5095
Evaluation of kidney injury using ASL and BOLD MRI: an experimental study in rats with CCl4-induced liver cirrhosis1The School of Medicine, Nankai Univeisity, Tianjin, China, 2Department of Radiology, Tianjin First Central Hospital, Tianjin, China, 3Weihai Central Hospital, Weihai, China, 4Department of Radiology, Nankai Univeisity, Tianjin, China, 5Tianjin Medical University, Tianjin, China, 6Tianjin First Central Hospital, Tianjin, China, 7Nankai Univeisity, Tianjin, China, 8Siemens Healthineers, Beijing, China, 9Siemens Healthineers AG, Erlangen, Germany
Synopsis
Keywords: fMRI Analysis, Animals
Motivation: Noninvasive and sensitive methods for assessing chronic liver disease-associated kidney injury are needed in clinics.
Goal(s): We investigated the potential of arterial spin labeling (ASL) and blood oxygenation level-dependent (BOLD) MRI for diagnosing and evaluating chronic liver disease-associated kidney injury progression.
Approach: We observed the renal blood flow (RBF) and T2* changes in rats with CCl4-induced chronic liver disease and compared imaging, pathological, and biochemical indicators at different time points.
Results: During chronic liver disease development in rats, RBF and T2* gradually decreased, and ASL and BOLD MRI were more sensitive than serum creatinine in diagnosing renal injury.
Impact: Compared with serum creatinine, ASL and BOLD MRI exhibited more sensitive diagnostic value for liver cirrhosis-associated renal injury, providing a noninvasive and reliable method for monitoring kidney injury in patients with chronic liver disease.
Introduction
Kidney injury is a common complication of decompensated cirrhosis, occurring in 30%–50% of hospitalized patients and seriously affecting patients’ prognoses1,2. Previous studies have shown that acute kidney injury in patients with cirrhosis is likely to lead to development of chronic kidney disease and progressive loss of kidney