5049
3D high-resolution isotropic multi-contrast knee MRI using 3D mDixon TSE with deep learning constrained Compressed SENSE
Yasuyuki Morita1, Michinobu Nagao1, Masami Yoneyama2, Mana Kato1, Takumi Ogawa1, Kazuo Kodaira1, Yutaka Hamatani1, Isao Shiina1, Yasuhiro Goto1, and Shuji Sakai1
1Tokyo Women's Medical University Hospital, Tokyo, Japan, 2Philips Japan, Tokyo, Japan
1Tokyo Women's Medical University Hospital, Tokyo, Japan, 2Philips Japan, Tokyo, Japan
Synopsis
Keywords: Cartilage, Artifacts
Motivation: Knee joint MRI requires m sequences involving multiple planes and with- and without fat suppression, which is time-consuming.
Goal(s): Provides detailed cartilage and ligament information in a short period of time and allows multiplanar reconstruction in any plane of any thickness from a single high-resolution isotropic imaging.
Approach: CS-AI 3D mDixon TSE images were compared with conventional SENSE and CS images.
Results: It indicated that 3D mDixon CS-AI can provide more accurate image information of cartilage and ligaments with high reproducibility and robustness.
Impact: This technique may be helpful to further assess knee pathology.
Introduction
Knee MRI is the most important method for evaluating cartilage and ligaments.1 Knee joint MRI requires m sequences involving multiple planes and with- and without fat suppression,2 which is time-consuming. Dixon technique provides separated fat and water images as an alternative to fat suppression. 3 Therefore, by using mDixon images might be used as a substitute for PDWI and FS PDWI images simultaneously. On the other hand, 3D knee MRI is recently widely used4-7. To accurately assess the small anatomies such as cartilage and ligaments, higher spatial resolution of 0.5 mm with isotropic is clinically desioable8. However, 3D mDixon TSE require two shifted echo datasets, it was quite challenging to apply 3D mDixon TSE in routine clinical examinations. Recently, integrating artificial intelligence (AI) into