5057
Ultrashort Echo Time MRI for Pediatric Patients with Craniofacial Abnormalities1Department of Radiology, University of Pennsylvania, Philadelphia, PA, United States, 2Department of Bioengineering, University of Pennsylvania, Philadelphia, PA, United States, 3Division of Plastic, Reconstructive, and Oral Surgery, Children's Hospital of Philadelphia, Philadelphia, PA, United States, 4School of Electronics Engineering, Kyungpook National University, Daegu, Korea, Republic of, 5Department of Orthopaedic Surgery, University of Pennsylvania, Philadelphia, PA, United States
Synopsis
Keywords: MSK, Bone
Motivation: Ionizing radiation risk from CT remains a concern for pediatric patients with craniofacial abnormalities.
Goal(s): Use high-resolution bone-selective MRI for cranial bone imaging and evaluate feasibility in pediatric patients.
Approach: We quantitatively assessed a new echo-subtraction UTE sequence against clinical CT and another well-known MRI technique to assess their strengths and limitations.
Results: The proposed UTE sequence had high agreement with CT among the 3D rendered bone segmentations in terms of Dice similarity coefficient and quantification of clinical craniometric measurements. Furthermore, the bone-selective MR images clearly depict thin bone structures with attenuation of both soft-tissues and air.
Impact: Craniofacial imaging with the proposed ultrashort echo time sequence has high agreement with CT in pediatric patients. MRI can be a reliable non-ionizing and radiation-free modality for pediatric patients who are at increased risk of radiation malignancy.
Abstract
IntroductionCraniofacial anomalies are a variety of birth defects that affect the head, face, and neck.1,2 CT is the clinical standard for pre-operative and post-operative assessment of pediatric patients. However, children are at higher risk of ionizing radiation exposure due to the greater sensitivity of their developing organs to radiation.3-5 Therefore, there is an ongoing interest in using high-resolution MRI as a non-ionizing, radiation-free alternative to CT.6-10 The authors’ lab developed a dual-radiofrequency, dual-echo, three-dimensional ultrashort echo time (DURANDE) sequence, which exploits the sensitivity of bone proton magnetization to both T2 and RF pulse duration to further suppress soft-tissues and increase bone contrast.11 It has previously demonstrated enhanced bone signal and suppression of soft-tissues and air, and has been evaluated against CT both ex vivo and in vivo in healthy adults.12-14 In this study, we quantitatively evaluated DURANDE against clinical-standard CT in a small group of pediatric patients with craniofacial anomalies. Furthermore, we quantitatively assessed DURANDE’s performance against another common MRI craniofacial technique, zero-echo time (ZTE) MRI 8,15,16, to fully evaluate their strengths and limitations.
Methods
Pediatric patients indicated for clinical CT were recruited (n=6, 3 females, age range 8.8-16.4 yo). Patients had a variety of medical conditions, including craniosynostosis, jaw asymmetry, and subgaleal fluid. Patients were imaged at 3.0 T (Prisma, Siemens, Erlangen, Germany) with a 20-channel head/neck coil using two skull-imaging sequences. DURANDE11 (Fig.1) is a custom sequence that exploits the sensitivity of the signal to both RF pulse duration and echo time11,17 with TR/TE1/TE2 = 7/0.06/2.36 ms, RF1/RF2 = 0.04/0.52 ms, flip angle = 12º, FOV = 280x280x280 mm, matrix size = 256x256x256, and scan time = 6 minutes. ZTE-PETRA15,18 is a Siemens Work in Progress sequence with TR/TE = 2.85/0.07 ms, flip angle = 2º, FOV = 280x280x280 mm, matrix size = 256x256x256, and scan time = 5 minutes. For DURANDE, bone-specific images are generated by echo subtraction of the short- and long T2 images [Imagebone = (Imageecho1 – Imageecho2)/(Imageecho1 + Imageecho2)].11 For ZTE-PETRA, bias-field correction was applied using the nonparametric N4ITK method19 and bright-bone images were derived via logarithmic inversion.9,15,16 Images were semi-automatically segmented, and using the 3D renderings of the skull binary masks, a total of six craniometric measurements were manually derived: cranial height, cranial width, cranial length, interzygomatic distance, left and right orbit heights. Lin’s concordance correlation coefficient (CCC) and Bland-Altman plots were utilized to assess the agreement in craniometrics between MRI and CT. Furthermore, CT and ZTE-PETRA were registered to DURANDE, and the segmented skulls were then manually cropped to include only the cranial vault, orbits, and upper part of the maxilla. The similarity of the segmented skulls among the scans were quantified using the dice similarity coefficient (DSC).