function3-5. Early diagnosis and treatment can delay the progression of kidney injury and improve prognoses. The pathophysiological mechanisms underlying kidney injury in patients with chronic liver disease are intricate. Previous studies have indicated that alterations in renal hemodynamics leading to changes in oxygenation status and inflammatory states are the primary causative factors contributing to kidney injury11-13. Arterial spin labeling (ASL) is a noninvasive and reliable technique for assessing organ blood perfusion without requiring contrast agent injection14-17. The blood oxygenation level-dependent (BOLD) response is highly sensitive to tissue hypoxia and allows effectively evaluating tissue oxygenation status18,19. Increasing studies have used these techniques to noninvasively detect changes in renal perfusion and renal hypoxia in acute kidney injury, renal allografts, chronic kidney disease, and metabolic syndrome19-25. However, these techniques remain limited in their assessment of renal damage in liver cirrhosis, and relevant research is lacking; thus, the value of these techniques remains uncertain. This study was conducted to investigate whether ASL and BOLD magnetic resonance imaging (MRI) can detect alterations in renal hemodynamics and blood oxygenation in chronic liver disease, thereby providing early indicators for kidney injury and offering a reliable basis for early clinical detection and intervention.Methods
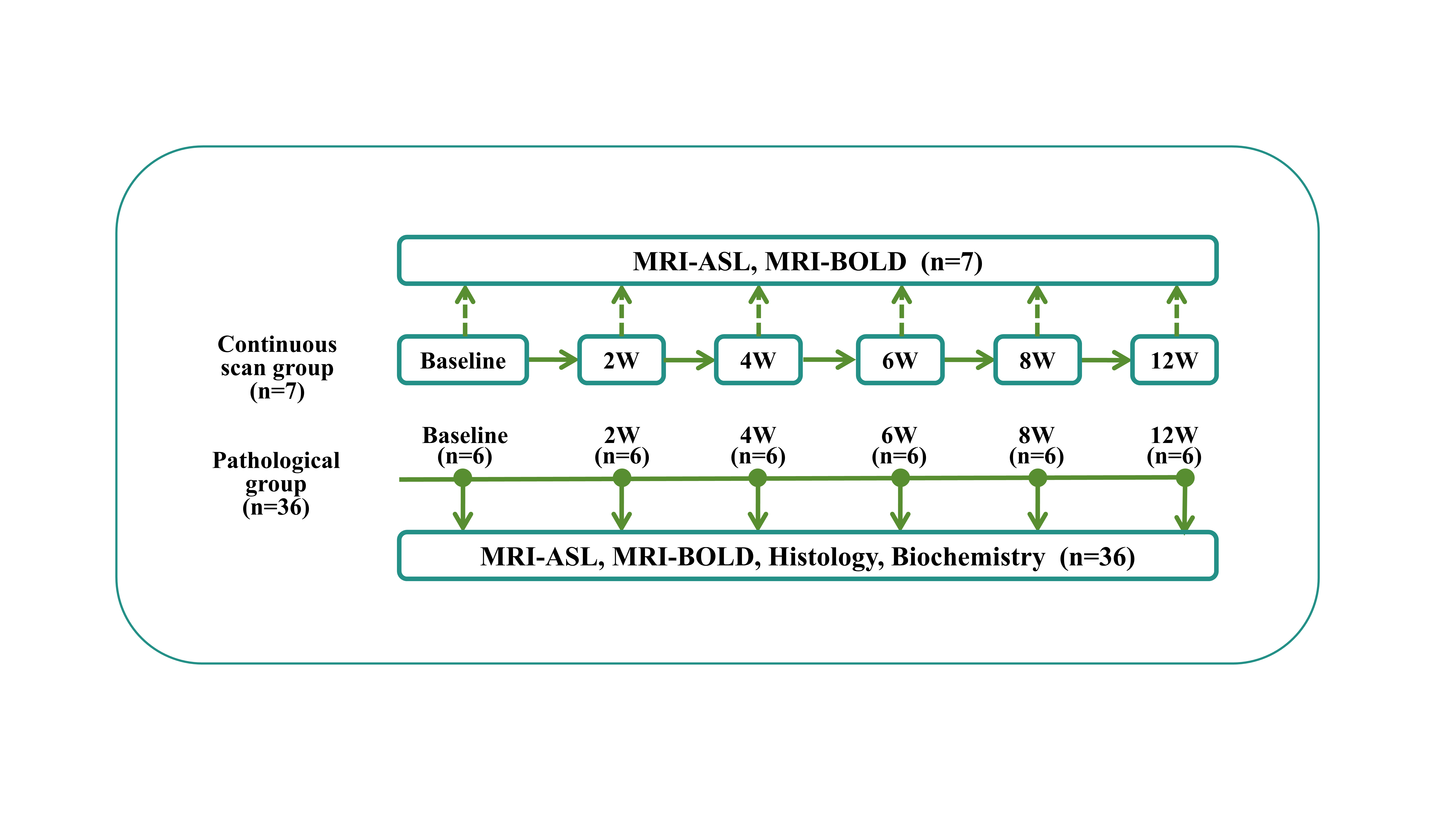
Liver cirrhosis was induced via subcutaneous carbon tetrachloride (CCl4) injection twice weekly for 12 weeks. Thirty-six rats underwent renal MRI followed by pathological analysis at baseline and 2, 4, 6, 8, and 12 weeks (n=6 rats/group/time point). Seven rats underwent MRI examinations at all time points. All MRI examinations were performed on a 3T MRI system (MAGNETOM Prisma, Siemens Healthineers, Erlangen, Germany) equipped with