acquired. The total acquisition time was 4 min and 43 seconds.
Data Preprocessing: All images were corrected for susceptibility distortions6 and linearly registered to the averaged b0 image of 1.3mm resolution7,8 for motion and eddy current correction. The nine normalized diffusion-weighted images and one b0 image were taken as the input of DeepHIBRID network to predict the 14 diffusion metrics maps at the resolution of 1.3mm iso. The DeepHIBRID network was pre-trained using the HCP adult dataset9 and fine-tuned with fully sampled data acquired in 12 healthy participants on the same Prisma scanner in local hospital using an HCP-style protocol.
Results
As shown in Fig. 3, the diffusion metrics in normal-appearing tissue were largely consistent with their expected anatomical characteristics. The acute lesion located in the pons of patient one (Fig. 4) showed decreased extra-cellular diffusivities (extraMD, extraTrans) and volume fractions (fcsf, fh), and increased intra-cellular volume fractions (ficvf, fintra), suggesting cell swelling with a resultant increased tortuosity in the extracellular space, which was consistent with the characteristic of cytotoxic edema typically seen in the acute phase following ischemic stroke10,11. A chronic lesion of a larger size was found in the frontal lobe of patient two, where a decrease in FA, fh and μFA and increases in the rest metrics were observed compared with the normal-appearing counter lateral regions (Fig. 5). These findings were also consistent with the massive neural losses observed on T2-FLAIR (Fig. 2).Discussion and Conclusion
In this work, we demonstrated an accelerated diffusion microstructural imaging approach based on the DeepHIBRID framework and achieved 14 maps from 4 diffusion models with whole brain coverage and 1.3mm isotropic voxel size, which is otherwise very challenging within feasible scanning time for acute diseases. It is worth mentioning that the smaller-sized acute lesion barely showed up on the T1w, T2w, and T2-FLAIR images, but was clearly revealed on the generated diffusion maps, evidencing a superior sensitivity of microstructural imaging compared to the clinical standard. Further, the imaging characteristics differ between chronic and acute lesions, and the microstructural information conveyed by the complimentary 14 diffusion maps altogether was in good agreement with the expected histological pathology12, evidencing a plausible specificity to diseased tissue microstructures. Moreover, a side finding lies in the peri-ventricular hyperintensities shown up on T2w and T2-FLAIR of patient two (Fig. 2), where ficvf was decreased, fh was increased, which was consistent with characteristics of increased interstitial water that are typically seen in the aged brain13,14.This preliminary study is limited in a few aspects. The network is hard to be tuned specifically for acute stroke patients due to the conflicts of ethics in urgent medical care versus the need of a long acquisition time of fully sampled data. Therefore, the potential significance of the approach remains to be further validated in future investigations with more variations of lesion type and larger sample sizes.
Acknowledgements
This work was supported by the National Natural Scientific Foundation of China 82071994References
- Fan Q, Tian Q, Ngamsombat C, Huang S. DeepHIBRID:How to condense the sampling in the k-q joint space for microstructural diffusion metric estimation empowered by deep learning. In: Proceeding of ISMRM Workshop on Data Sampling and Image Reconstruction. Selona,AZ,USA: ISMRM; 2020. 2.
- Pierpaoli C, Jezzard P, Basser PJ, Barnett A, Di Chiro G. Diffusion tensor MR imaging of the human brain. Radiology. 1996;201(3):637-648.
- Zhang H, Schneider T, Wheeler-Kingshott CA, Alexander DC. NODDI: Practical in vivo neurite orientation dispersion and density imaging of the human brain. NeuroImage. 2012;61(4):1000-1016.
- Kaden E, Kelm ND, Carson RP, Does MD, Alexander DC. Multi-compartment microscopic diffusion imaging. NeuroImage. 2016;139:346-359.
- Kaden E, Kruggel F, Alexander DC. Quantitative mapping of the per-axon diffusion coefficients in brain white matter. Magnetic Resonance in Medicine. 2016;75(4):1752-1763.
- Andersson JLR, Skare S, Ashburner J. How to correct susceptibility distortions in spin-echo echo-planar images: application to diffusion tensor imaging. Neuroimage. 2003;20(2):870-888.