Results
Example bone slices for two pediatric patients comparing DURANDE and ZTE-PETRA to clinical CT are shown in Fig.2, along with skull 3D renderings in Fig.3. DSC per patient is illustrated in Fig.4A, with an overall average ± standard deviation of 0.75±0.18, 0.70±0.19, and 0.77±0.15 for DURANDE versus CT, ZTE-PETRA versus CT, and DURANDE vs ZTE-PETRA, respectively (Fig.4B). The bias in craniometric measurements among scan pairs are shown in Fig.4C. Table 1 lists the average percent difference in craniometrics and agreement based on Lin’s (CCC).
Discussion
Two MRI sequences were validated against clinical CT in pediatric patients with craniofacial abnormalities by assessing the similarities among their skull segmentations and craniometric measurements. Based on DSC, there is overall good skull overlap between MRI and CT, however, it decreases near the orbits and nasal concha where there are thinner bone structures and more bone-air interfaces. Additionally, compared to adults, children have thinner bones and are generally less compliant, the latter resulted in motion artifacts in a few patients during both DURANDE and ZTE-PETRA.
Compared to ZTE-PETRA, DURANDE had greater bone-contrast in the facial regions and higher segmentation overlap with CT based on the DSC. Thus, DURANDE had higher Lin’s CCC on average with CT for the interzygomatic distance and left/right orbit heights. Moreover, DURANDE had smaller absolute percent differences in craniometrics when compared to CT (<2 mm), while ZTE-PETRA had greater differences (<5mm).
Conclusion
There was good agreement between CT and DURANDE in pediatric patients, demonstrating the clinical feasibility of the technique. DURANDE is a UTE-subtraction technique that is self-normalized (i.e., no need for bias correction) and is designed to yield bone-selective images with soft-tissue and air attenuated. ZTE-PETRA had insufficient facial-bone contrast, however; its low level of acoustic noise as the gradients are not ramped down between views may be advantageous for pediatric patients’ comfort.
Acknowledgements
NIH T32 EB020087; NIH T32-AR007132; NIH R21 DE028417References
1. Kajdic N, Spazzapan P, Velnar T. Craniosynostosis - Recognition, clinical characteristics, and treatment. Bosn J Basic Med Sci 2018;18(2):110-116. (In eng). DOI: 10.17305/bjbms.2017.2083.
2. Johnson D, Wilkie AO. Craniosynostosis. Eur J Hum Genet 2011;19(4):369-76. (In eng). DOI: 10.1038/ejhg.2010.235.
3. Miglioretti DL, Johnson E, Williams A, et al. The use of computed tomography in pediatrics and the associated radiation exposure and estimated cancer risk. JAMA Pediatr 2013;167(8):700-7. (In eng). DOI: 10.1001/jamapediatrics.2013.311.
4. Pearce MS, Salotti JA, Little MP, et al. Radiation exposure from CT scans in childhood and subsequent risk of leukaemia and brain tumours: a retrospective cohort study. Lancet 2012;380(9840):499-505. (In eng). DOI: 10.1016/s0140-6736(12)60815-0.