a dedicated eight-channel animal coil (Chenguang, Shanghai, China). Renal ASL was performed using a research three-dimensional turbo gradient spin echo pulsed ASL sequence with the following parameters: repetition time/echo time (TR/TE): 6000/49.86 ms, field of view (FOV): 153 × 153 mm2, slice thickness: 3.00 mm, slice number: 8, matrix: 64 × 64, voxel size reconstructed to 1.2 × 1.2 × 3 mm3, 7 inversion times: 300/500/700/900/1100/1300/1500 ms, bolus length: 700 ms, and acquisition time: 7 min. BOLD MRI was acquired using a multiple echo gradient echo sequence with the following parameters: TR: 255 ms, 6 echoes equally spaced (3.22–16.22 msec), FOV: 85 × 85 mm2, slice thickness: 3.00 mm, matrix: 192 × 154, and acquisition time: 4 minutes. Quantitative renal blood flow (RBF) and T2* maps were generated inline after data acquisition. Mean renal perfusion and T2* were manually calculated by selecting the regions of interest (ROIs) on the corresponding parametric maps. Radiological, biochemical, and pathological indicators were analyzed (Figure 1), and p<0.05 was considered statistically significant.Results
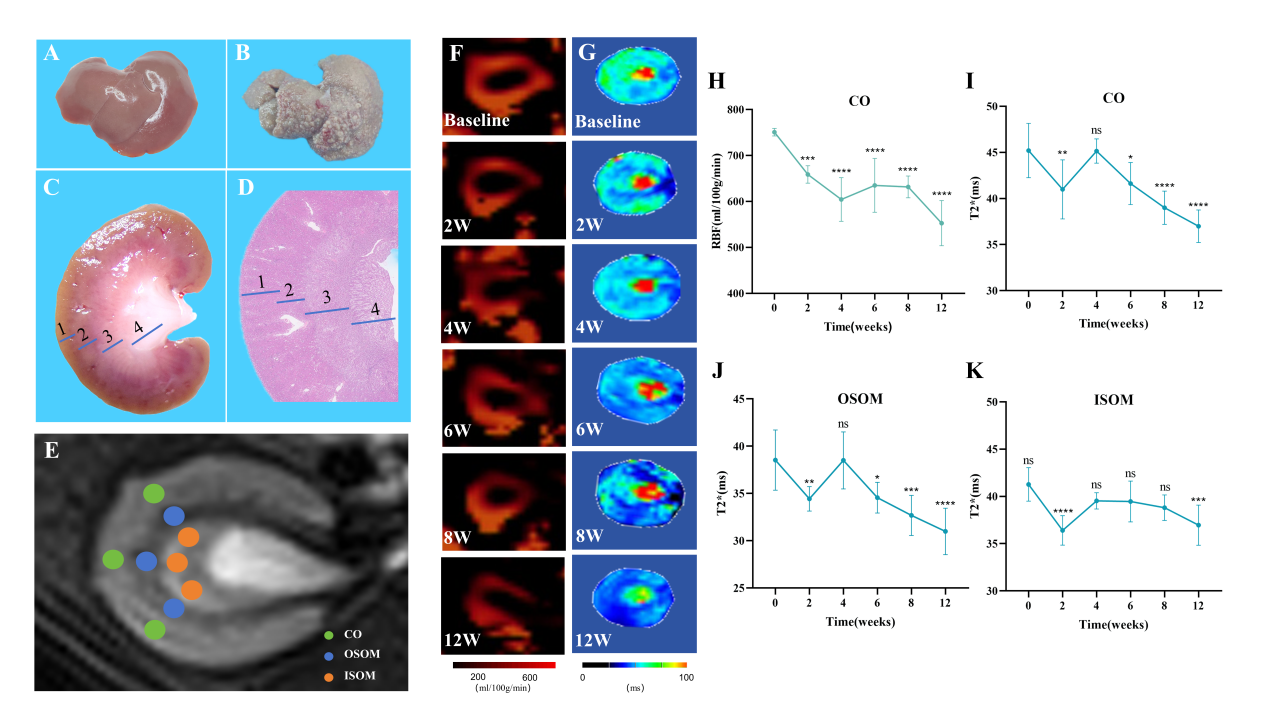
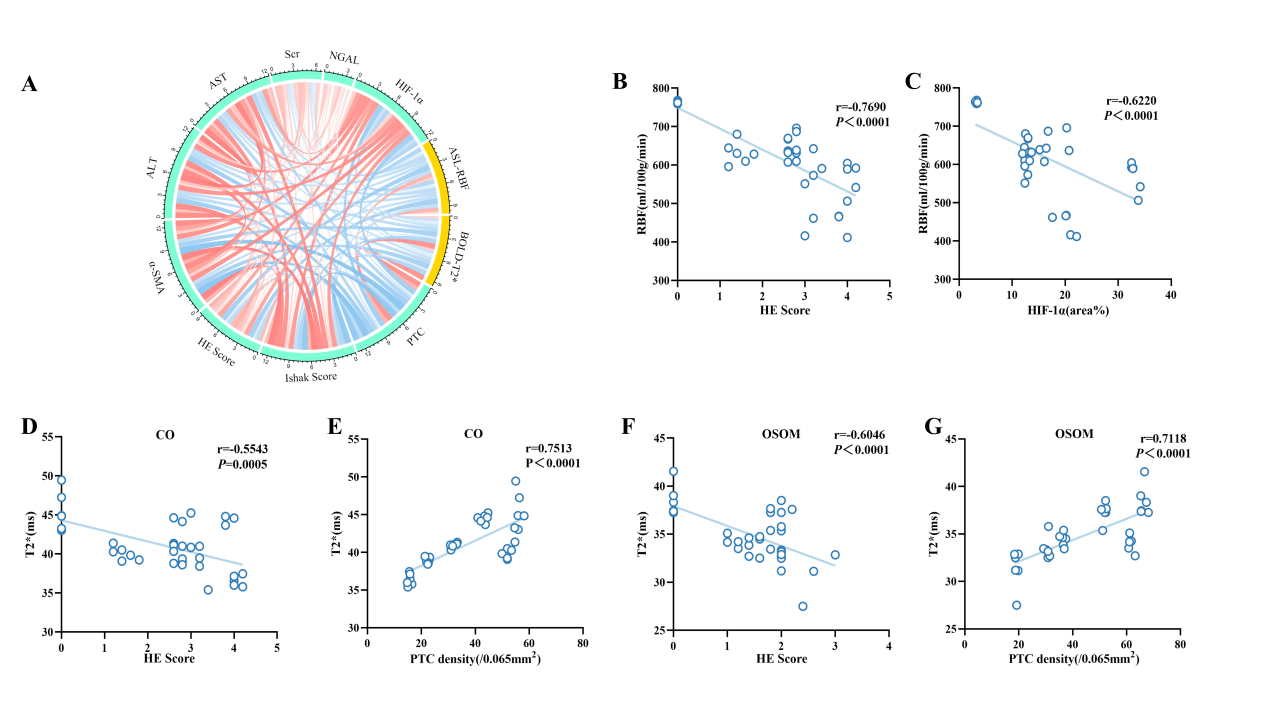
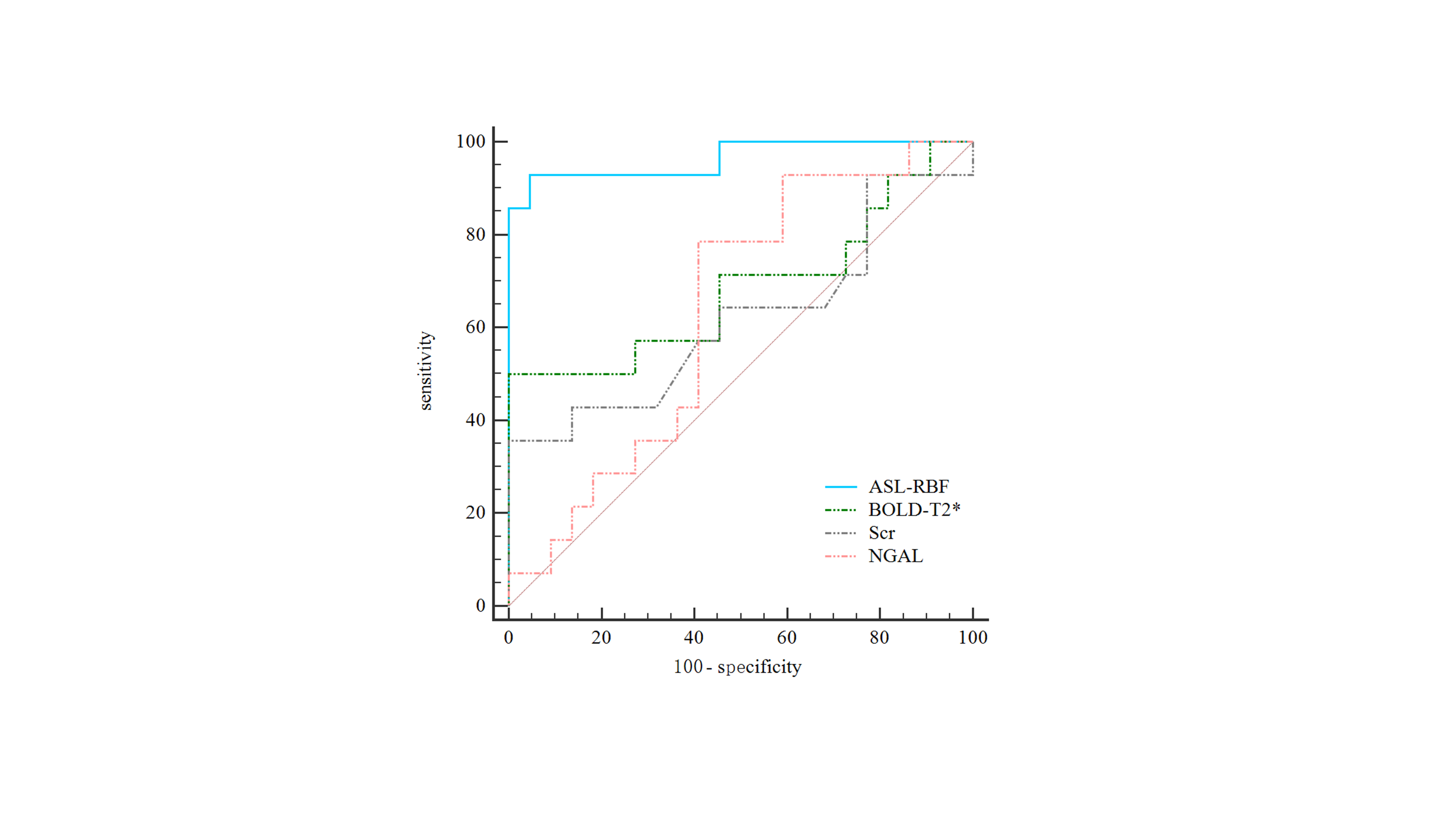
RBF in the renal cortex and T2* in all anatomical compartments differed significantly among all time points (all p<0.05; Figure 2). From 6–12 weeks after modeling, RBF and T2* in the renal cortex and T2* in the renal outer stripe of the outer medulla were significantly lower than those at baseline. Both RBF and T2* were significantly correlated with renal injury pathological scores, α-smooth muscle actin, hypoxia-inducible factor (HIF)1-α, and peritubular capillary density (|r|=0.406–0.853; Figure 3). RBF demonstrated superior diagnostic capability in identifying severe kidney injury in chronic liver disease compared with the diagnostic capabilities of T2*, serum creatinine, and neutrophil gelatinase-associated lipocalin (area under the curve: 0.964; Figure 4).Discussion