- Jenkinson M, Smith S. A global optimisation method for robust affine registration of brain images. Medical Image Analysis. 2001;5(2):143-156.
- Jenkinson M, Bannister P, Brady M, Smith S. Improved Optimization for the Robust and Accurate Linear Registration and Motion Correction of Brain Images. NeuroImage. 2002;17(2):825-841.
- Uğurbil K, Xu J, Auerbach EJ, et al. Pushing spatial and temporal resolution for functional and diffusion MRI in the Human Connectome Project. NeuroImage. 2013;80:80-104.
- Wang Z, Zhang S, Liu C, et al. A study of neurite orientation dispersion and density imaging in ischemic stroke. Magnetic Resonance Imaging. 2019;57:28-33.
- Adluru G, Gur Y, Anderson JS, Richards LG, Adluru N, DiBella EVR. Assessment of white matter microstructure in stroke patients using NODDI. In: 2014 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society. Chicago, IL: IEEE; 2014:742-745.
- Fung SH, Roccatagliata L, Gonzalez RG, Schaefer PW. MR Diffusion Imaging in Ischemic Stroke. Neuroimaging Clinics of North America. 2011;21(2):345-377.
- Haller S, Kövari E, Herrmann FR, et al. Do brain T2/FLAIR white matter hyperintensities correspond to myelin loss in normal aging? A radiologic-neuropathologic correlation study. Acta Neuropathologica Communications. 2013;1(1):14.
- Rau A, Reisert M, Kellner E, Hosp JA, Urbach H, Demerath T. Increased interstitial fluid in periventricular and deep white matter hyperintensities in patients with suspected idiopathic normal pressure hydrocephalus. Sci Rep. 2021;11(1):19552.
Figures
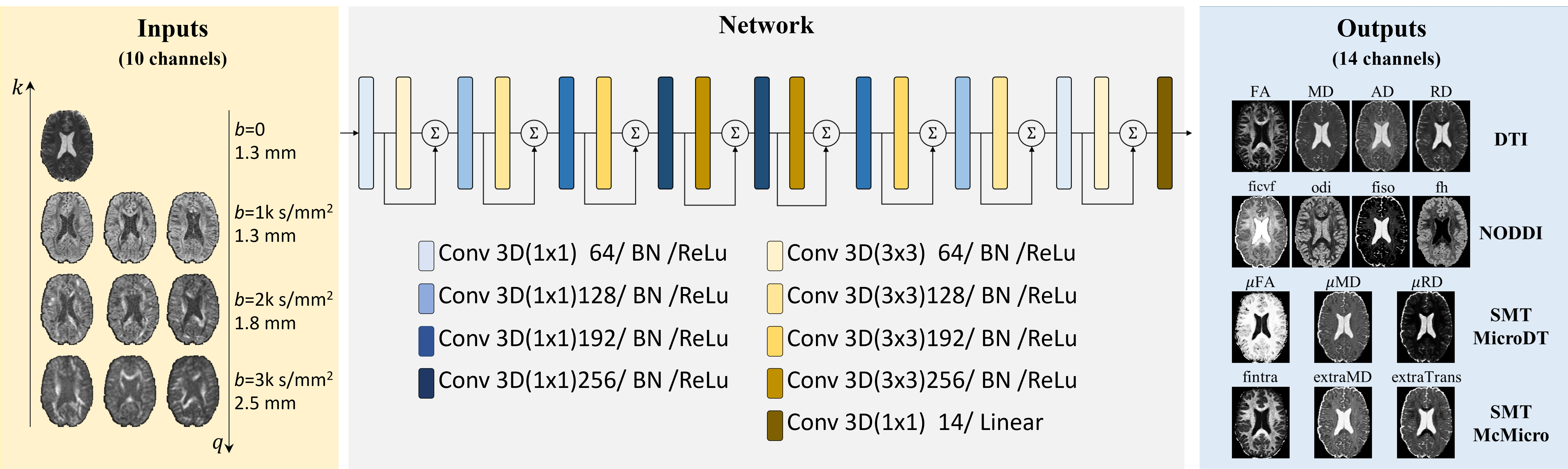
Fig. 1. The illustration of the input, network structure, and output of the DeepHIBRID.