5. Mathews JD, Forsythe AV, Brady Z, et al. Cancer risk in 680,000 people exposed to computed tomography scans in childhood or adolescence: data linkage study of 11 million Australians. BMJ (Clinical research ed) 2013;346:f2360. (In eng). DOI: 10.1136/bmj.f2360.
6. Eley KA, McIntyre AG, Watt-Smith SR, Golding SJ. "Black bone" MRI: a partial flip angle technique for radiation reduction in craniofacial imaging. The British journal of radiology 2012;85(1011):272-278. (In eng). DOI: 10.1259/bjr/95110289.
7. Eley KA, Watt-Smith SR, Golding SJ. "Black bone" MRI: a potential alternative to CT when imaging the head and neck: report of eight clinical cases and review of the Oxford experience. The British journal of radiology 2012;85(1019):1457-64. (In eng). DOI: 10.1259/bjr/16830245.
8. Wiesinger F, Ho ML. Zero-TE MRI: principles and applications in the head and neck. The British journal of radiology 2022;95(1136):20220059. (In eng). DOI: 10.1259/bjr.20220059.
9. Lu A, Gorny KR, Ho ML. Zero TE MRI for Craniofacial Bone Imaging. AJNR Am J Neuroradiol 2019;40(9):1562-1566. (In eng). DOI: 10.3174/ajnr.A6175.
10. Saarikko A, Mellanen E, Kuusela L, et al. Comparison of Black Bone MRI and 3D-CT in the preoperative evaluation of patients with craniosynostosis. J Plast Reconstr Aesthet Surg 2020;73(4):723-731. (In eng). DOI: 10.1016/j.bjps.2019.11.006.
11. Lee H, Zhao X, Song HK, Zhang R, Bartlett SP, Wehrli FW. Rapid dual-RF, dual-echo, 3D ultrashort echo time craniofacial imaging: A feasibility study. Magnetic resonance in medicine 2019;81(5):3007-3016. (In eng). DOI: 10.1002/mrm.27625.
12. Zhang R, Lee H, Zhao X, et al. Bone-Selective MRI as a Nonradiative Alternative to CT for Craniofacial Imaging. Academic Radiology 2020;27(11):1515-1522. DOI: https://doi.org/10.1016/j.acra.2020.03.001.
13. Zimmerman CE, Khandelwal P, Xie L, et al. Automatic Segmentation of Bone Selective MR Images for Visualization and Craniometry of the Cranial Vault. Acad Radiol 2021 (In eng). DOI: 10.1016/j.acra.2021.03.010.
14. Kamona N, Jones BC, Lee H, et al. Cranial bone imaging using ultrashort echo-time bone-selective MRI as an alternative to gradient-echo based “black-bone” techniques. Magnetic Resonance Materials in Physics, Biology and Medicine 2023((in press)). DOI: 10.1007/s10334-023-01125-8.
15. Wiesinger F, Sacolick LI, Menini A, et al. Zero TE MR bone imaging in the head. Magnetic resonance in medicine 2016;75(1):107-14. (In eng). DOI: 10.1002/mrm.25545.
16. Delso G, Wiesinger F, Sacolick LI, et al. Clinical evaluation of zero-echo-time MR imaging for the segmentation of the skull. J Nucl Med 2015;56(3):417-22. (In eng). DOI: 10.2967/jnumed.114.149997.
17. Johnson EM, Vyas U, Ghanouni P, Pauly KB, Pauly JM. Improved cortical bone specificity in UTE MR Imaging. 2017;77(2):684-695. DOI: https://doi.org/10.1002/mrm.26160.
18. Li C, Magland JF, Seifert AC, Wehrli FW. Correction of excitation profile in Zero Echo Time (ZTE) imaging using quadratic phase-modulated RF pulse excitation and iterative reconstruction. IEEE transactions on medical imaging 2014;33(4):961-9. (In eng). DOI: 10.1109/tmi.2014.2300500.
