5029
Pretreatment brain magnetic resonance imaging outperforms clinical ratings in predicting major depressive disorder treatment outcomes1Department of Radiology and Huaxi MR Research Center (HMRRC), Functional and Molecular Imaging Key Laboratory of Sichuan Province, West China Hospital, Sichuan University, Chengdu, China
Synopsis
Keywords: Psychiatric Disorders, MR Value
Motivation: It is clinically needed to explore predictive potential of pretreatment features in major depressive disorder (MDD) treatment outcomes to guide personalized medicine approaches.
Goal(s): To evaluate and compare overall predictive performance of clinical and brain magnetic resonance imaging (MRI) features for treatment outcomes and assess performance of distinct modalities and interventions in MRI studies.
Approach: We conducted separate meta-analyses on clinical and MRI studies followed with subgroup meta-analyses and meta-regression.
Results: MRI studies outperformed clinical studies in sensitivity. Within MRI group, resting-state functional MRI exhibited higher specificity than task-based functional MRI . No significant differences were found among remaining modality and intervention subgroups.
Impact: Our findings highlight the potential of utilizing pretreatment brain MRI data to predict treatment outcomes for MDD. This is valuable for using MRI features to early identify patients' treatment outcomes, potentially assisting clinicians in considering alternative treatment options.
Introduction
MDD is a highly prevalent and disabling condition 1. Approximately 30-50% of MDD patients do not respond to first-line medication or psychotherapy 2. Recent studies proved that pretreatment clinical severity ratings and brain MRI data can predict treatment outcomes. A meta-analysis of this growing literature can help us understand brain basis of variability in treatment outcomes, compare predictive utility between clinical and MRI features, and explore variations within MRI studies.Methods
We followed PRISMA guidelines, searched studies in PubMed, Embase, Web of Science, and Science Direct databases before June 22, 2023, and extracted prediction confusion matrices. We conducted separate meta-analyses for studies based on clinical features, encompassing demographics and severity ratings (Hamilton depression rating scale [HDRS] scores, illness duration, sleep quality, etc.), and based on MRI features. The logarithm of diagnostic odds ratio [log(DOR)] was summarized as a predictive result. We conducted sensitivity and specificity using Reitsma’s approch 3. The area under curve (AUC) of summary receiver operating characteristic (SROC) curve was calculated.Subgroup analyses were conducted in MRI studies based on modalities: resting-state functional MRI (rsfMRI), task-based fMRI (tbfMRI, subdivided into emotional and cognitive task subgroups), and structural MRI; and interventions: antidepressant (including selective serotonin reuptake inhibitors) and electroconvulsive therapy (ECT).
Meta-regression was used firstly to explore the effects of covariates (sample size, age, sex ratio, etc.) on sensitivity and specificity 4. Subsequently, it assessed differences 1) between clinical and MRI studies, and 2) among modality or intervention subgroups in MRI studies. We constructed a multivariate regression model for predicting log(DOR) in each study to examine variables’ impact on prediction.
Results
We included 13 clinical studies and yielded a log(DOR) of 1.62. The AUC, sensitivity, and specificity were 0.73, 0.62, and 0.76. In 44 MRI studies, the log(DOR) was 2.53. The AUC, sensitivity, and specificity were 0.89, 0.78, and 0.75 (Figure 1).MRI studies had higher sensitivity in predicting treatment outcomes than clinical studies (P = 0.001). The rsfMRI had higher specificity (0.79 vs. 0.69) than tbfMRI studies (P = 0.004). No significant differences were found among the remaining modality and intervention subgroups (Table 1). For covariates, HDRS scores impacted specificity in emotional task subgroup (P = 0.004), and sample size influenced sensitivity in ECT treatment outcomes (P < 0.001). In MRI studies, antidepressant studies primarily identified predictive neuroimaging features in limbic and default mode networks (DMN), while ECT mainly focused on limbic network.
The predicted log(DOR) correlated with true log(DOR) only within MRI group (r = 0.39, P = 0.02), identifying six variables based on their coefficient absolute values (Figure 2).
