5054
Ultrashort Echo Time and Fast Field Echo Imaging and Processing for Spine Bone Imaging in Spondylolysis1University of California, San Diego, La Jolla, CA, United States, 2Canon Medical Systems Corporation, Tochigi, Japan, 3Family Medicine, Unviersity of California, San Diego, La Jolla, CA, United States, 4VA San Diego Healthcare System, San Diego, CA, United States
Synopsis
Keywords: MSK, Adolescents, Pars Interarticularis, UTE, FE, Image Processing
Motivation: Fracture of pars interarticularis is a common injury in adolescent athletes, currently requiring CT scan for accurate diagnosis.
Goal(s): Advance MR imaging to depict spinal bone with high fidelity.
Approach: Two techniques utilizing multiecho ultrashort echo time (UTE) and field echo (FE) with simple post-processing were developed to image lumbar spinal bone. SNR and CNR were determined, and clinical utility was assessed in patients.
Results: Improvements in visual quality and bone contrast were achieved using multiecho processing as opposed to a single echo inversion. Both UTE and FE techniques provided good bone contrast, although FE provide significantly better resolution and bone-muscle contrast.
Impact: This study advances MR imaging of the pars interarticularis for evaluation of spondylolysis. We demonstrated clinical feasibility in a patient with a pars defect, depicted with clarity with the techniques described here.
INTRODUCTION
Isthmic spondylolysis,1 characterized by stress injury to the pars interarticularis of the lumbar spine,2, 3 is found in half of adolescent athletes with persistent low back pain.2, 4-9 For clinical evaluation computed tomography (CT) is the gold standard, but a suitable MRI technique could reduce unnecessary radiation exposure. Bone imaging with MRI has been available using ultrashort echo time (UTE),10 and zero echo time (ZTE)11 MRI. While promising, limitations of these techniques include low signal to noise ratio and resolution. We describe and compare two techniques using multiecho UTE and field echo (FE) acquisition followed by simple post-processing that yields CT-like contrast.METHODS
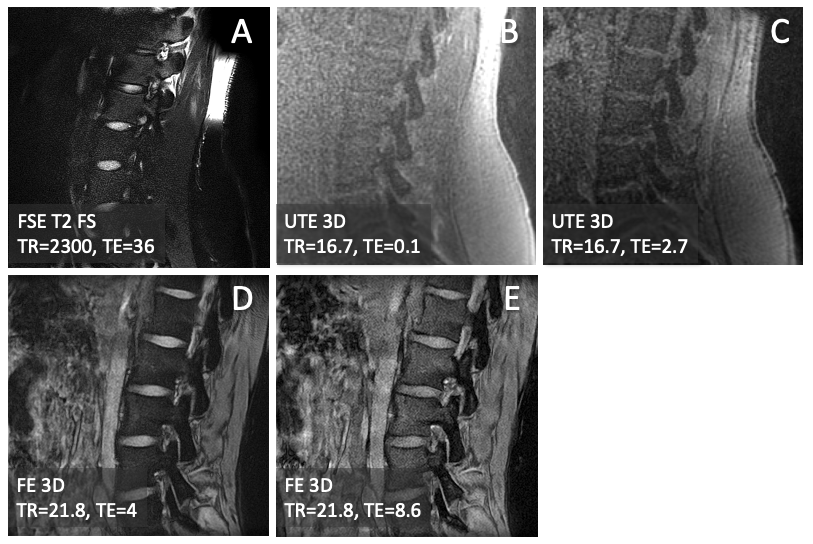
Subjects: Lumbar spines of four subjects (n=4, 3 females, 19.5 ± 5.5 years old) were imaged at 3-T (Canon Galan) with a posterior spine coil. Two of the subjects were adolescent (16 yo female, 14 yo male) athletes with low back pain for past 4-8 weeks.MRI: One anatomical sequence and two bone-oriented sequences were used: (1) sagittal fast spin echo T2 (FSE T2) weighted with fat suppression: TR=5600 ms, TE=80 ms, FOV=220 mm, matrix=320x416, slice=3 mm, ETL=19; (2) axial 3D UTE multi-echo: TR=16.7 ms, TE=0.1, 2.7, 5.3 ms, FOV=300 ms, matrix=320x320, slice=1 mm, reformatted to sagittal plane. (3) sagittal 3D field echo (FE) multi-echo: TR=34.4 ms, TE=4, 8.6, 13.2 ms, FOV=170 mm, matrix=320x240, slice=1 mm. The raw images are shown in Figure 1.
