5062
Utility of diffusion-weighted magnetic resonance imaging in predicting treatment response to radiotherapy in locally advanced cervical cancer1Department of Medical Imaging, Radiology Center, The University of Hong Kong-Shenzhen Hospital, Shenzhen, China, 2Department of Clinical Oncology, The University of Hong Kong-Shenzhen Hospital, Shenzhen, China
Synopsis
Keywords: DWI/DTI/DKI, Tumor, cervical cancer; radiotherapy;diffusion-weighted imaging;apparent diffusion coeffificient
Motivation: Radiotherapy (RT) is regarded as standard therapy for locally advanced cervical cancer. To date there are no accepted modalities that can reliably predict treatment response.
Goal(s): Present study aimed to explore the baseline and interim-ADC as well as change in ADC for predicting treatment outcomes.
Approach: 80 patients underwent pelvis MRI at least three times: before treatment, juring the course of RT and after completion of RT. Following values were calculated: Pre-ADC , Interim-ADC, △ADC and △%ADC. Treatment outcome was assessed by RECIST.
Results: Pre-treatment tumor size and interim-ADC could be potential biomarkers for predicting treatment outcomes in cervical cancer patients referred for RT.
Impact: The results of present study can evaluate the early efficacy of RT, in order to allow for the timely adjustment of treatment plans, improve the efficacy and prognosis, and provide a reference for the clinical individualized treatment of cervical cancer.
Introduction
Radiotherapy (RT) with or without concurrent chemotherapy is regarded as the standard therapy for locally advanced cervical cancer (International Federation of Gynecology and Obstetrics [FIGO] stage IB2 and above). However, predicting the treatment response of RT in patients with locally advanced cervical cancer is challenging. The present study aimed to explore the utility of baseline apparent diffusion coeffificient (ADC) and interim-ADC as well as change in ADC for predicting end-of-treatment outcomes in cervical cancer patients referred for RT.Methods
