5076
Feasibility of Volumetric Multiple-Breath Washout 19F-Perfluoropropane Ventilation Mapping of the Lung in Healthy Children1Medical Biophysics, University of Toronto, Toronto, ON, Canada, 2Translational Medicine, The Hospital for Sick Children, Toronto, ON, Canada, 3Newcastle University, Newcastle upon Tyne, United Kingdom, 4Division of Respiratory Medicine, The Hospital for Sick Children, Toronto, ON, Canada
Synopsis
Keywords: Non-Proton, Pediatric, lung
Motivation: Multiple-breath washout (MBW) MRI following exhalation of a tracer gas results in regional maps of fractional ventilation (FV). Using perfluoropropane (PFP) gas allows for long washout experiments which may provide useful clinical insight on slow-filling regions of diseased lungs, particularly in children.
Goal(s): Test feasibility of MBW PFP-MRI in pediatric healthy participants, investigate gravitational dependence of FV.
Approach: 3 healthy pediatric participants were imaged using 3D broad-banded 19F-MRI and the following MBW maneuver: 6 inhalations of PFP gas mixture, then wash-out with room air with 8s MR-images every second breath.
Results: MBW PFP-MRI was feasible in children. The gravitational gradient was as expected.
Impact: The ability of PFP to be mixed with oxygen and the fact that it is thermally polarized makes longer MBW studies possible and thus has the potential to improve tolerance by younger subjects and those with more advanced lung disease.
Introduction
Novel therapies for cystic fibrosis (CF) lung disease are promising for delaying disease progression and most effective when initiated in children, before functional decline begins. However, standard pulmonary function tests are normal in children[1]. The lung clearance index (LCI) derived from nitrogen (N2) multiple-breath washout (MBW) is an at-the-mouth test that discriminates health from pediatric CF but misses regional information which limits its sensitivity[2].Performing MRI during washout following inhalation of hyperpolarized 129Xe gas results in regional maps of fractional ventilation (FV), measuring gas clearance/breath[3,4]. Regional information makes MBW Xe-MRI potentially more sensitive to disease progression. However, depolarization interactions with oxygen prevent acquisition of longer wash-out which may provide more useful clinical insight. MBW 19F-MRI using perfluoropropane (PFP) gas is an attractive alternative because its high gyromagnetic ratio, high spin density and short T1 relaxation time allows for sufficient signal, enabling extended free-breathing and access to slower washout regions. The compatibility of PFP with oxygen facilitates its clinical translation, especially in children. Its feasibility in adults has been demonstrated[5], but not yet tested in children.
In this work, we test the feasibility of MBW PFP-MRI in pediatric healthy participants and investigated gravitational dependence of FV.
Methods
In this feasibility study, three healthy children (mean age 12.3±1) were recruited with institutional Research Ethics Board and Health Canada approval. Written informed consent/assent was obtained from all parents/participants.19F-MRI was performed on a 3T MRI system (Prisma, Siemens, Erlangen, Germany) with a rigid elliptical birdcage transmitter/flexible 8-channel receiver (Rapid Biomedical, Rimpar, Germany). Participants inhaled clinical grade 79% perfluoropropane/21% oxygen gas mixture (Airgas Therapeutics, Pennsylvania) during each ~3-minute acquisition comprising (Figure 1): 6 deep breaths of the gas through a non-rebreathing valve and mouthpiece (Hans Rudolph, Shawnee, Kansas), followed by a switch to room air and 8s breath-hold 19F-MRI images (acquired at functional residual capacity plus tidal volume) every second breath until the signal was depleted (8 breaths/5 images).
Images were acquired using a 3D multi-nuclear (19F-MRI) broad-banded gradient echo sequence with parameters: slices=16, slice thickness=15 mm, TR=8.7 ms, TE=1.75 ms, FA=45°, FOV=360x480 mm, matrix=36x48, bandwidth=668 Hz/pixel, averages=3, acceleration factor 2, 12 reference lines, reconstructed using GeneRalized Autocalibrating Partial Parallel Acquisition (GRAPPA).