Our results showed that compared with serum creatinine, ASL and BOLD MRI enable earlier detecting and monitoring of chronic liver disease-associated renal injury. RBF, T2*, renal hematoxylin and eosin score, renal microvessel density, and HIF-1α were all significantly correlated, indicating that ASL and BOLD MRI can effectively reflect the reductions in renal blood perfusion and oxygenation leading to renal injury in chronic liver disease. RBF showed the best diagnostic performance of all tested indicators for diagnosing severe and non-severe renal injuries.Conclusion
Both ASL and BOLD MRI are effective imaging tools for monitoring kidney injury during liver cirrhosis progression. Cortical RBF is a key indicator for early and advanced kidney injury.Acknowledgements
The authors thank Siemens Healthcare for providing the prototypic renal ASL and BOLD sequence and technical support.References
1 Ginès P, Solà E, Angeli P, et al. Hepatorenal syndrome. Nat Rev Dis Primers. 2018;4:23.2 Huelin P, Piano S, Solà E et al (2017) Validation of a Staging System for Acute Kidney Injury in Patients With Cirrhosis and Association With Acute-on-Chronic Liver Failure. Clin Gastroenterol Hepatol 15:438-445.e4353 Bassegoda O, Huelin P, Ariza X et al (2020) Development of chronic kidney disease after acute kidney injury in patients with cirrhosis is common and impairs clinical outcomes. J Hepatol 72:1132-11394 Maiwall R, Pasupuleti SSR, Bihari C et al (2020) Incidence, Risk Factors, and Outcomes of Transition of Acute Kidney Injury to Chronic Kidney Disease in Cirrhosis: A Prospective Cohort Study. Hepatology 71:1009-10225 Patidar KR, Naved MA, Grama A et al (2022) Acute kidney disease is common and associated with poor outcomes in patients with cirrhosis and acute kidney injury. J Hepatol 77:108-1156 Shields J, Maxwell AP (2010) Managing