5043
Clinical value of a 10-minute deep-learning reconstruction fast spinecho knee magnetic resonance imaging protocol including T2 mapping1Renmin Hospital of Wuhan University, Wu Han, China, 2GE Healthcare China, Beijing, Beijing, China
Synopsis
Keywords: Cartilage, Quantitative Imaging
Motivation: T2 mapping is difficult to be implemented in clinics for long scan time.
Goal(s): To propose a 10-minute fast spin echo knee MRI protocol including quantitative T2 map and morphologic images in identifying cartilage injury or grading cartilage degeneration.
Approach: To subjectively and objectively assess the clinical value of knee imaging with different acceleration factor of 2 and 3 as well as using conventional and deep learning reconstruction algorithms (CR, DLR).
Results: Both FSEDLR and DL-based quantitative T2 map with either an acceleration factor of 2 or 3 elevated diagnostic accuracy using a senior rater as a final diagnosis.
Impact: A knee protocol including deep-learning based FSE structure imaging and quantitative T2 map could be facilitated in clinical application further elevating the diagnostic accuracy and performance.
Introduction
Fourier transform has been widely used to reconstruct k-space data and combing parallel imaging (PI), compressed sensing (CS) and multi-layer acquisition can speed up MRI acquisition and image computation[1]. Higher acceleration factors bring under-sampling and scarce high-frequency data and also contribute to lower signal-noise ratio (SNR) or more image blurring. In recent years, deep learning reconstruction (DLR) algorithm has great potential to improve image quality via removal of MR image noise and truncation artifacts in skeletomuscular systems[2]. This study aimed to validate the clinical value of a feasible rapid knee MRI protocol especially including quantitative T2 mapping using both PI and DLR methods at the aspects of qualitative and quantitative evaluation.Materials and methods
92 patients with suspected knee lesions prospectively enrolled to undergo 2D FSE based routine knee scan and 39 of whom also underwent T2 mapping with an acceleration factor of 2 or 3 for parallel imaging on 3.0T MRI (Signa Architect, GE Healthcare). All image data were reconstructed using conventional and deep learning reconstruction algorithms as FSEO, FSEDLR, T2O-ARC=2/3, and T2DLR-ARC=2/3. Subjective evaluation for overall image quality, sharpness and diagnostic confidence using 5-point Likert scale and objective assessment for signal-noise ratio and contrast-to-noise ratio was carried out. Diagnostic performance and accuracy was respectively done using arthroscopic diagnosis and diagnosis of a senior radiologist as reference.Results
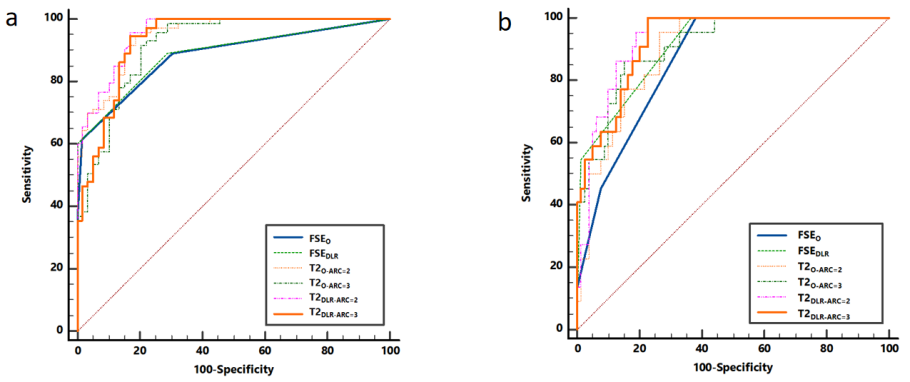
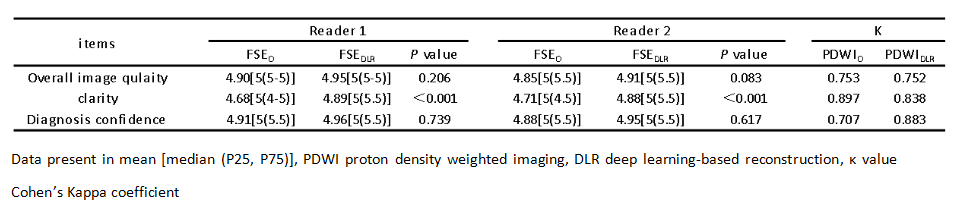
Inter-reader agreement of subjective assessment ranged from 0.707 to 0.897 and higher score on FSEDLR than FSEO (P < 0.05) (Table I). Both SNR and CNR of PDWIDLR were partly higher than those of PDWIO (P<0.05). The accuracy and sensitivity of PDWIDLR for evaluating knee cartilage injury were higher than those of PDWIO (Fig. 1). ROC curve analysis showed that T2DLR-ARC=2 had the highest diagnostic efficacy in differentiating group A (with cartilage 0 and 1) from group B (cartilage 2, 3) while Delong test showed no significant between-method difference of AUCs (Fig. 2). Moreover, the diagnostic accuracy of knee injury evaluation using both routine FSEDLR images and T2DLR-ARC=2 by a junior radiologist was improved by 13.8%-25% using a senior one as a final diagnosis (Table II).Discussion