FV was calculated by fitting a mono-exponential equation[6] to the washout images on a pixel-wide basis. Mean FV was used to represent FV for a given slice, plotted against the distance from the posterior lung to investigate gravitational dependence of ventilation.
Results
Table 1 shows participant demographics. PFP gas mixture and breathing maneuvers were well-tolerated by all participants.Figure 2 shows representative washout images of the center slice for each participant.
Figure 3 contains FV maps for all 8-10 slices of each participant, anterior (left) to posterior (right). Median [IQR] FV for the 3 participants were 0.37 [0.36 0.43], 0.22 [0.22 0.25] and 0.22 [0.21 0.24], respectively.
A negative gradient in FV was observed in the posterior/anterior direction for all participants. Gradient slope (cm-1) for participants 1-3 were -0.0236, -0.0066 and -0.0124, respectively (mean gradient -0.0142±0.009). Figure 4 shows a representative gradient.
Discussion
This preliminary work presents the first FV maps obtained in children using 19F-MRI of PFP gas washout.The washout observation period was twice as long as previous work using multiple-slice MBW Xe-MRI, where 5 images/8 breaths were acquired instead of 4 images/4 breaths[8]. This is owed to the thermally-polarized 19F signal and normoxic gas mixture, unaffected by T1- and RF-mediated polarization losses encountered in hyperpolarized MRI.
The measured FV for participant 1 are consistent with similar healthy volunteers using xenon, with median [IQR] FV 0.35 [0.31 0.50] in single-slice[4] and 0.35 [0.30 0.36] in multi-slice[7]. However, participants 2 and 3 have lower FV than expected. This may result from the different PFP-MRI breathing maneuver allowing for smaller tidal breaths between images compared to the consistent deep breaths of Xe-MRI. Stricter coaching and/or faster imaging may allow for more consistency in breathing maneuvers between participants.
The average gradient is consistent with Xe-MRI studies in healthy adults[8] and with the known deformation of the lung due to gravity in the supine position, resulting in more efficient washout (higher FV) in the dependent (posterior) lung[9].
Washin was limited to 6 breaths. In future, we anticipate using ~12 washin breaths to capture slow-filling regions of disease. Participant fatigue may be a concern in sicker children due to repeated long breath-holds. Incorporating compressed sensing allows for shortened scan durations which may increase tolerability of longer washouts in children.
Conclusion
Volumetric MBW PFP-MRI is feasible in healthy pediatric volunteers, and the gravitational gradient is consistent with MBW Xe-MRI.Acknowledgements
This study was funded by the Canadian Institute for Health Research (CIHR). Faiyza Alam was supported by a Restracomp award from SickKids Research Institute.
References
1. CF foundation. (2022). Cystic Fibrosis Foundation Patient Registry Highlights [Ebook] (p. 1). Bethesda: Cystic Fibrosis Foundation. Retrieved from https://www.cff.org/medical-professionals/patient-registry.
2. Stanojevic, S., Davis, S., Retsch-Bogart, G., Webster, H., Davis, M., & Johnson, R. et al. (2017). Progression of Lung Disease in Preschool Patients with Cystic Fibrosis. American Journal Of Respiratory And Critical Care Medicine, 195(9), 1216-1225. Doi: 10.1164/rccm.201610-2158oc
3. Couch, M., Morgado, F., Kanhere, N., Kowalik, K., Rayment, J., Ratjen, F., & Santyr, G. (2019). Assessing the feasibility of hyperpolarized 129 Xe multiple‐breath washout MRI in pediatric cystic fibrosis. Magnetic Resonance In Medicine, 84(1), 304-311. doi: 10.1002/mrm.28099
4. Alam, F., Zanette, B., Braganza, S., Li, D., Ratjen, F., & Santyr, G. (2022). Intra-Visit and Inter-Visit Repeatability of 129Xe Multiple-Breath Washout MRI in Children with Stable Cystic Fibrosis Lung Disease. International Society of Magnetic Resonance in Medicine (ISMRM), 2022.