The input of the network using the HIBRID sampling scheme with the image resolution gradually decrease as the b-value increase. The batch normalization and residual learning were added to the network structure. The network outputted the 14 different diffusion metric maps at the same resolution with b0 and b1k images.
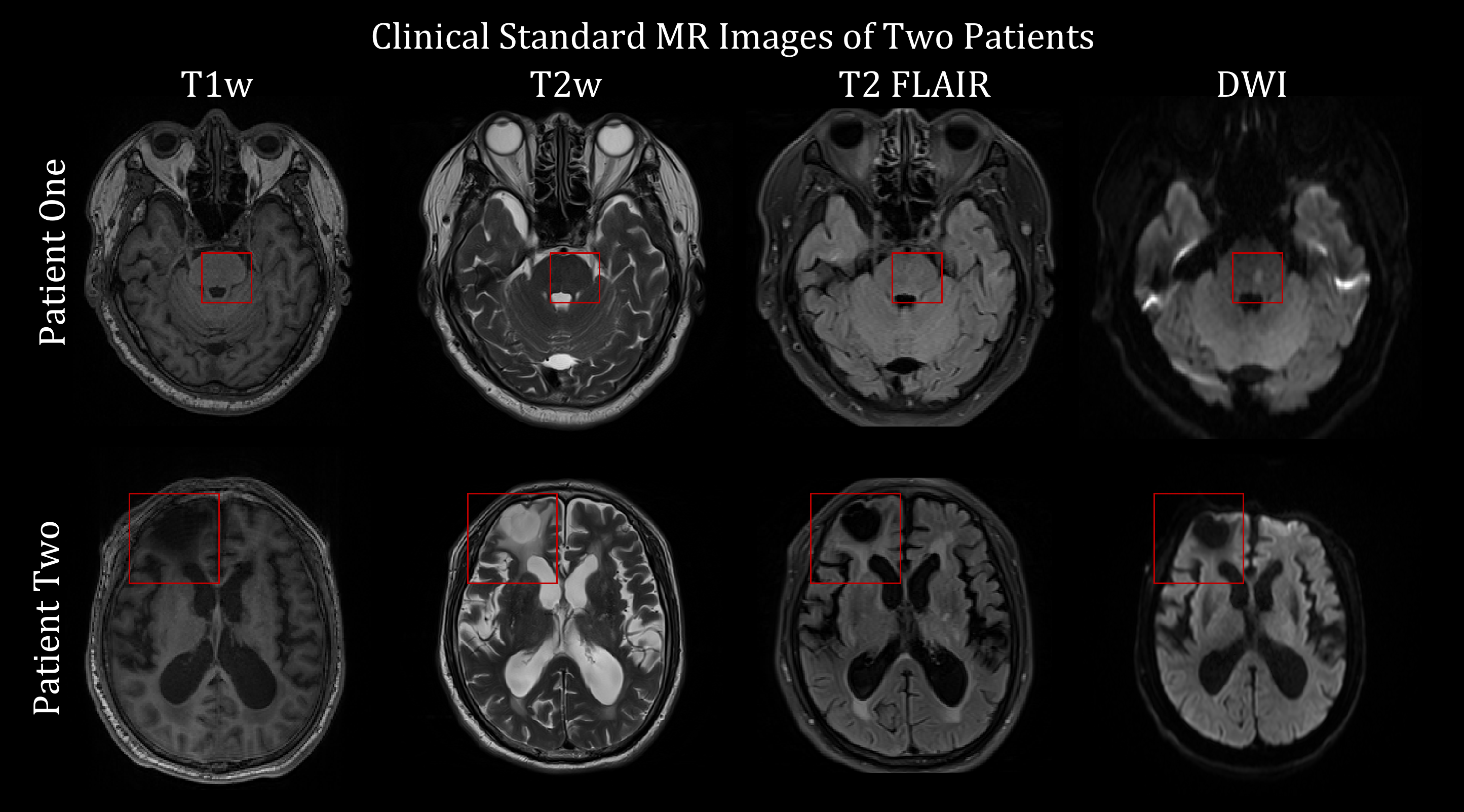
Fig. 2. The four MR modality images used in the clinical standard operation protocol of the two patients.
The T1w, T2w, and T2 FLAIR images were sampled with an in-plane resolution of 0.65mm and 5mm slice thickness. The DWI image shown here was also sampled with 0.65mm in-plane resolution and 5mm slice thickness using b=1000 s/mm2.