Discussion
The present meta-analysis findings highlight the potential of utilizing pretreatment brain MRI data to predict treatment outcomes for MDD patients, outperforming the accuracy of clinical studies. While all clinical studies include symptom rating scale scores, variations in other features (such as comorbidities and duration) introduce heterogeneity, potentially limiting predictive performance of clinical features.The enhanced predictive power of rsfMRI over tbfMRI is grounded in prior studies, and our multivariate regression result reinforces this conclusion. While methods across studies can vary in terms of how measurements are performed, for tbfMRI there is additional major consideration of what task is being performed during scans. Previous research suggests that increased MDD symptom severity correlates with reduced activation in emotional processing brain regions 5. Individuals with severe symptoms and varied treatment outcomes may exhibit comparable low baseline activation in these regions, hindering accurate prediction of treatment outcomes. Additionally, studies demonstrated that longer MDD duration is associated with reduced volume in hippocampus and anterior cingulate cortex (ACC) 6, along with weakened functional connectivity between ACC and DMN 7. This aligns with crucial regions (limbic and DMN) we identified for prediction, and brain MRI features yield a higher log(DOR) for outcome prediction for patients with a longer illness duration.
Despite distinct mechanisms of antidepressants and ECT, similar sensitivity, specificity, and AUC were observed in prediction using overlapping brain features. We demonstrated that primary distribution of brain regions predicting antidepressant therapy outcomes was in limbic network and DMN, while those for ECT were more specific to limbic network. The interpretation of this similarity is complex, given that many receiving ECT also take antidepressants before and during ECT treatment.
Conclusion
Our findings suggest a robust promise for pretreatment brain MRI features in predicting MDD treatment outcomes, offering higher accuracy than clinical studies. While tasks in tbfMRI studies differed, those studies overall had less predictive utility than rsfMRI data. For MRI studies, overlapping but distinct network-level measures predicted outcomes for antidepressants and ECT.Acknowledgements
No acknowledgement found.References
1. World Health Organization. Depression fact sheet. World Health Organization. Published December 2019. Accessed November 20, 2022. https://www.who.int/mediacentre/factsheets/fs369/en/.
2. Davis AK, Barrett FS, May DG, et al. Effects of Psilocybin-Assisted Therapy on Major Depressive Disorder: A Randomized Clinical Trial. JAMA Psychiatry. 2021;78(5):481-489.
3. Reitsma JB, Glas AS, Rutjes AW, Scholten RJ, Bossuyt PM, Zwinderman AH. Bivariate analysis of sensitivity and specificity produces informative summary measures in diagnostic reviews. J Clin Epidemiol. 2005;58(10):982-990.
4. Macaskill P TY, Deeks JJ, Gatsonis C. Chapter 9: Understanding meta-analysis. Draft version (4 October 2022) for inclusion in: Deeks JJ, Bossuyt PM, Leeflang MM, Takwoingi Y, editor(s). Cochrane Handbook for Systematic Reviews of Diagnostic Test Accuracy Version 2. London: Cochrane.
5. Ai H, Opmeer EM, Marsman JC, et al. Longitudinal brain changes in MDD during emotional encoding: effects of presence and persistence of symptomatology. Psychol Med. 2020;50(8):1316-1326.
6. Lemke H, Romankiewicz L, Förster K, et al. Association of disease course and brain structural alterations in major depressive disorder. Depress Anxiety. 2022;39(5):441-451.
7. Sheng W, Cui Q, Jiang K, et al. Individual variation in brain network topology is linked to course of illness in major depressive disorder. Cereb Cortex. 2022;32(23):5301-5310.