19. Tustison NJ, Avants BB, Cook PA, et al. N4ITK: Improved N3 bias correction. IEEE transactions on medical imaging 2010;29(6):1310-1320. (Article). DOI: 10.1109/TMI.2010.2046908.
Figures
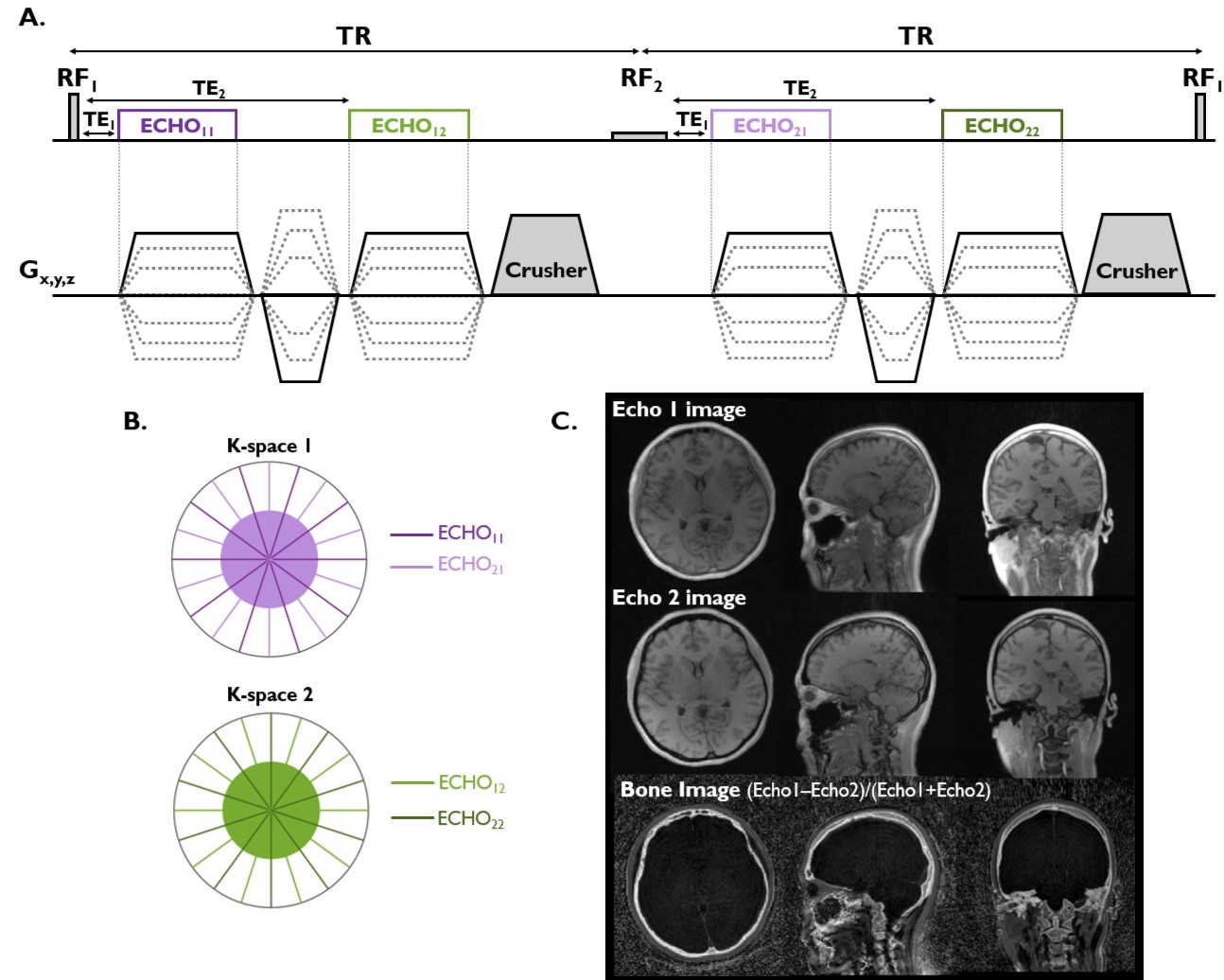
Figure 1: Overview of the DURANDE sequence. A) Pulse sequence diagram with short and long RF pulses applied along two successive TRs to produce four datasets. B) Construction of two independent k-space datasets, where echo11/echo21 make k-space set 1, and echo12/echo22 make k-space set 2. C) Echo1 image captures the signal from both short and long T2 species, while echo2 image contains only the signal from long T2 species. The final bone image is the subtraction image depicting bone signal only.