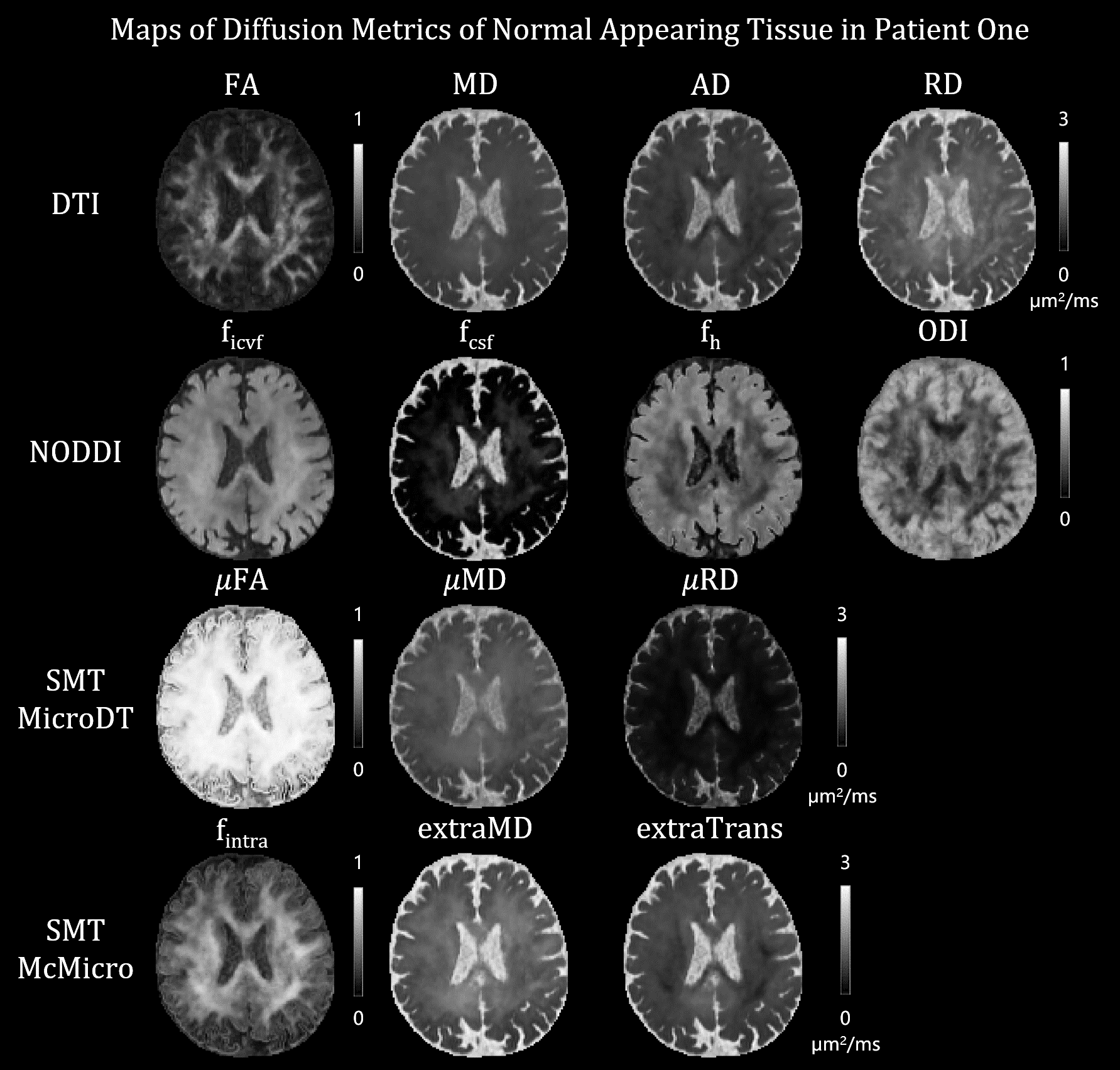
Fig. 3. The predicted 14 diffusion metric maps of the normal appearing tissue from patient two at the 1.3mm iso. resolution.
The diffusion metrics were largely as expected in different tissues of the brain.