diabetic nephropathy. Clin Med (Lond) 10:500-5047 Bräsen JH, Mederacke YS, Schmitz J et al (2019) Cholemic Nephropathy Causes Acute Kidney Injury and Is Accompanied by Loss of Aquaporin 2 in Collecting Ducts. Hepatology 69:2107-21198 Khawaja S, Jafri L, Siddiqui I, Hashmi M, Ghani F (2019) The utility of neutrophil gelatinase-associated Lipocalin (NGAL) as a marker of acute kidney injury (AKI) in critically ill patients. Biomark Res 7:49 Velez JCQ, Therapondos G, Juncos LA (2020) Reappraising the spectrum of AKI and hepatorenal syndrome in patients with cirrhosis. Nat Rev Nephrol 16:137-15510 Zhang H, Wang P, Shi D et al (2022) Capability of intravoxel incoherent motion and diffusion tensor imaging to detect early kidney injury in type 2 diabetes. Eur Radiol 32:2988-299711 Francoz C, Durand F, Kahn JA, Genyk YS, Nadim MK (2019) Hepatorenal Syndrome. Clin J Am Soc Nephrol 14:774-78112 Schrier RW, Arroyo V, Bernardi M, Epstein M, Henriksen JH, Rodés J (1988) Peripheral arterial vasodilation hypothesis: a proposal for the initiation of renal sodium and water retention in cirrhosis. Hepatology 8:1151-115713 Nadim MK, Garcia-Tsao G (2023) Acute Kidney Injury in Patients with Cirrhosis. N Engl J Med 388:733-74514 Laothamatas I, Al Mubarak H, Reddy A et al (2023) Multiparametric MRI of Solid Renal Masses: Principles and Applications of Advanced Quantitative and Functional Methods for Tumor Diagnosis and Characterization. J Magn Reson Imaging 58:342-35915 Yu Y, Xie S, Wang K et al (2022) Perfusion Analysis of Kidney Injury in Rats With Cirrhosis Induced by Common Bile Duct Ligation Using Arterial Spin Labeling MRI. J Magn Reson Imaging 55:1393-140416 Huhndorf M, Eimer C, Becher T et al (2023) Effect of General Anesthesia on Cerebral Blood Flow Measured by Arterial Spin Labeling: A Retrospective Study. J Magn Reson Imaging 58:663-66517 Herrera CL, Wang Y, Udayakumar D et al (2023) Longitudinal assessment of placental perfusion in normal and hypertensive pregnancies using pseudo-continuous arterial spin-labeled MRI: preliminary experience. Eur Radiol. 