5020
Effects of short-term methylphenidate treatment on functional network connectivity in attention-deficit hyperactivity disorder1Radiology and Nuclear Medicine, Amsterdam University Medical Center, Amsterdam, Netherlands, 2Animal Imaging and Technology core, CIBM Center for Biomedical Imaging, École polytechnique fédérale de Lausanne (EPFL), Lausanne, Switzerland, 3Department of Anatomy and Neurosciences, Amsterdam UMC, Vrije Universiteit Amsterdam, Amsterdam Neuroscience, Amsterdam, Netherlands
Synopsis
Keywords: Psychiatric Disorders, Brain Connectivity
Motivation: Long-term treatment with methylphenidate for ADHD may not sustain initial treatment gains, potentially attributed to the development of tolerance over time. However, the underlying neural mechanisms remain unexplored.
Goal(s): To investigate how methylphenidate treatment alters functional connectivity changes to an acute methylphenidate challenge within three resting-state networks implicated in ADHD dysfunction.
Approach: Resting-state fMRI before and after the challenge was collected in children and adults with ADHD, at baseline and after 16-week treatment with methylphenidate or placebo.
Results: Functional connectivity measures in the frontoparietal network in children became more similar to that of controls after 4-months of methylphenidate treatment.
Impact: Methylphenidate has long-lasting effects on within-frontoparietal network connectivity, but lack of change in response to MPH-challenge after treatment suggests that there is no tolerance in this neurobiological parameter. Future investigations require long term follow-up to investigate neurobiological and symptom tolerance.
Introduction
