5030
White Matter Microstructure Alterations and Their Link to Symptomatology in Early Psychosis and Schizophrenia1Lausanne University Hospital (CHUV), Lausanne, Switzerland, 2University of Lausanne, Lausanne, Switzerland, 3University of Lausanne (UNIL), Lausanne, Switzerland
Synopsis
Keywords: Psychiatric Disorders, White Matter, Neuroinflammation, DKI, DTI, DWI, Psychosis
Motivation: Schizophrenia features complex symptomatology. Increased dMRI measures specificity is the key to capture the relation of white matter microstructure alterations with patients psychopathology.
Goal(s): We aim to better characterize WM pathology and, thus, understand its relation with the symptomatology of early-psychosis and schizophrenia.
Approach: Diffusion Kurtosis Imaging and White Matter Tract Integrity–Watson were estimated in 275 individuals. Whole-brain WM estimates were compared between patients and controls, and associated with patients psychopathology.
Results: dMRI patterns suggest that WM alterations are already present and widespread in EP. Two trends of WM deterioration with concomitant demyelination vs neuroinflammation were found associated with clinical scales regression analysis.
Impact: Our findings possibly provide a missing link between specific symptoms and underlying pathology. The association between patients' psychopathology and advanced dMRI metrics may spark further interest in linking specific symptom in psychiatry diseases to microstructure alterations.
Introduction
Clinical studies on schizophrenia featured diffusion magnetic resonance imaging (dMRI) as main means of investigation and identified pathological white matter (WM) as a feature of the disease1,2,3. The complexity of the symptomatology when related to the limited specificity of diffusion tensor imaging(DTI) metrics highlights the importance of increasing our measure specificity. By employing the more comprehensive Diffusion Kurtosis Imaging(DKI)4, and the microstructure model, White Matter Tract Integrity – Watson(WMTI-W)5, we aim to better characterise WM pathology in early psychosis and schizophrenia, and as a result, better relate and understand WM microstructure alterations in relation to the observed symptomatology.Methods
Data from 275 subjects (Table 1) were collected on two scanners (Siemens 3T Prisma and Trio), divided as N=93 patients with early psychosis (EP), 47 with chronic schizophrenia (SZ), and N=135 healthy individuals (HC) that were further subdivided into younger (HC-Y, N=130) and older (HC-O, N=84) to better match the age ranges of the clinical groups. MRI: Diffusion-weighted images were acquired using a PGSE-EPI sequence (TE/TR=0.144/6.1s, 2-mm isotropic resolution, 15 b-values, range 0-8 ms/μm2, Cartesian q-space coverage totaling 129 (Trio, Prisma) or 257 (Trio) images) were acquired. After standard preprocessing6, diffusion and kurtosis tensors and their derived scalars maps (axial, mean, radial diffusivity (AD/MD/RD) and kurtosis (AK/MK/RK), and fractional anisotropy (FA)) were estimated for diffusion data acquired with b≤2.5 ms/μm2. The WMTI-W model parameters were computed using an in-house Python script. The model disentangles axonal water fraction f, intra-axonal diffusivity Da, extra-axonal axial and radial diffusivities De//, De,⊥, and axon orientation alignment C2. WM labels from the JHU template were back projected to individual space using a registration-based approach using ANTs. Mean value along the global WM as well as the average value inside all the regions defined in the atlas were computed for each microstructure metric and harmonised for scanner type using ComBat7. WM core differences between groups were tested via the Wilcoxon test after controlling for sex,age (quadratic),age-at-first-psychosis episode, illness duration and chlorpromazine equivalent doses. Scales: Patients' psychopathology was measured via the Positive and Negative Syndrome Scale (PANSS)8, the Young Mania Rating Scale (YMRS)9, and MADRS,GAF,SOFAS scales (Table 1). Correlation analysis was performed between WM core microstructure metrics and the psychiatric scales. After FDR correction, significant correlations were further investigated with robust linear models, controlling for the same covariates mentioned above.Results