the Compressed SENSE reconstruction (CS-AI), based on Adaptive-CS-Net, has been introduced. We hypothesize that the CS-AI reconstruction can accelerate the 3D-Dixon TSE acquisition while maintaining clinically acceptable SNR. In this study, we attempted to utilize the CS-AI framework for 3D mDixon TSE. The purpose of this study was to demonstrate the feasibility of 3D mDixon TSE with CS-AI in knee joint imaging with healthy volunteers compared to conventional acceleration techniques.Methods
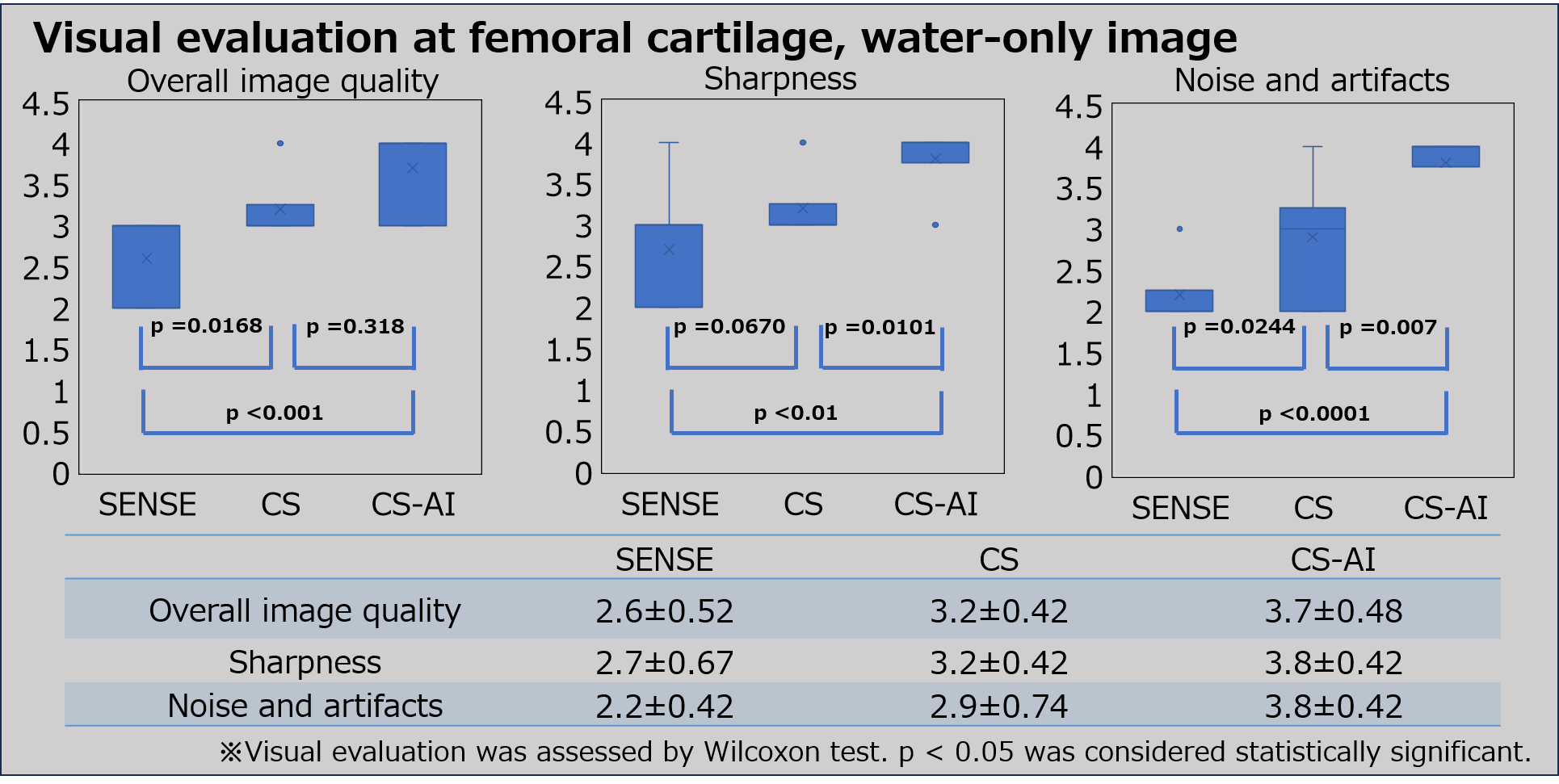
A total of 5 healthy volunteer were examined on a 3.0T whole-body clinical system (Ingenia Elition X, Philips Healthcare). The study was approved by the local IRB, and written informed consent was obtained from all subjects. 3D mDixon TSE with CS-AI is based on turbo spin-echo two-point Dixon algorithm with separated acquisition (Figure 1). CS-AI 3D mDixon TSE images were compared with conventional SENSE and CS images. Image quality was evaluated by visual score at the 2-points (femoral cartilage: water-only image, ligament: in-phase image) . For overall image quality, sharpness and noise and artifacts, we evaluated them as 4-point grades (grade “4” was excellent, “1” was severe) by two blinded readers. Visual evaluation was assessed by Wilcoxon test. For quantitative comparison, signal-to-noise ratio (SNR) and contrast-to-noise ratio (CNR) were measured. The SNR was assessed in the cartilage and ligaments. To allow quantitative SNR measurements, we used a noise-measurement-method proposed by Zwanenburg et al9. The standard-deviation of a region of interest of the corresponding area in the noise image was used as metric for the noise. SNRcartilage and SNRligaments were then calculated as follows: SNRA = SI(A) / SDnoise(A). Where SI are the mean average signal intensity of the cartilage and ligaments respectively, and the corresponding SDnoise is the standard-deviation at the same location on the noise images. Subsequently, we