10.1007/s00330-023-09945-x18 Pruijm M, Milani B, Burnier M (2016) Blood Oxygenation Level-Dependent MRI to Assess Renal Oxygenation in Renal Diseases: Progresses and Challenges. Front Physiol 7:66719 Zhang B, Wang Y, Wang C et al (2019) Comparison of blood oxygen level-dependent imaging and diffusion-weighted imaging in early diagnosis of acute kidney injury in animal models. J Magn Reson Imaging 50:719-72420 Niles DJ, Artz NS, Djamali A, Sadowski EA, Grist TM, Fain SB (2016) Longitudinal Assessment of Renal Perfusion and Oxygenation in Transplant Donor-Recipient Pairs Using Arterial Spin Labeling and Blood Oxygen Level-Dependent Magnetic Resonance Imaging. Invest Radiol 51:113-12021 Mora-Gutiérrez JM, Garcia-Fernandez N, Slon Roblero MF et al (2017) Arterial spin labeling MRI is able to detect early hemodynamic changes in diabetic nephropathy. J Magn Reson Imaging 46:1810-181722 Hueper K, Gutberlet M, Rong S et al (2014) Acute kidney injury: arterial spin labeling to monitor renal perfusion impairment in mice-comparison with histopathologic results and renal function. Radiology 270:117-12423 Mao W, Ding Y, Ding X et al (2023) Capability of arterial spin labeling and intravoxel incoherent motion diffusion-weighted imaging to detect early kidney injury in chronic kidney disease. Eur Radiol 33:3286-329424 Liang P, Yuan G, Li S et al (2023) Noninvasive Assessment of the Renal Function, Oxford Classification and Prognostic Risk Stratification of IgAN by Using Intravoxel Incoherent Motion Diffusion-Weighted Imaging and Blood Oxygenation Level-Dependent MRI. J Magn Reson Imaging 58:879-89125 Buchanan C, Mahmoud H, Cox E et al (2021) Multiparametric MRI assessment of renal structure and function in acute kidney injury and renal recovery. Clin Kidney J 14:1969-1976Figures