5. Goralski, J. L., Chung, S. H., Glass, T. M., Ceppe, A. S., Akinnagbe-Zusterzeel, E. O., Trimble, A. T., Boucher, R. C., Soher, B. J., Charles, H. C., Donaldson, S. H., & Lee, Y. Z. (2020). Dynamic perfluorinated gas MRI reveals abnormal ventilation despite normal FEV1 in cystic fibrosis. JCI Insight, 5(2). https://doi.org/10.1172/jci.insight.133400
6. Couch, M. J., Fox, M. S., Viel, C., Gajawada, G., Li, T., Ouriadov, A. V., & Albert, M. S. (2016). Fractional ventilation mapping using inert fluorinated gas MRI in rat models of inflammation and fibrosis. NMR in Biomedicine, 29(5), 545–552. https://doi.org/10.1002/nbm.3493
7. Alam, F., Couch, M., Zanette, B., Li, D., Ratjen, F., & Santyr, G. (2023). Multiple-Slice, Multiple-Breath Washout Hyperpolarized 129Xe Ventilation Mapping of the Lung using Accelerated Data Acquisition. International Society of Magnetic Resonance in Medicine (ISMRM), 2023. #4103.
8. Horn, F. C., Deppe, M. H., Marshall, H., Parra-Robles, J., & Wild, J. M. (2014). Quantification of regional fractional ventilation in human subjects by measurement of hyperpolarized 3he washout with 2D and 3D MRI. Journal of Applied Physiology, 116(2), 129-139. doi:10.1152/japplphysiol.00378.2013
9. Sá, R. C., Cronin, M. V., Cortney Henderson, A., Holverda, S., Theilmann, R. J., Arai, T. J., & Kim Prisk, G. (2010). Vertical distribution of specific ventilation in normal supine humans measured by oxygen-enhanced Proton MRI. Journal of Applied Physiology, 109(6), 1950-1959. doi:10.1152/japplphysiol.00220.2010
10. Thomen, R., Walkup, L., Roach, D., Cleveland, Z., Clancy, J., & Woods, J. (2017). Hyperpolarized 129Xe for investigation of mild cystic fibrosis lung disease in pediatric patients. Journal Of Cystic Fibrosis, 16(2), 275-282. doi: 10.1016/j.jcf.2016.07.008
Figures
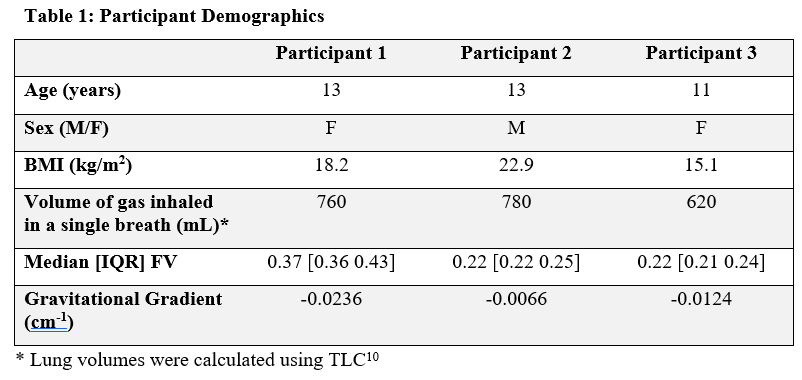
Table 1: Participant Demographics
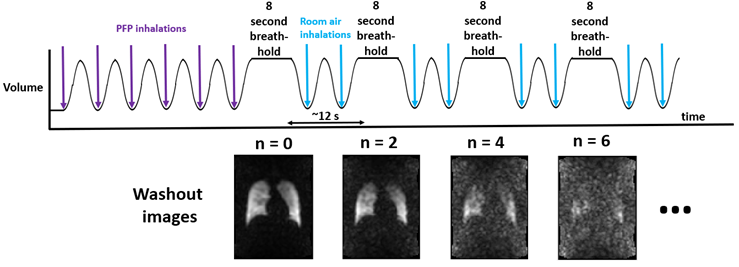
Figure 1: MBW PFP-MRI Method.