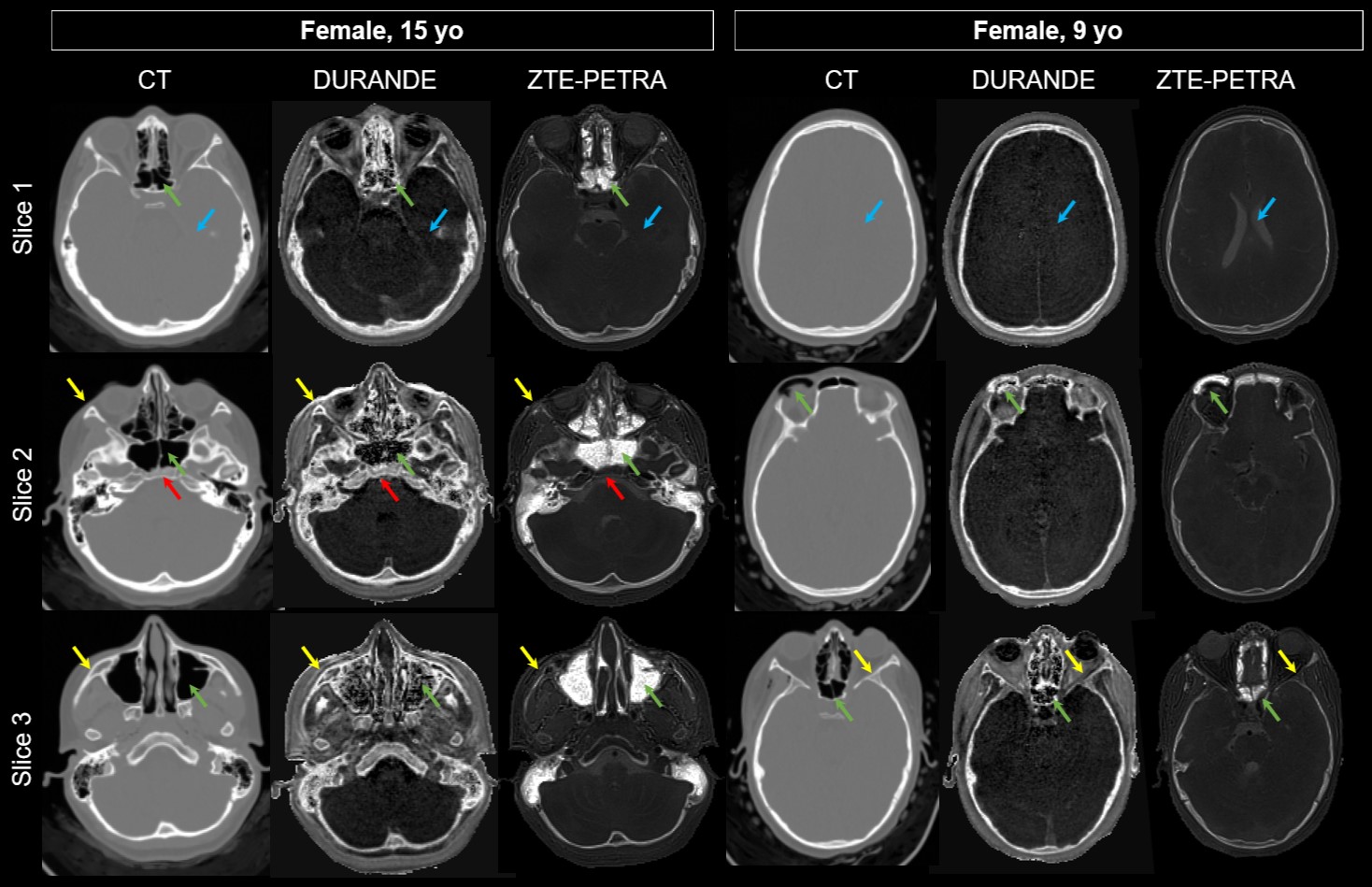
Figure 2: Clinical CT images compared against the bright-bone images from two MRI sequences for two pediatric patients. Air appears with background intensity in DURANDE and white in ZTE-PETRA (green arrows). DURANDE clearly resolves thin facial bone structures, unlike ZTE-PETRA (yellow arrows). Soft-tissue suppression is superior in DURANDE (blue arrows), while ZTE-PETRA has full bone-marrow attenuation compared to the partial attenuation in DURANDE (red arrows).