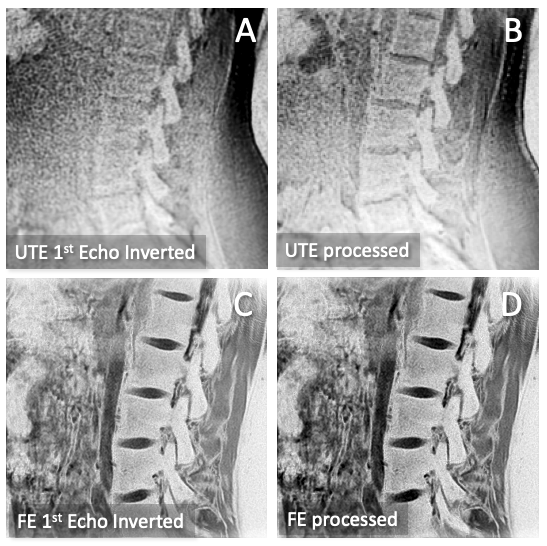
CT-like Image Processing (Figure 2): 1st echo images from UTE (Figure 1B) and FE (Figure 2D) were inverted to create a CT-like contrast (Figure 2AC). Additionally, to create multiecho-processed images for UTE (Figure 2B) and FE (Figure 2D), the images from different TEs were first averaged then inverted to create the CT-like contrast.
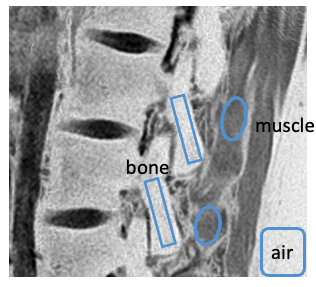
SNR, CNR: Regions of interest (ROI) were drawn on selected slices of the CT-like images. ROIs were placed on the pars, muscle, and air (Figure 3) to determine SNR and CNR values. Effects of sequence (UTE, FE) and processing (1st echo vs. multiecho) were determined using two-way ANOVA.
Spondylolysis: On the subjects with low back pain, conventional, processed UTE, and processed FE images were evaluated to detect the presence of pars defect (Figure 4).
RESULTS
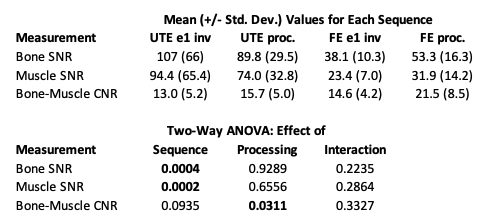
CT-Like Images: Compared to FSE T2 (Figure 1A), 1st echo inverted (Figure 2AC) and multiecho processed (Figure 2BD) UTE and FE images all depicted spinal bone distinctly with high signal intensity, similar to CT. UTE (Figure 2AB) and FE (Figure 2CB) images, while both providing CT-like contrast, had clear differences; UTE was softer while providing a flatter contrast between bone vs. other tissues. FE images were sharper, depicted bone with high contrast, but also depicted non-bone tissues (e.g., fascia of muscle) with high signal intensity. When comparing 1st echo inverted (Figure 2AC) vs. processed (Figure 2BD) images, the processed images were less noisy and had better contrast for bone.SNR, CNR: Table 1 summarizes SNR and CNR values for the CT-like images. CT-like images from UTE data had mean SNR values of 90 to 100, which was significantly higher (p=0.0002) than the value from FE data (mean SNR 38 to 53). However, the CNR (bone-muscle) values were slightly higher (p=0.09) for FE (15 to 22) compared to UTE (13 to 16). Multiecho processing, for both UTE and FE data, improved the CNR values significantly (p=0.03): For UTE, CNR on average improved by 2.7, while for FE, CNR improved by 6.9. This corroborates visual improvements in contrast apparent in the image comparison in Figure 2.