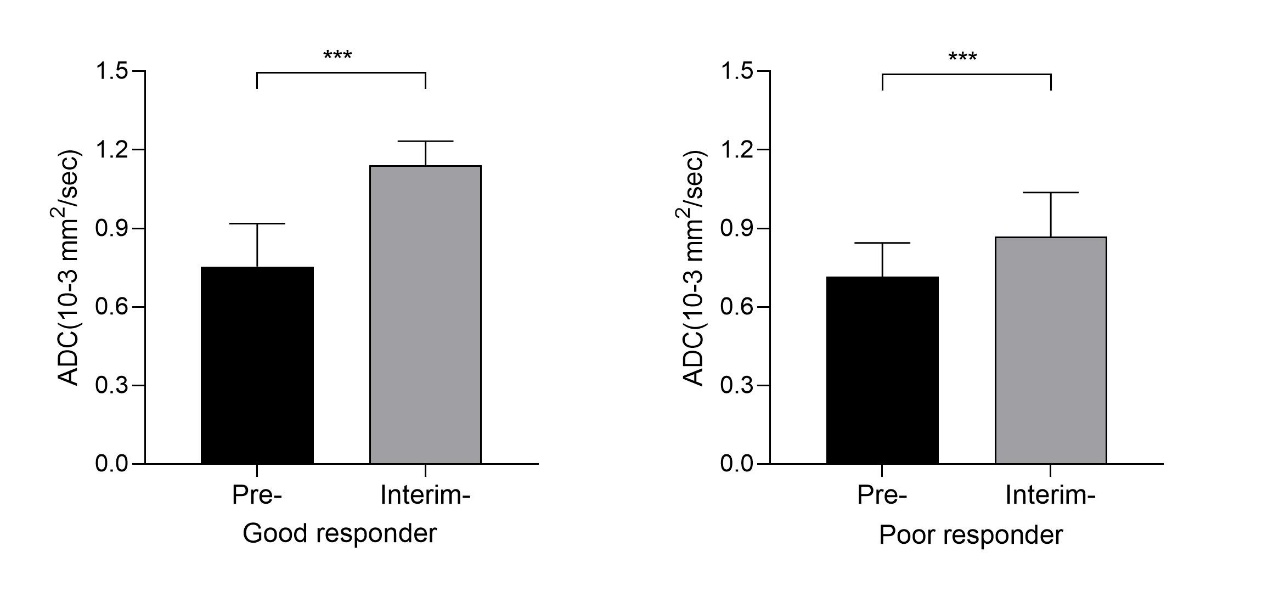
This retrospective study enrolled 80 stage IB2 to IVA cervical cancer patients. All patients had biopsy-proven squamous cell carcinoma (SCC) of the cervix and underwent RT or CCRT at the department of Clinical Oncology of the University of Hong Kong-Shenzhen hospital between November 2015 and July 2020. All of the 80 patients underwent abdomenal or pelvis MRI at least three times: before treatment, three weeks after beginning of RT and about 2 months after completion of RT. The following ADC values of the primary tumor were calculated: Pre-ADC = Mean ADC value recorded before RT; Interim-ADC = Mean ADC value recorded three weeks after beginning of RT;△ADC = Pre-ADC minus Interim-ADC;△%ADC = (△ADC/Pre-ADC)×100%. The statistical endpoint was treatment outcome assessed by end-of-treatment MR according to the Response Evaluation Criteria in Solid Tumors (RECIST). The patients were classified as good responders (complete response) and poor responders (stable disease, partial response, or progressive disease) based on the end-of-treatment MR.Results
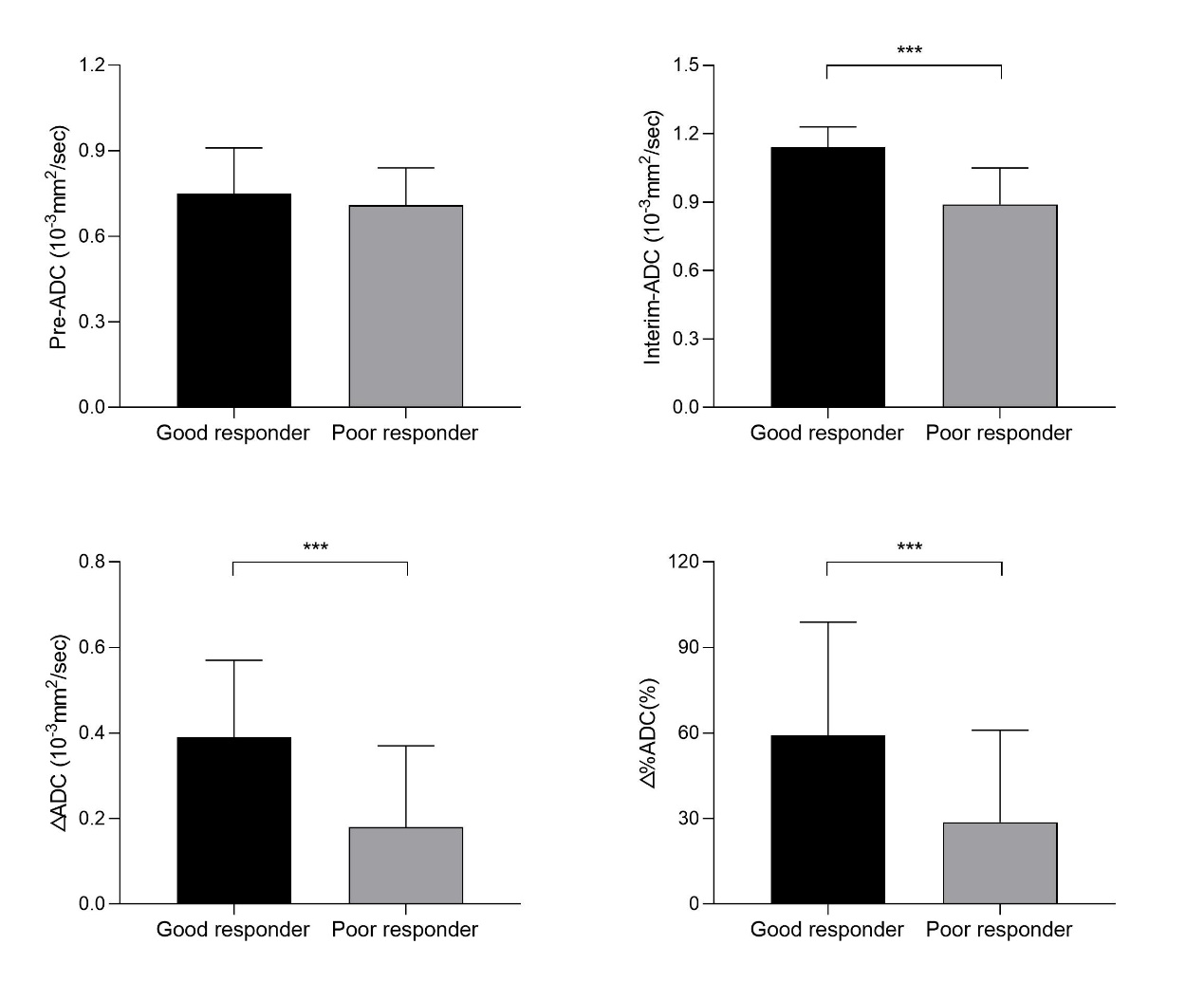
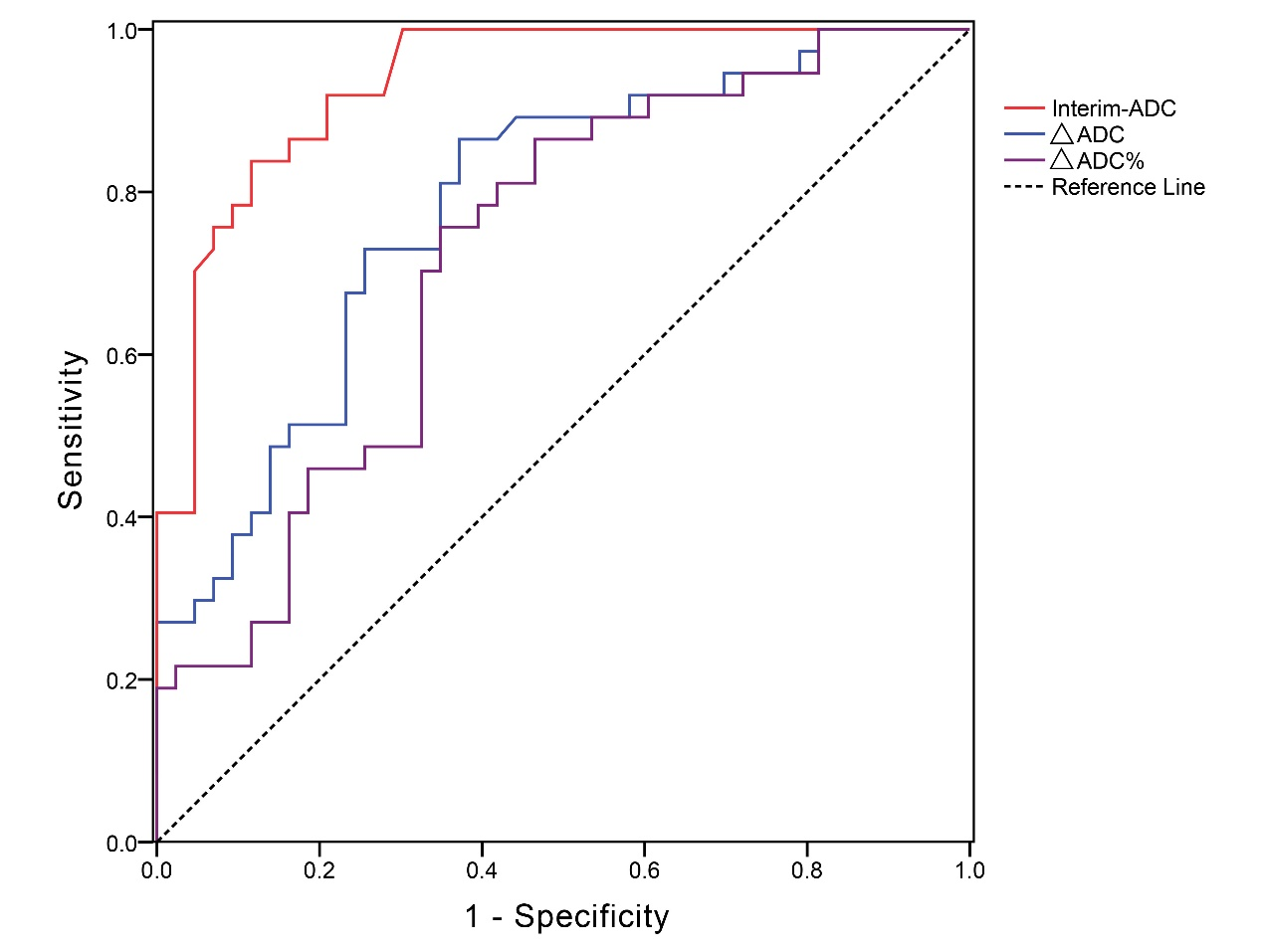
The values of the interim-ADC was signifificantly higher than the pre-ADC (1.01±0.18 VS 0.73±0.15, p < 0.001, Wilcoxon signed-rank test). There was not a statistically signifificant difffference of pre-ADC (p = .245) between of good-responder group (0.75 ± 0.16 × 10−3 mm2/s) and poor-responder group (0.71 ± 0.13 × 10−3 mm2/s). The mean interim-ADC was 1.14 ± 0.09 × 10−3 mm2/s in good-responder group and 0.89 ± 0.16 × 10−3 mm2/s in poor-responder group, with a statistical signifificant difffference (p < .001). ADC changes (△ADC and △%ADC), calculated about three weeks after beginning of RT as compared to baseline value, were significant lower in poor-responder group than in good-responder group (p ≤ .001). ROC curve analysis revealed that larger Interim-ADC and large changes in ADC values (△ADC and △%ADC) were strongly associated with a good response, with AUC values of 0.935, 0.783, and 0.723, respectively. The Interim-ADC, △ADC, and △%ADC performed well to differentiate poor responders from good responders, with sensitivities, specifificities, and accuracies above 75.68%, 62.79%, and 70.0%, respectively. Univariate analysis revealed younger age (<50 years old), smaller baseline-size, larger interim-ADC and large changes in ADC values (△ADC and △%ADC) were associated with a good response to treatment in univariate analysis (p<0.05). However, multivariate analysis revealed that treatment response was not correlated with age and changes in ADC values (△ADC and △%ADC) but just with the baseline-size and interim-ADC (p = 0.013, p < 0.001, respectively).Discussion
The pre-treatment tumor size and interim-ADC obtained during the mid-treatment periods could be potential biomarkers for predicting end-of-treatment outcomes in cervical cancer patients referred for RT.Conclusion
This is the first attempt to study the utility of baseline-ADC and interim-ADC as well as change in ADC for predicting end-of-treatment outcomes in cervical cancer patients referred for RT. The results can facilitate individualized tailoring of radiation treatment in cervical cancer patients.Acknowledgements
The authors would like to express their gratitude to Dr. Chaoxia Lv from Department of Obstetrics and Gynecology, the University of Hong Kong-Shenzhen Hospital, for the kind help provided.References
1 Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021;71:209–49.
2 Bhatla N, Aoki D, Sharma DN, et al. Cancer of the cervix uteri. Int J Gynaecol Obstet 2018;143 Suppl 2:22–36.
3 Kim YS, Shin SS, Nam JH, et al. Prospective randomized comparison of monthly flfluorouracil and cisplatin versus weekly cisplatin concurrent with pelvic radiotherapy and high-dose rate brachytherapy for locally advanced cervical cancer. Gynecol Oncol 2008;108:195-200.