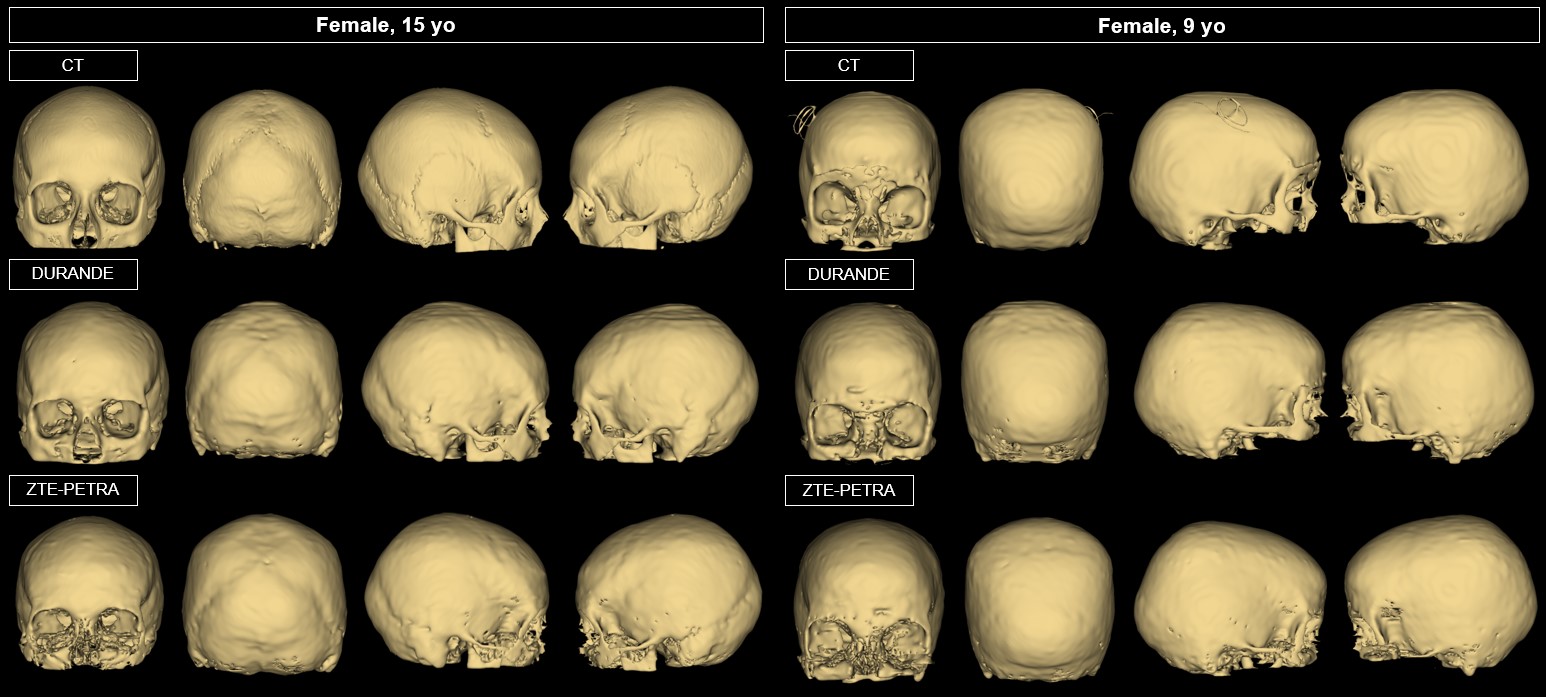
Figure 3: Skull 3D renderings of the two pediatric patients in Figure 2, comparing CT, DURANDE and ZTE-PETRA. Note the poor contrast in the facial regions in ZTE-PETRA when compared to CT and DURANDE (red arrows). There is slight motion blur in DURANDE (blue arrow).