Several group differences were found (Fig. 1). Compared to HC-Y, EP showed significantly higher DTI diffusivities, lower FA (Fig. 2A-D) and lower kurtosis (Fig. 2E-G). Axonal water fraction, f, and alignment, C2 ,were also significantly lower in EP than HC-Y (Fig. 2H,L), while extra-axonal diffusivities, De,// and De,⊥, were higher (fig. 2J,K). SZ vs HC-O showed no DTI differences but lower kurtosis (Fig. 2E-G). The WMTI-W metrics showing significant differences were lower f (Fig. 2H) and higher Da and De,// in SZ when compared to HC-O (Fig. 2I,J). In the association of psychiatric tests with microstructure estimates, the SZ group showed a higher number of significant relations than EP (Table 2). While DTI diffusivities were generally higher in EP vs HC-Y, within the EP group, worse clinical scores at PANSS P5 grandiosity, G14 poor impulse control, and G3 guilt feelings were associated with lower MD and AD (Table 2). Interestingly, SZ displayed higher diffusivities and lower kurtosis in manic symptoms (PANSS P4 excitement, YMRS, Table 2, Fig. 3), while in other features, a worse score was on the contrary associated with lower diffusivity and higher kurtosis (P3 hallucinatory behaviour, N6 lack of spontaneity, Table 2, Fig. 2) - similarly to the associations in the EP group. No association was found with MADRS, GAF or SOFAS domains.Discussion and conclusion
The dMRI patterns in EP and SZ highly suggest that WM atrophy is already present and widespread in the early psychosis stage in comparison to HC-Y, while differences in dMRI microstructure are less dramatic between chronic SZ and HC-O. Speculatively, two competing pathological mechanisms could explain these findings. WM deterioration10 with concomitant demyelination increase diffusivities and reduce kurtosis, while neuroinflammation11 would have the opposite effect of reducing diffusivities and increasing kurtosis due to higher cellular crowding associated with microgliosis and astrocytosis11. The clinical scales regression analysis supports this conclusion, revealing a part of the associations in contrast with the age-matched microstructure group comparisons. When considering different sets of symptoms, namely excitement and manic behaviour, worse scores within the SZ group correlated with the signature of deteriorated WM, while the remaining associations supported WM changes typically associated with neuroinflammation. These findings might provide a missing link between specific symptoms and underlying pathology.Acknowledgements
T. Pavan and I. Jelescu are supported by SNSF Eccellenza PCEFP2_194260. Dr Alameda is supported by Carigest fellowship and by Frutiger Adrian et Simone fellowship.References
[1] Kelly et al., Mol Psychiatry 2018. [2] Kubicki et al., Curr. Opin. Psychiatry 2014. [3] Hanlon et al., Schizophrenia research 2021. [4] Jensen & Helpern, NMR In Biomedicine 2010. [5] Jespersen et al., Neuroimage 2018. [6] Ades-Aron et al., Neuroimage 2018 [7] Fortin et al., Neuroimage 2017. [8] Kay et al. Schiz. Bull. 1987. [9] Young et al., Brit. J. Psyc. 1978. [10] Cetin-Karayumak et al., Mol. Psy. 2020 [11] Jelescu and Fieremans, ch. 2, Imaging neuroinflammation 2023.Figures
Table 1: Cohort demographics. P-values refer to the Wilcox’s tests between clinical and healthy control groups. Sex proportions are tested via Chi-squared test. The significant difference in age between groups was corrected for quadratic age effects. HC: healthy controls, Y: young, O: old, EP: early psychosis, SZ: chronic schizophrenia.
Figure 1: Stir plot group comparisons. Each clinical group is compared to its respective HC group. Interestingly, EP showed stronger alterations than SZ in kurtosis (E,F,G) but especially in diffusivities (A,B,C). The estimated axonal fraction, f, was similarly decreased for EP and SZ with respect to their HC (H), while the altered EP diffusivities were localised in the extra-axonal compartment (J,K). EP: early psychosis, SZ: chronic schizophrenic, HC-Y/O: healthy controls young/old. *:p≤5e-2, **:p≤1e-2, ***:p≤1e-3, ****:p≤1e-4.
Table 2: Significant associations between DKI, WMTI-W metrics, and PANSS, YMRS. Red/blu arrows: positive/negative association. Results can be classified into two categories: neuroinflammation-like and WM deterioration-like. Neuroinflammation has a signature of a decrease in diffusivities (RD,MD,AD,De,⊥) and increase in complexity metrics (RK,FA,f). The opposite trends are expected for deterioration (as in SZ for P4 YMRS). PANSS subscales: P5-grandiosity, G3-poor impulse control, G14-guilty feelings. P3-hallucinatory behaviour, P4-excitement, N6-lack spontaneity
Figure 2: Significant associations between dMRI metrics and PANSS P3 Hallucinatory Behaviour sub-scale in SZ, showing association resembling neuroinflammation-like features with dMRI metrics. RK and f significantly increase with worst scores in hallucinatory behaviour, while MD decreases. During neuroinflammation, the higher cellular crowding associated with microgliosis and astrocytosis increases the kurtosis (RK) and the estimated neurites (f), while decreasing the measured water displacement (MD).