Figures
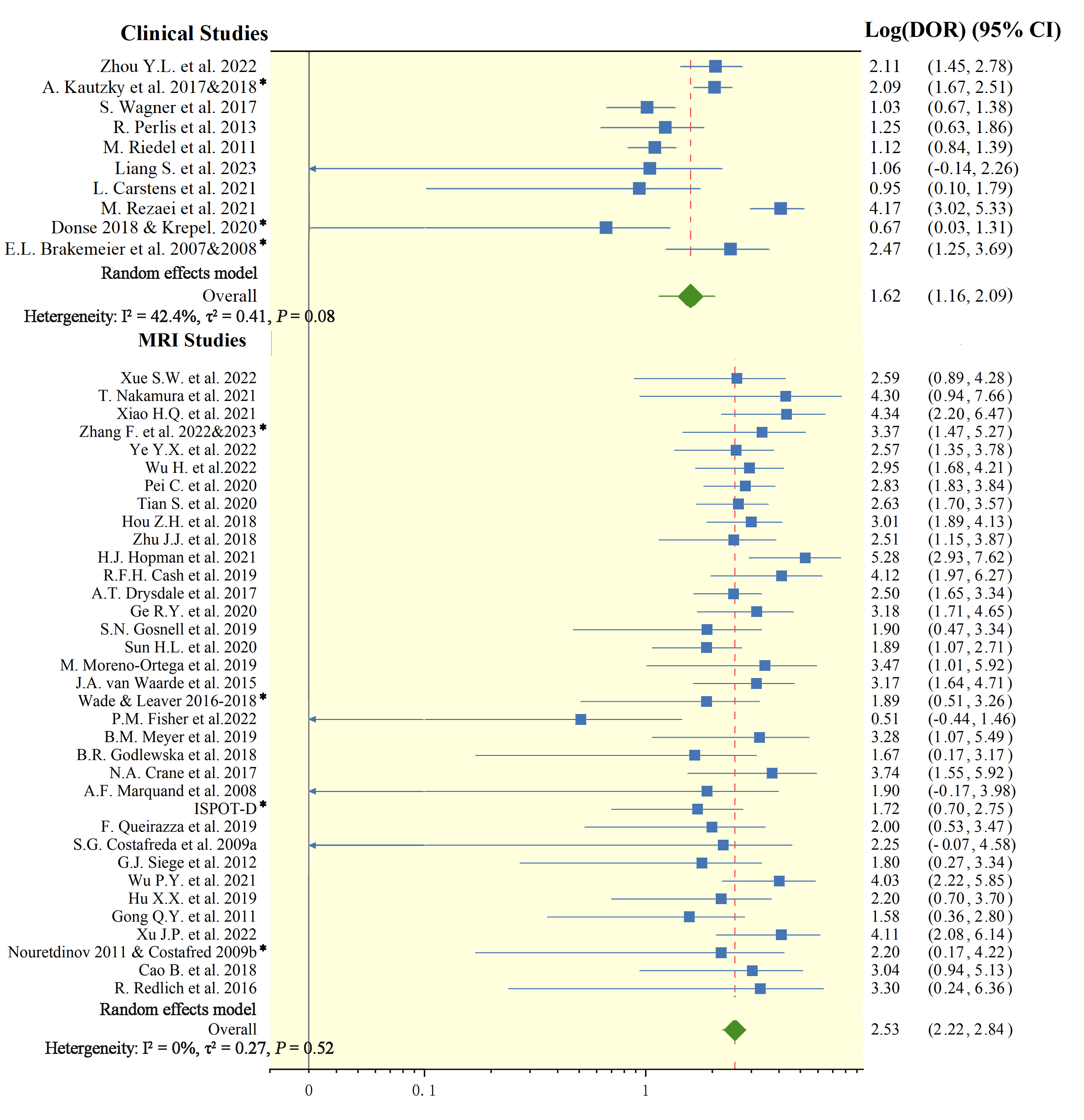
Notes: * represents data after weighted averaging of studies that used repeated samples. ISPOT-D included six studies utilizing the international study to predict optimized treatment in depression data.
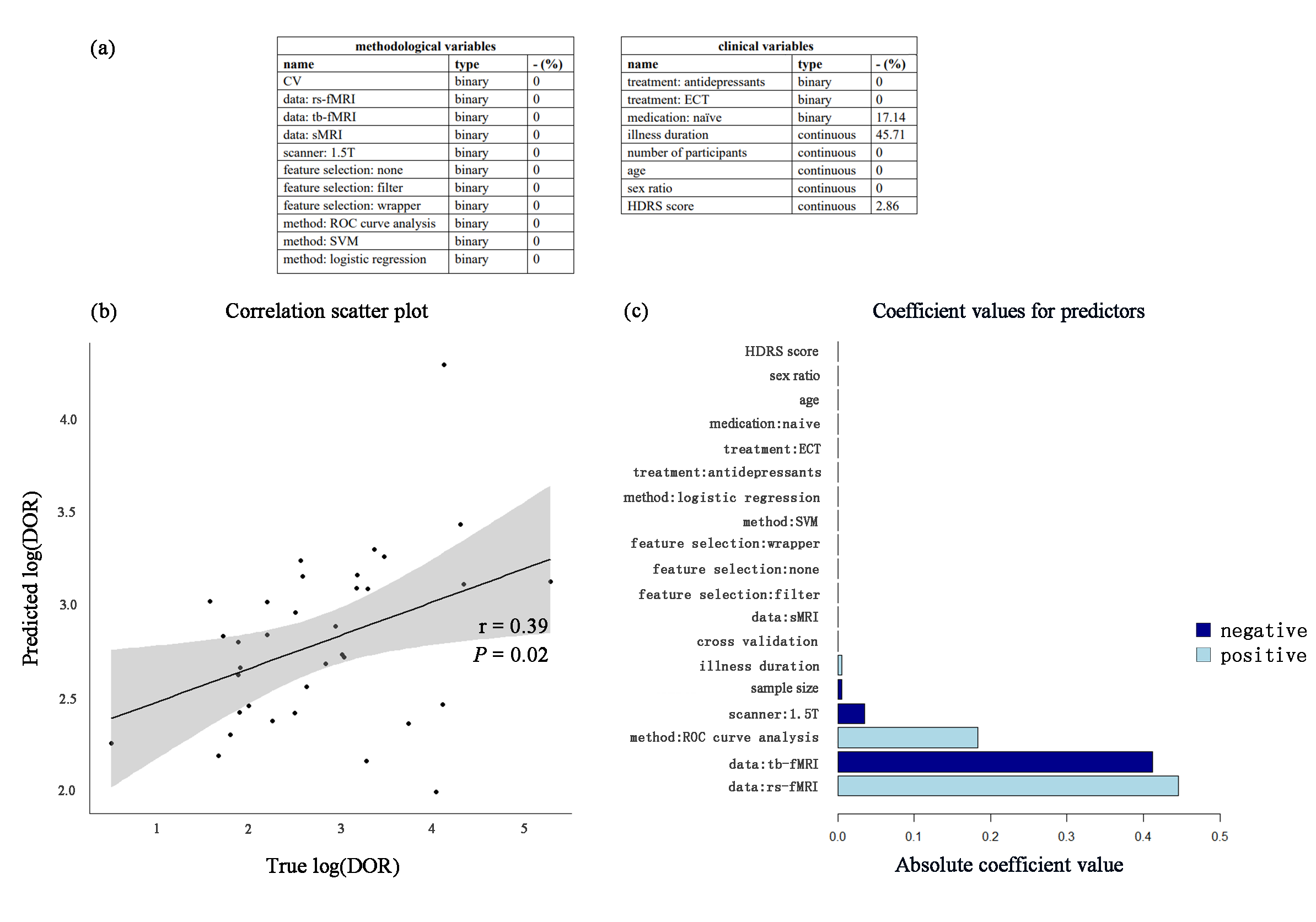
(a) N = 19 methodological and clinical variables included in elastic net algorithm. (b) The