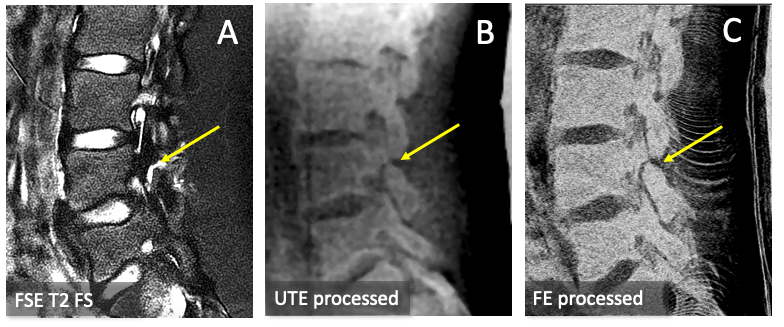
Spondylolysis: In a low back pain subject, we detected a progressive spondylolysis with a moderate-sized bone defect seen as a gap with high signal intensity in FSE T2 (Figure 4A), and a clear non-union in the UTE processed (Figure 4B) and FE processed (Figure 4C) images.
CONCLUSION
We demonstrated the feasibility of spine bone MRI that provides CT-like contrast using existing multiecho sequences and simple image processing. Improvements in visual quality and bone contrast were achieved using multiecho processing as opposed to a single echo inversion. Both UTE and FE techniques provided useable bone contrast, although FE provide significantly better resolution and bone-muscle contrast, which will be invaluable for detecting finer fractures. Clinical applicability was also demonstrated in a patient where a progressive spondylolysis was detected. Our FE technique is similar to fast field echo resembling a CT using restricted echo-spacing,12 but uses different post-processing. While there still is no MRI technique that provides a perfect CT-like contrast, continued advancement of different MRI techniques will provide benefit for specific use cases such as spondylolysis.Acknowledgements
Research reported in this publication was supported in part by a research grant from National Institute of Health (R01 AR066622 and P30 AR073761) in support of Dr. Bae, and a research grant support from Canon Medical Systems Corp., Japan (35938) in support of Dr. Miyazaki. The content is solely the responsibility of the authors and does not necessarily represent the official views of the sponsoring institutions.
References
1. Wiltse LL, Newman PH, Macnab I. Classification of spondylolisis and spondylolisthesis. Clin Orthop Relat Res: 23-29, 1976.
2. Fredrickson BE, Baker D, McHolick WJ, Yuan HA, Lubicky JP. The natural history of spondylolysis and spondylolisthesis. J Bone Joint Surg Am 66: 699-707, 1984.
3. Bechtel W, Griffiths H, Eisenstadt R. The Pathogenesis of Spondylolysis. Investigative radiology 17: S29, 1982.
4. Micheli LJ, Wood R. Back pain in young athletes. Significant differences from adults in causes and patterns. Arch Pediatr Adolesc Med 149: 15-18, 1995.
5. Olsen TL, Anderson RL, Dearwater SR, Kriska AM, Cauley JA, Aaron DJ, LaPorte RE. The epidemiology of low back pain in an adolescent population. Am J Public Health 82: 606-608, 1992. PMCID:PMC1694113.
6. Selhorst M, MacDonald J, Martin LC, Rodenberg R, Krishnamurthy R, Ravindran R, Fischer A. Immediate functional progression program in adolescent athletes with a spondylolysis. Phys Ther Sport 52: 140-146, 2021.
7. Soler T, Calderon C. The prevalence of spondylolysis in the Spanish elite athlete. Am J Sports Med 28: 57-62, 2000.
8. Reitman CA, Gertzbein SD, Francis WR, Jr. Lumbar isthmic defects in teenagers resulting from stress fractures. Spine J 2: 303-306, 2002.
9. Deyo RA, Weinstein JN. Low back pain. N Engl J Med 344: 363-370, 2001.
10. Bae WC, Biswas R, Chen K, Chang EY, Chung CB. UTE MRI of the Osteochondral Junction. Curr Radiol Rep 2: 35, 2014. PMCID:4104718
11. Bharadwaj UU, Coy A, Motamedi D, Sun D, Joseph GB, Krug R, Link TM. CT-like MRI: a qualitative assessment of ZTE sequences for knee osseous abnormalities. Skeletal Radiol 51: 1585-1594, 2022. PMCID:PMC9198000
12. Johnson B, Alizai H, Dempsey M. Fast field echo resembling a CT using restricted echo-spacing (FRACTURE): a novel MRI technique with superior bone contrast. Skeletal Radiol 50: 1705-1713, 2021.
Figures