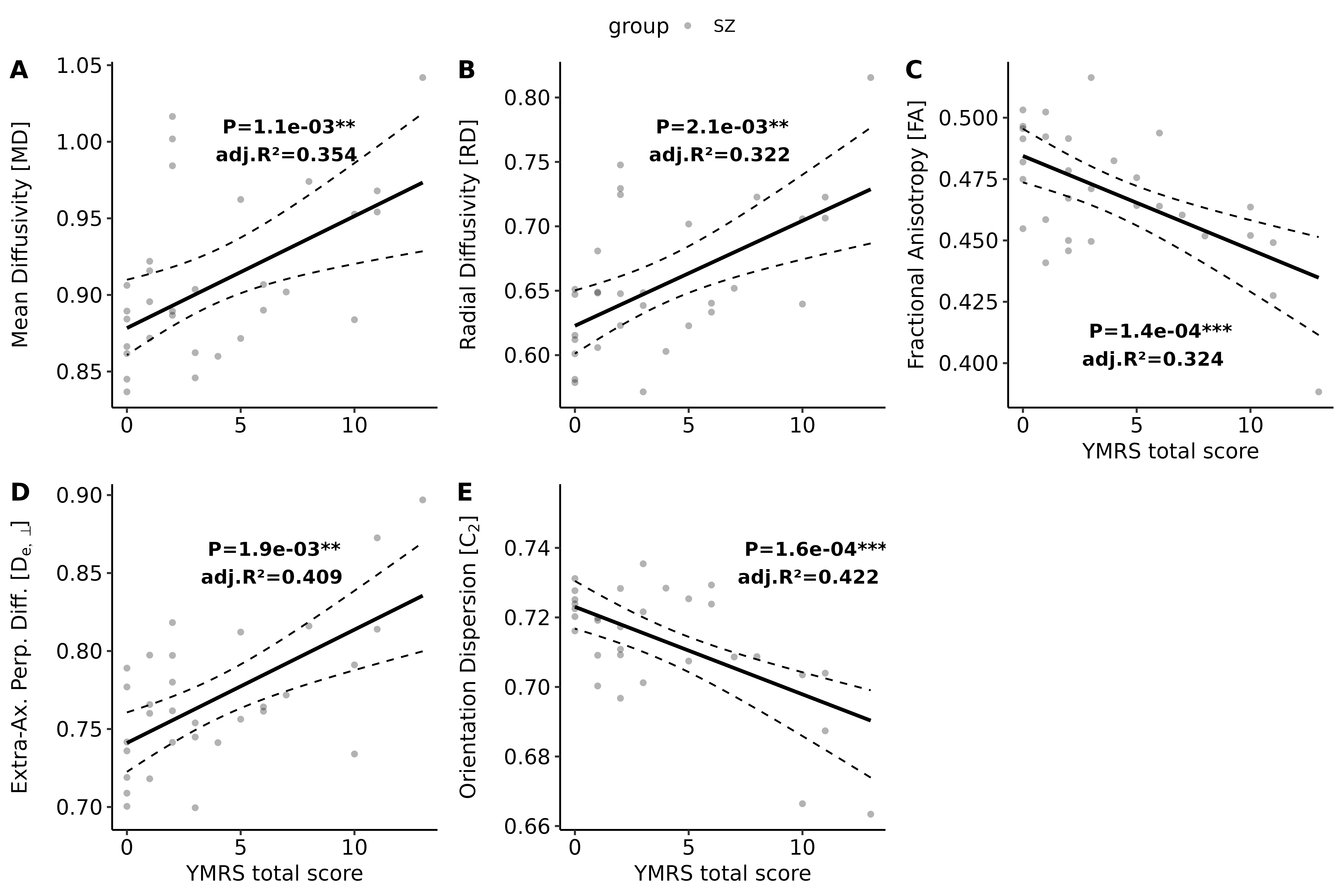
Figure 3: Significant associations between dMRI metrics and YMRS in SZ, showing association resembling WM deterioration features with dMRI metrics. Diffusivities significantly decrease with worst manic symptoms, while FA and C2 increase. Characteristics of WM deterioration are phenomena like demyelination, volume loss or dystrophic glia, whose effects mainly reflect on the diffusion signal as increased water displacement (MD,RD,De⊥), but also reduced fibre coherence, alignment (FA,C2).