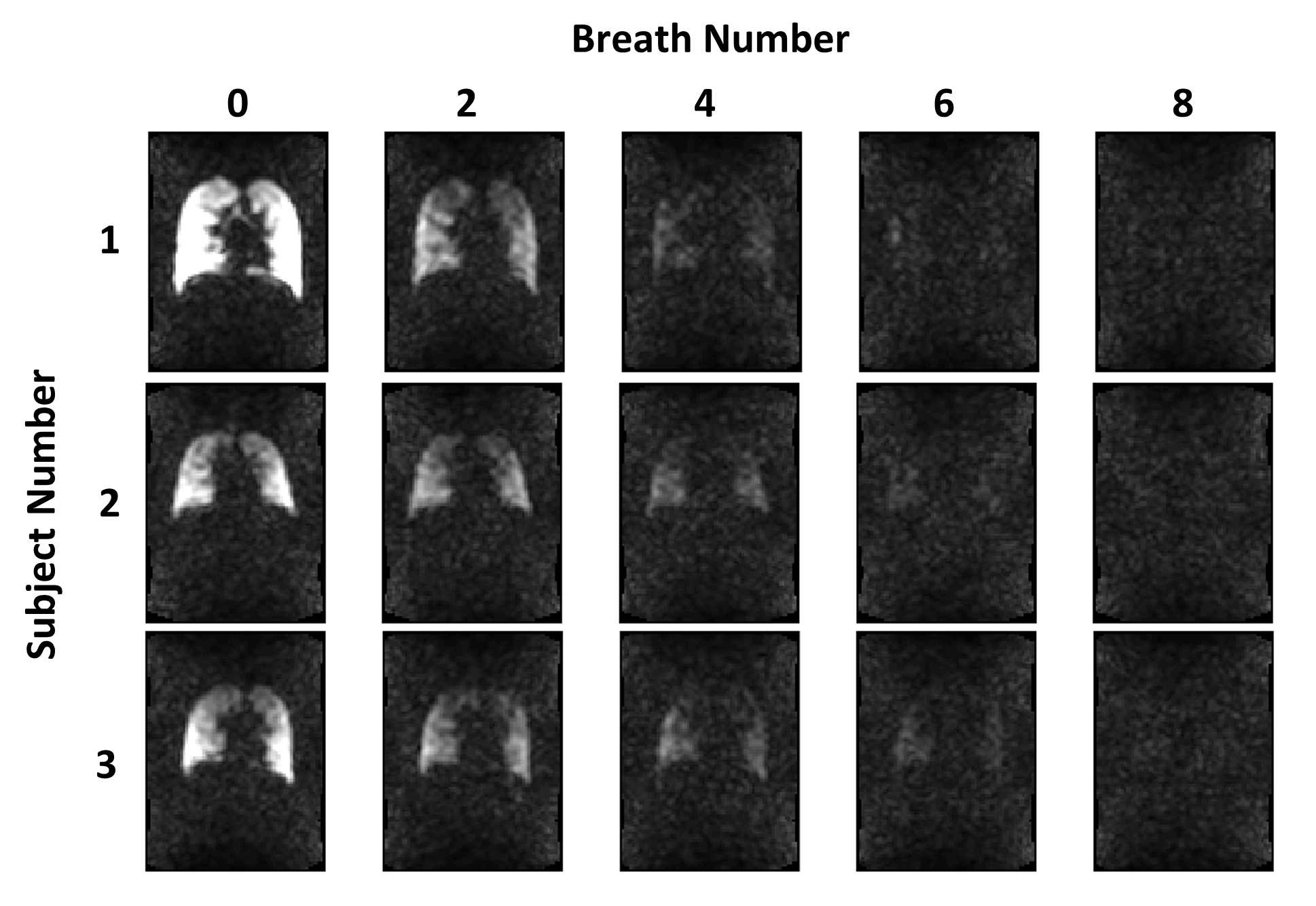
Figure 2: Representative washout for a center slice (slice number 5) from each subject (from top to bottom: participant 1, 2 and 3). Image 1 represents the first image on the 6th inhalation of PFP gas, with subsequent images representing every second breath number.