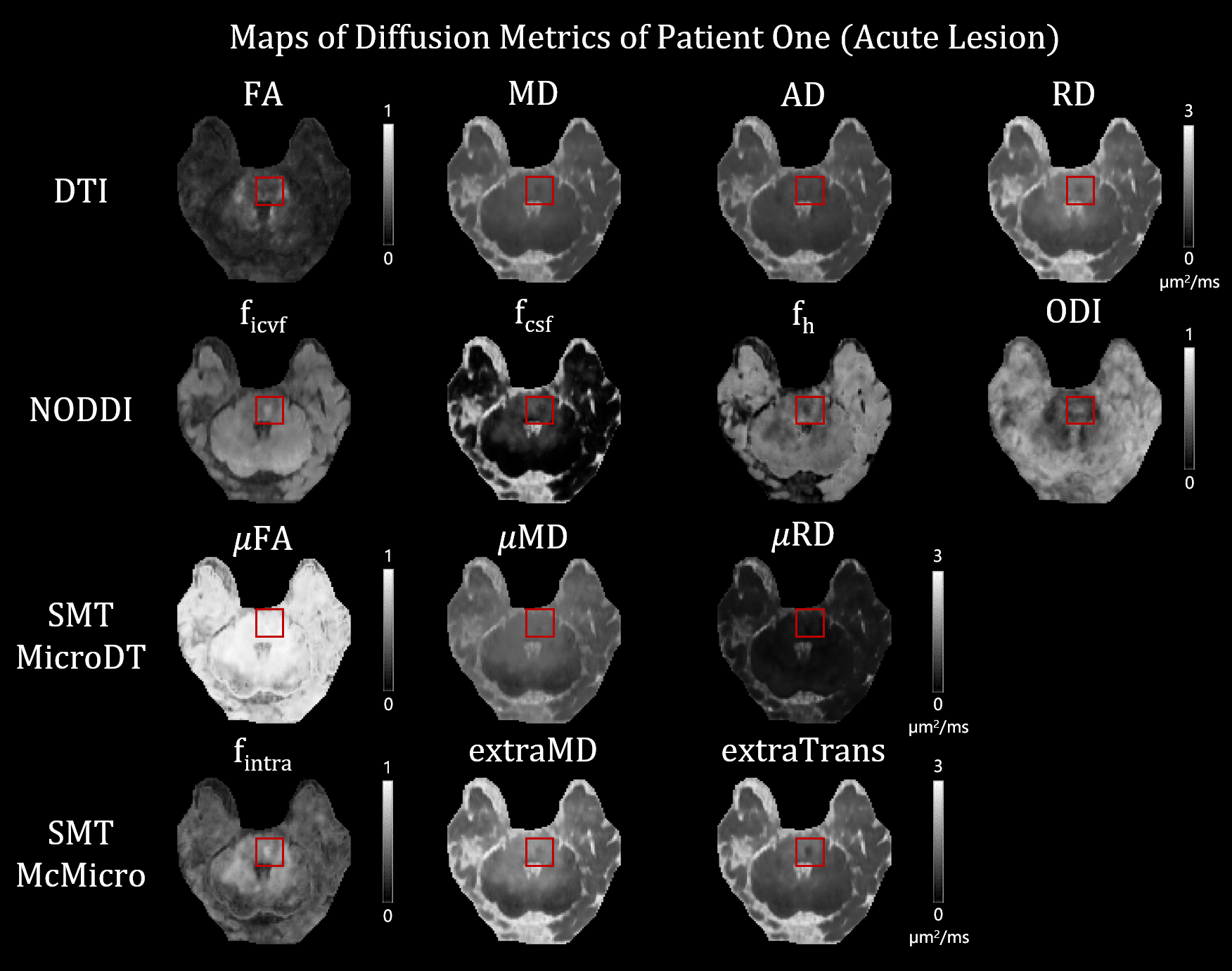
Fig. 4. The predicted 14 diffusion metric maps of the acute stroke lesion.
The stroke lesion was labeled in the red box and situated in the right pons. In the acute period of ischemic stroke, the cytotoxic edema effects were well captured by the DeepHIBRID network with increased ficvf and fintra as well as decreased extraMD, extraTrans, and fcsf.