measured the CNR for comparing image contrast quantitatively. The CNR was estimated for cartilage and synovial fluid (CNRcartilage-synovial fluid). The CNRcartilage -synovial fluid was calculated by the following equations: CNRA-B = [SI(A) - SI(B)] / 0.5 [SDnoise(A) + SDnoise(B)] The SNR and CNR were assessed by one-way repeated measures analysis of variance (ANOVA) and the post-hoc Tukey-Kramer test. Imaging parameters for 3D mDixon TSE are as follows: voxel size = 0.6*0.6*0.6mm, FOV = 160*160*160mm, 533slices, TR = 1000ms, TE = 44ms, SENSE/C-SENSE acceleration factor = 8.0, total imaging time = 5 min 34 sec (SENSE, CS/CS-AI)Results and Discussion
Fig.2 shows representative images of healthy volunteer CS-AI-water-only-images. CS reduced the noise in the center of the SENSE-water-only- images, and CS-AI even further cleaned up the noise compared to CS. Fig.3 CS-AI also showed high cartilage sharpness. Fig. 4 shows representative images of healthy volunteer CS-AI-in-phase-images. ACL in CS-AI images were more conspicuous compared with SENSE and CS. It indicated that CS-AI can provide more accurate image information of cartilage and ligaments with high reproducibility and robustness. Although further clinical investigation is needed, CS-AI might be clinically useful in assessment of knee in more detail.Conclusion
3D mDixon TSE with CS-AI enables high-resolution (0.6mm) isotropic knee imaging with simultaneous PDW and fat-suppressed PDW contrasts without misalignments within a clinically feasible acquisition time around 5 minutes 30 seconds. This technique may be helpful to further assess knee pathology.Acknowledgements
No acknowledgements found.References
1.Link TM, Stahl R, Woertler K : Cartilage imaging, motivation, techniques, current and future significance, Eur Radiol., 17(5), 1135-1146, 2007. 2 .Kijowski R, Gold GE : Routine 3D magnetic resonance imaging of joints, J Magn Reson Imaging., 33(4), 758- 771, 2011. 