predicted log(DOR) was correlated with true log(DOR)(r = 0.39, P = 0.02). (c) Six variables with non-zero coefficients were important predictors for log(DOR) prediction, ranked by their absolute value of coefficient values from lowest to highest.
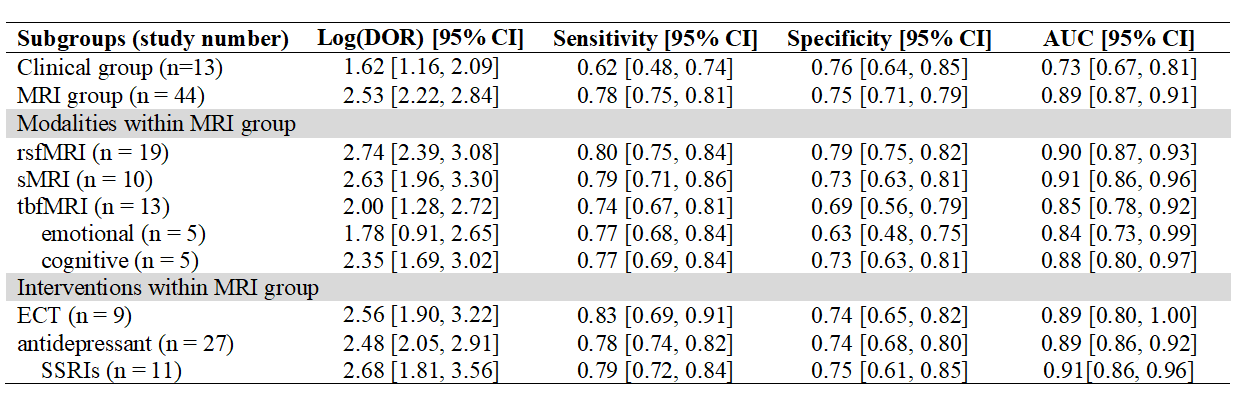
Table 1. Prediction performance of treatment outcomes in the present meta-analysis.