4 Hamstra DA, Rehemtulla A, Ross BD. Diffusion magnetic resonance imaging: a biomarker for treatment response in oncology. J Clin Oncol 2007;25:4104–4109.
5 Thoeny HC, De Keyzer F, King AD. Diffusion-weighted MR imaging in the head and neck. Radiology 2012;263:19–32.
6 Padhani AR, Liu G, Mu-Koh D, et al. Diffusion-weighted magnetic resonance imaging as a cancer biomarker: consensus and recommendations. Neoplasia 2009;11:102–125.
7 Lai V, and Khong PL. Updates on MR imaging and 18F-FDG PET/CT imaging in nasopharyngeal carcinoma. Oral Oncol 2014;50:539–548.
8 Hou J, Yu X, Hu Y, et al. Value of intravoxel incoherent motion and dynamic contrast-enhanced MRI for predicting the early and short-term responses to chemoradiotherapy in nasopharyngeal carcinoma. Medicine 2016;95: e4320.
9 Pickles MD, Gibbs P, Lowry M, et al. Diffusion changes precede size reduction in neoadjuvant treatment of breast cancer. Magn Reson Imaging 2006;24:843–847.
10 Zhao M, Zhao L, Yang H, et al. Apparent diffusion coefficient for the prediction of tumor response to neoadjuvant chemo-radiotherapy in locally advanced rectal cancer. Radiat Oncol 2021;16:17.
11 Dashottar S, Pany TP, Lohia N. Role of apparent diffusion coefficient as a biomarker in the evaluation of cervical cancer. Indian J Radiol Imaging 2019;29:25–32.
12 Zheng X, Guo W, Dong J, et al. Prediction of early response to concurrent chemoradiotherapy in cervical cancer: Value of multi-parameter MRI combined with clinical prognostic factors. Magn Reson Imaging 2019;72:159–166.
13 Meyer HJ, Wienke A, Surov A. Pre-treatment apparent diffusion coefficient does not predict therapy response to radiochemotherapy in cervical cancer: a systematic review and meta-analysis. Anticancer Res 2021;41:1163–1170.
14 Litière S, Bogaerts J. Imaging endpoints for clinical trial use: a RECIST perspective. J Immunother Cancer 2022;10:e005092.
Figures