3.Berglund J, Johansson L, Ahlstrom H, Kullberg ¨ J. Three-point Dixon method enables wholebody water and fat imaging of obese subjects. Magn Reson Med 2010; 63: 1659–68. doi: http://dx.doi.org/10.1002/mrm.22385 4.Shakoor D, Guermazi A, Kijowski R, et al. Diagnostic performance of three-dimensional MRI for depicting cartilage defects in the knee: a meta-analysis. Radiology 2018;289(01):71–82 5. Shakoor D, Kijowski R, Guermazi A, et al. Diagnosis of knee meniscal injuries by using three-dimensional MRI: a systematic review and meta-analysis of diagnostic performance. Radiology 2019;290(02):435–445 6.Altahawi F, Subhas N. 3D MRI in musculoskeletal imaging: current and future applications. Curr Radiol Rep 2018;6(08):27 7. Kijowski R, Davis KW, Woods MA, et al. Knee joint: comprehensive assessment with 3D isotropic resolution fast spin-echo MR imaging—diagnostic performance compared with that of conventional MR imaging at 3.0 T. Radiology 2009;2 8.Friedrich KM, Reiter G, Kaiser B, et al. : High-resolution cartilage imaging of the knee at 3T, basic evaluation of modern isotropic 3D MR-sequences, Eur J Radiol., 78(3),398-405, 2011. 9.Zwanenburg et al. MR Angiography of the cerebral perforating arteries with magnetization prepared anatomical reference at 7T: comparison with time-of-flight. J Magn Reson Imaging. 2008; 28: 1519–1526.Figures
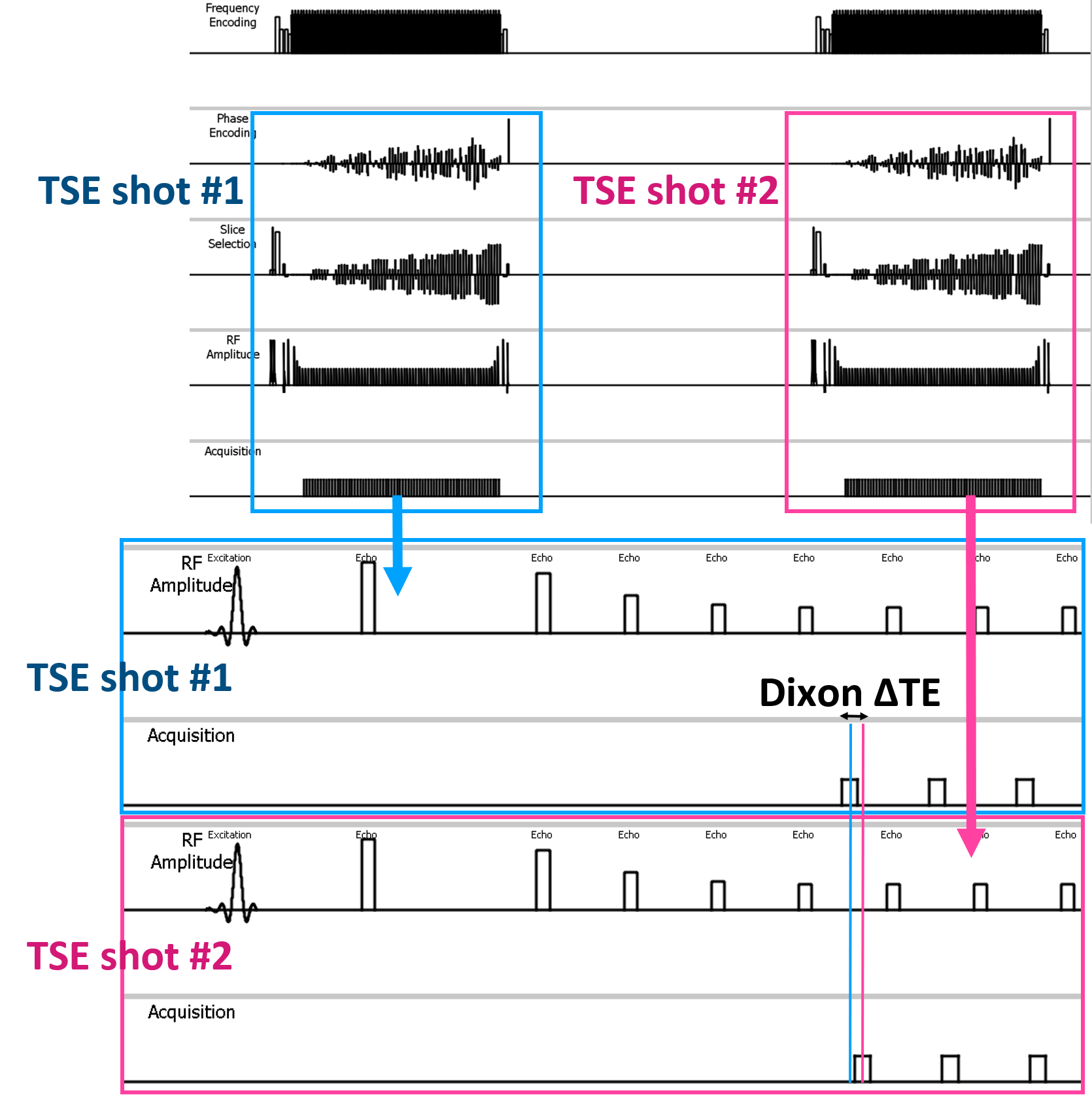
Scheme of the 3D mDixon TSE with CS-AI sequence is shown in Figure 1.

Figure
2. Representative
images of healthy volunteer . CS reduced
the noise in the center of the SENSE images,
and CS-AI even further cleaned up the
noise compared to CS.
Figure
3: The results of visual evaluation regarding cartilage and ligaments. For
overall image quality, sharpness and noise, CS-AI was showed significantly
higher than CS and SENSE.

Figure
4. Representative
images of healthy volunteer . CS reduced
the noise in the center of the SENSE images,
and
CS-AI even further cleaned up the noise compared to CS.
DOI: https://doi.org/10.58530/2024/5049