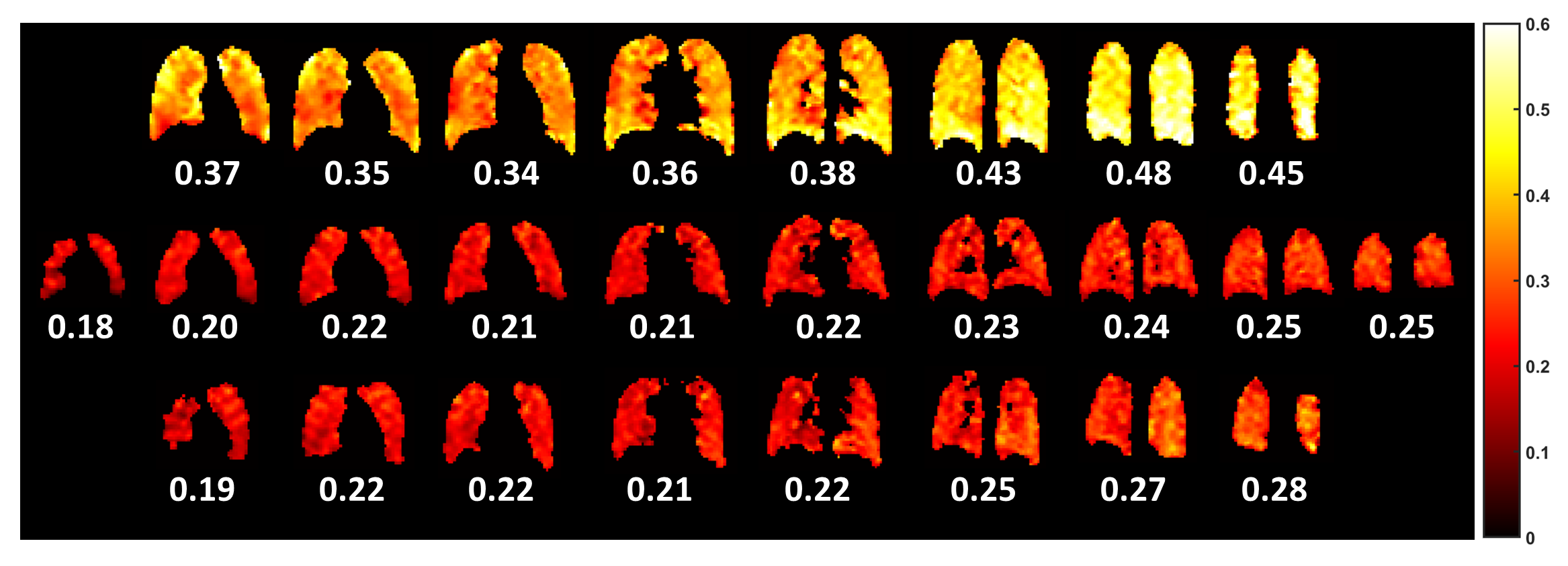
Figure 3: FV maps associated with each of the 8-10 slices from anterior (left) to posterior (right) for participant 1 (top), participant 2 (middle) and participant 3 (bottom). A scale bar for FV is on the far right with 0 representing no gas turnover in one breath, and 0.6 representing 60% gas replacement per breath. Large airways are masked. The mean FV value of each map is shown below each slice. Each FV map is calculated from the series of MBW PFP-MRI images for each individual slice (see Fig. 2).