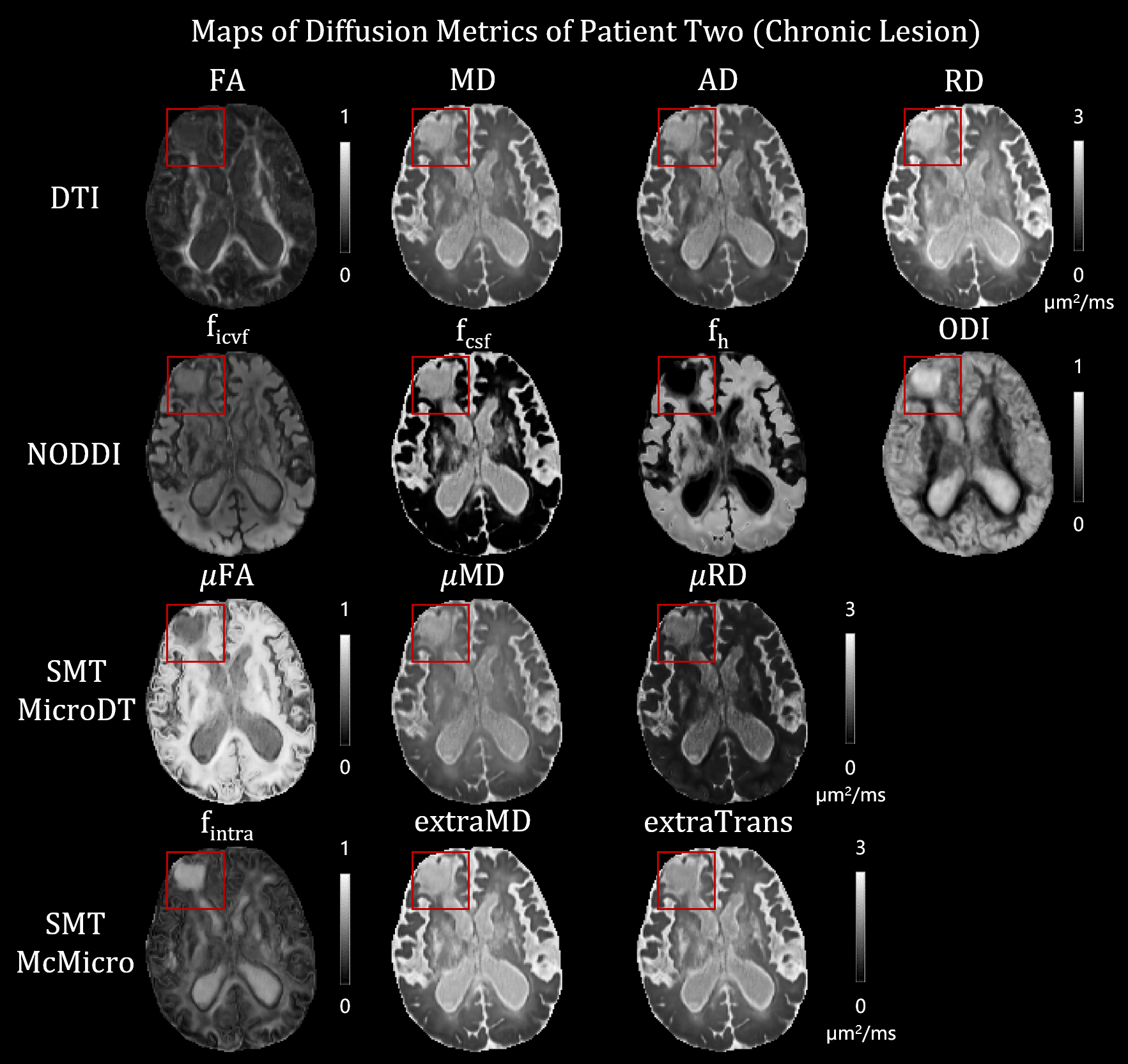
Fig. 5. The predicted diffusion metric maps of the chronic stroke lesion.
The stroke lesion labeled in the red box was located in the left frontal lobe and surrounded by the edema tissue. Within the chronic lesion of the stroke patient, observant contrast could be found against the collateral healthy tissue, exhibiting comparable metric values with the CSF compartment.