We firstly proposed a feasible rapid routine knee imaging protocol including T2 mapping using an inline deep learning-based reconstruction 2D FSE sequences and referred to arthroscopic results. DLR-based routine FSE images showed superior image quality to conventional reconstruction images. Moreover, a younger radiologist had higher diagnostic performance on differentiating cartilages especially with grade 0 and I from those with grade II. An optimized 2D-FSE-based routine imaging and T2 mapping for knee MRI was proposed, contributing to elevation of clinical utility. In terms of speed, the total scan time for T2 mapping with the acceleration factor of 3 was reduced by 42%, and the image quality still could meet the needs for diagnosis. Reducing scan time saves costs, increases patient comfort, and possibly reduces motion artifacts, and further elevates diagnosis accuracy for early diagnosis of defects on knee [3, 4]. In the near future, early alterations of signal intensity might assist clinicians to select appropriate therapeutic treatment for patients and their follow-ups. A knee imaging protocol including quantitative information (T2 relaxation time) using deep learning reconstruction technology can significantly shorten acquisition time and elevate diagnostic accuracy especially made by a junior radiologist.Conclusions
This proposed FSE-based imaging protocol has great clinical value in diagnosis of knee injury.Acknowledgements
No acknowledgement found.References
1.Johnson PM, Lin DJ, Zbontar J, Zitnick CL, Sriram A, Muckley M, et al. Deep Learning Reconstruction Enables Prospectively Accelerated Clinical Knee MRI. Radiology 2023: 220425.2.Herrmann J, Keller G, Gassenmaier S, Nickel D, Koerzdoerfer G, Mostapha M, et al. Feasibility of an accelerated 2D-multi-contrast knee MRI protocol using deep-learning image reconstruction: a prospective intraindividual comparison with a standard MRI protocol. European Radiology 2022; 32: 6215-6229.3.Yu A, Heilmeier U, Kretzschmar M, Joseph GB, Liu F, Liebl H, et al. Racial differences in biochemical knee cartilage composition between African-American and Caucasian-American women with 3T MR-based T2 relaxation time measurements - data from the Osteoarthritis Initiative. Osteoarthritis and Cartilage 2015; 23: 1595-1604.4.Chaudhari AS, Stevens KJ, Wood JP, Chakraborty AK, Gibbons EK, Fang Z, et al. Utility of deep learning super-resolution in the context of osteoarthritis MRI biomarkers. J Magn Reson Imaging 2020; 51: 768-779.Figures
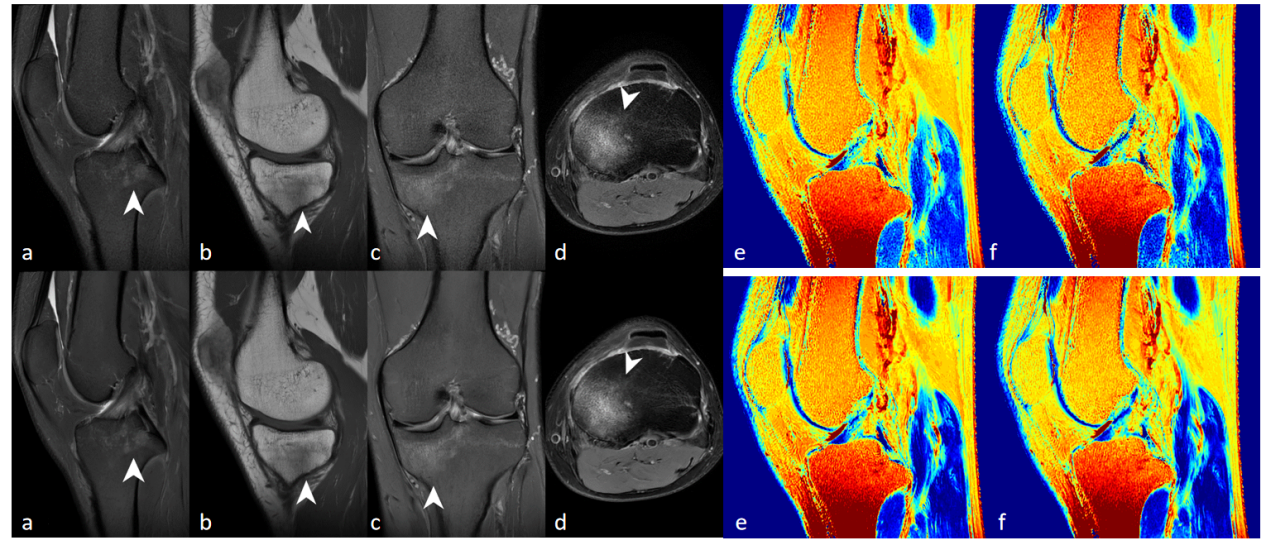
Fig. 1 A 31-year-old patient with pain in the medial side of the left knee after trauma. The original (upper row) and deep learning-based reconstruction (lower row) (a) T1WI, (b, c) fat-suppression PDWI, (d) fat-suppression T2WI, and (e, f) T2 mapping were shown. FSEDLR showed higher image quality with less noise and better clarity of the anatomic structures. Note that bone marrow edema (white arrowheads) of the tibial plateau is clearly definable on both FSEO and FSEDLR.