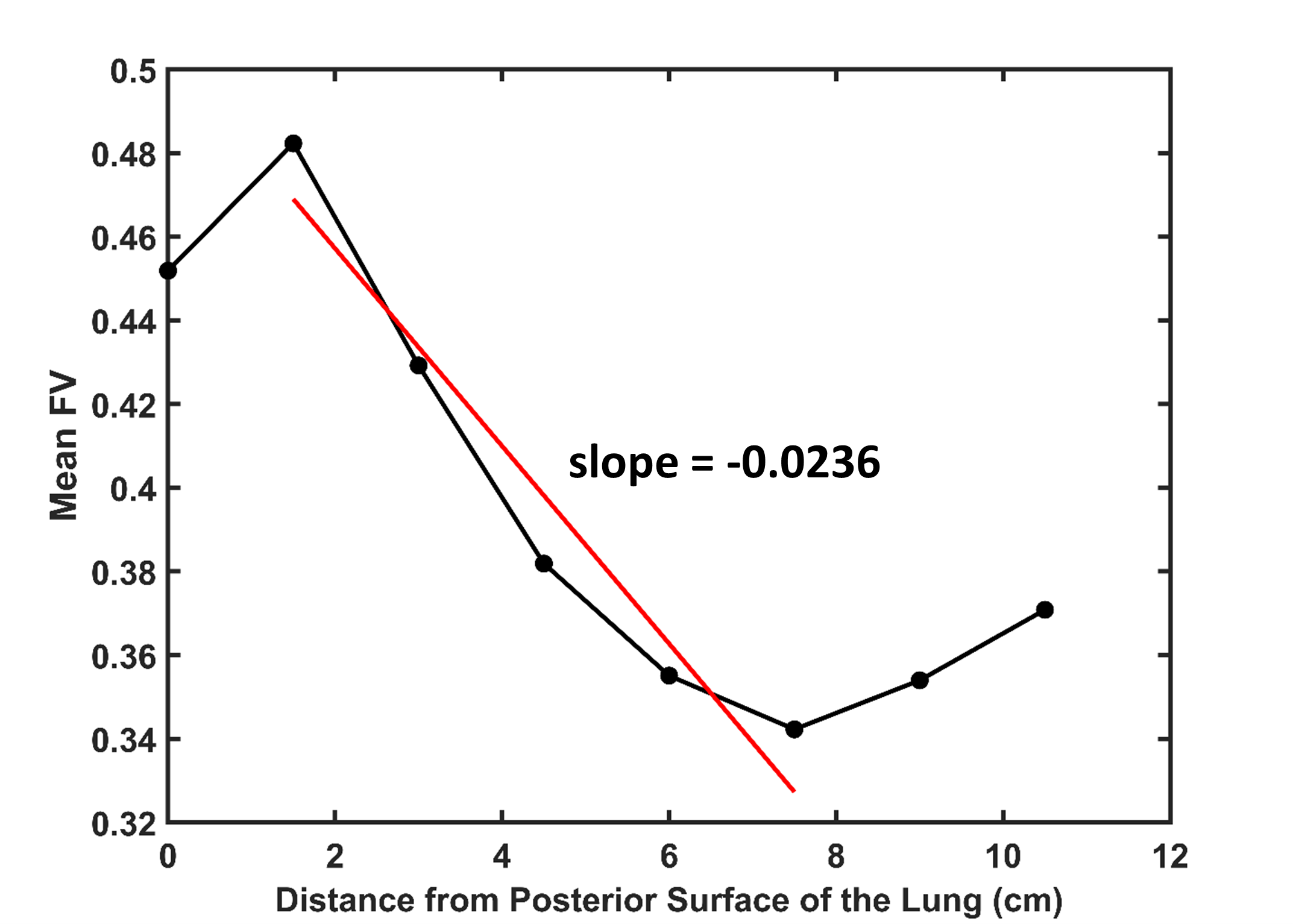
Figure 4: Representative fractional ventilation (FV) gradient calculated in the anterior/posterior (A/P) direction using PFP gas. The solid red line indicates the linear regression line for the data set and the slope indicates the ventilation gradient in the anterior-posterior direction. Very anterior/posterior data points were omitted from the fit.