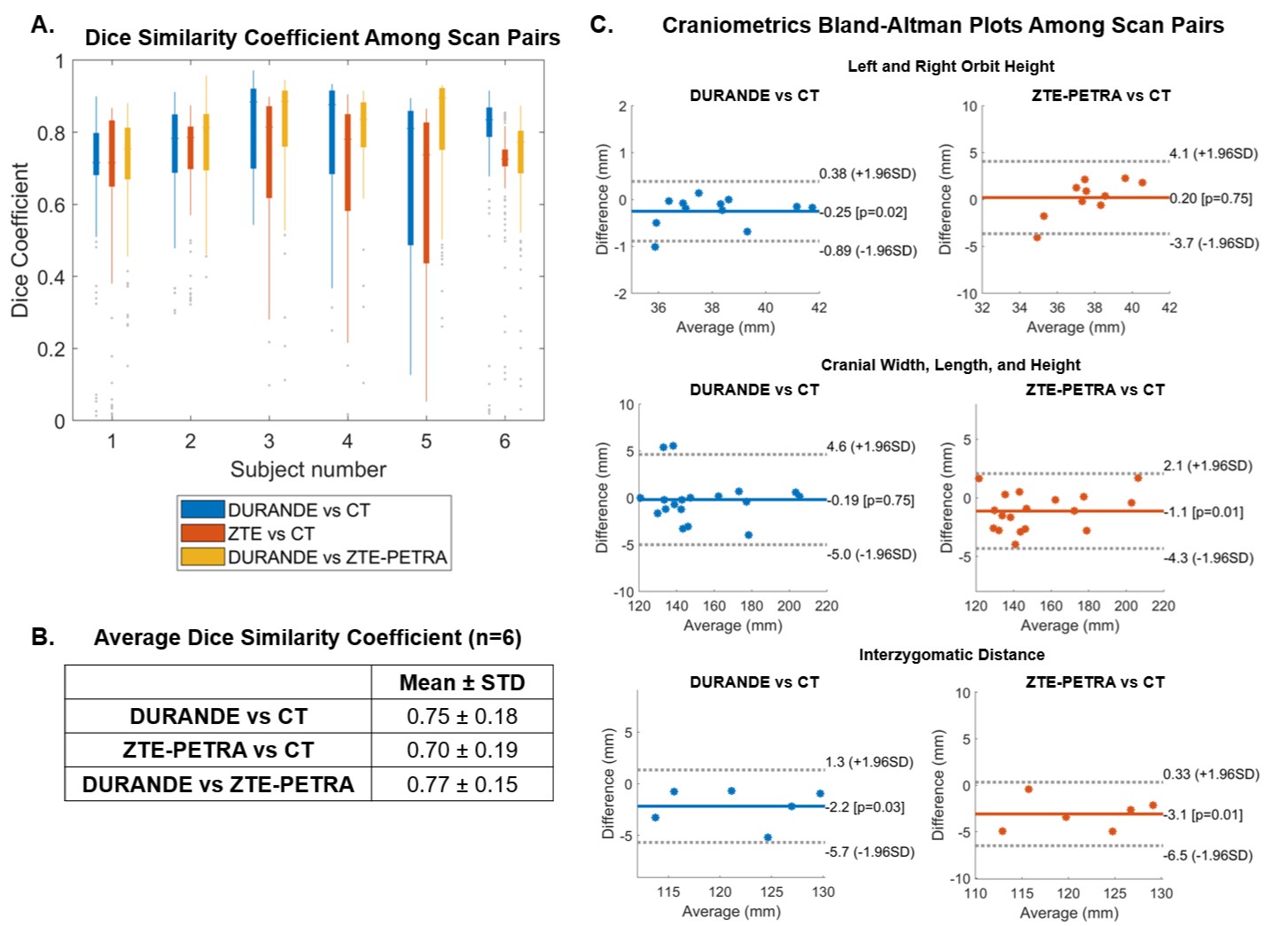
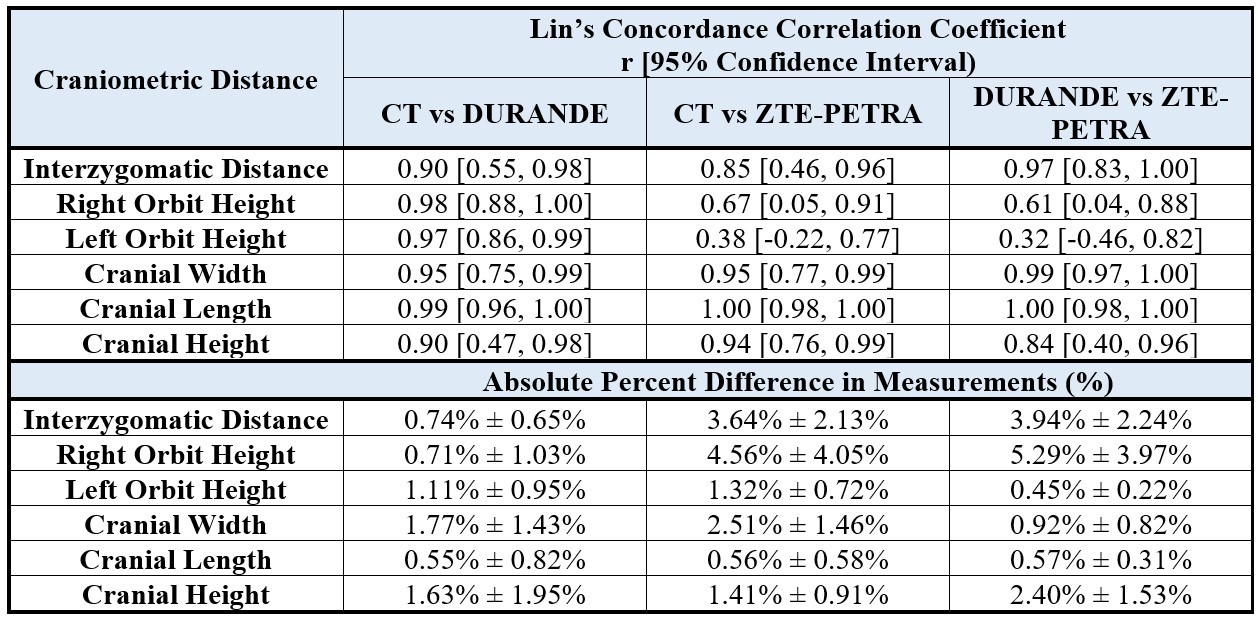
Table 1: Agreement in craniometric measurements based on Lin’s concordance correlation coefficient, and the absolute percent difference in measurements among scan pairs (n=6).