Methylphenidate is a stimulant medication commonly used in the treatment of attention-deficit hyperactivity disorder (ADHD), with a well-established short-term efficacy. However, treatment gains do not appear to be maintained in the long term1. A possible explanation is that individuals with ADHD develop tolerance after treatment with methylphenidate, yet, research investigating the underlying neural mechanisms is lacking. Therefore, this study investigated how treatment with methylphenidate affects the resting-state functional connectivity (rsFC) within three major networks implicated in ADHD dysfunction2. We hypothesized that (1) rsFC within the attention network (AN), default mode network (DMN) and frontoparietal network (FPN) is altered after a 4-month treatment with methylphenidate, and (2) that rsFC change to an acute methylphenidate challenge is reduced after prolonged treatment. In line with prior research in the same study population, we expect age-dependent effects of methylphenidate on rsFC in this sample3,4.Methods
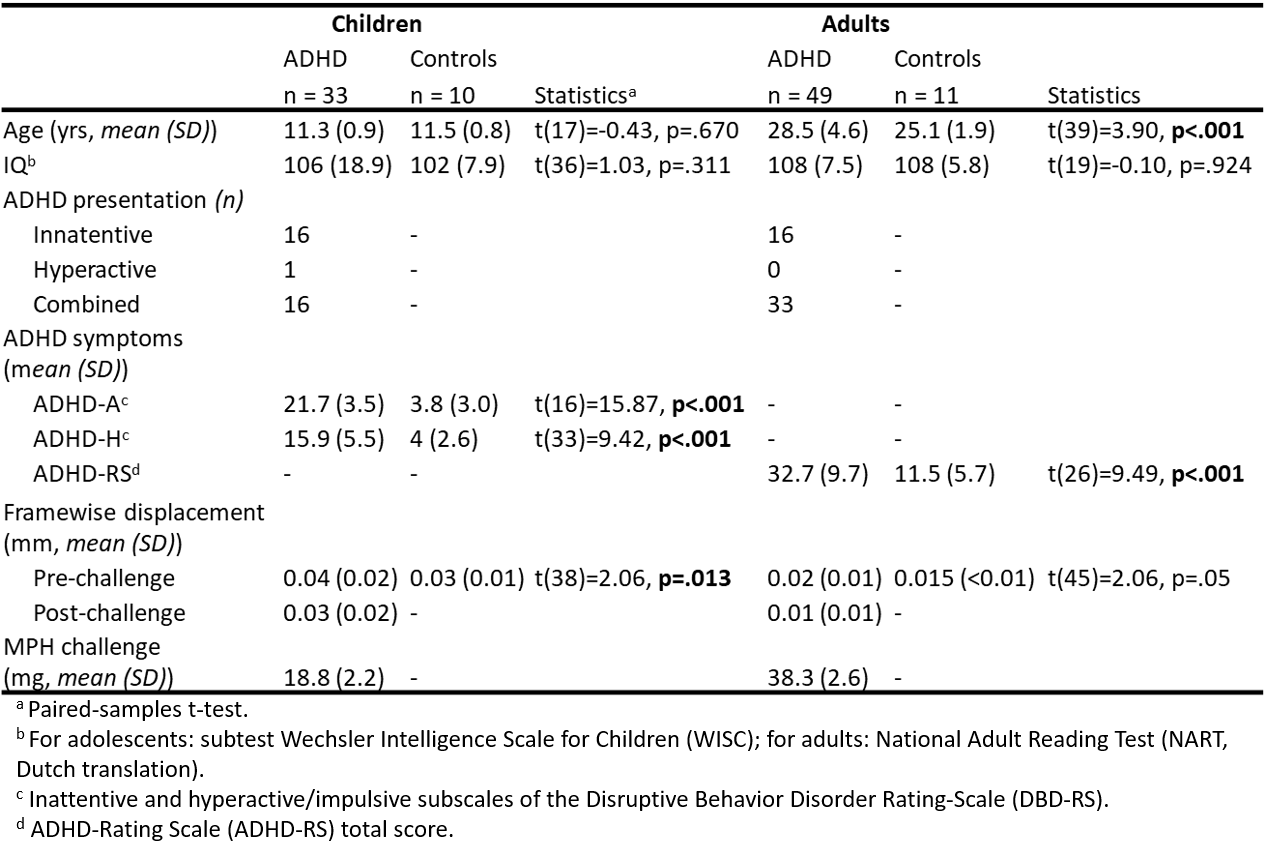
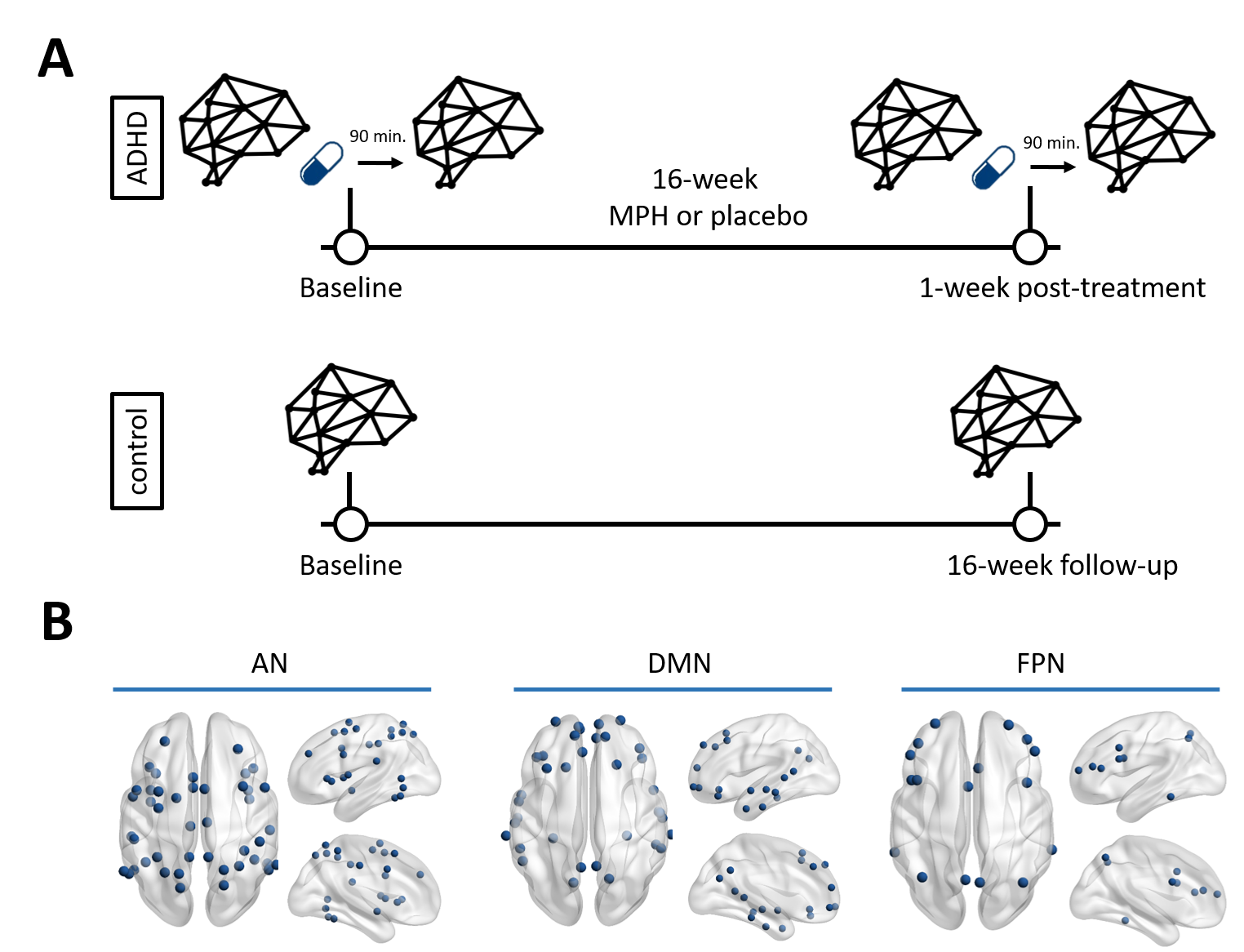
Participants and design: Fifty treatment-naïve boys and 49 stimulant-naïve men, diagnosed with ADHD, participated in a randomized controlled trial, consisting of 16 weeks of treatment with methylphenidate or placebo1,5. Participants underwent rs-fMRI at baseline and post-treatment (with one week washout), before and 90 minutes after an acute oral methylphenidate challenge (0.5mg/kg, Figure 1A). Additionally, 11 boys and 12 men were included as typically developing controls. The control group only underwent the pre-challenge rsfMRI scan and did not receive methylphenidate or placebo treatment. Baseline ADHD symptoms were assessed using the Disruptive Behavior Disorder Rating-Scale (inattention and hyperactivity/impulsivity subscales6) in adolescents, and the ADHD-Rating Scale7 in adults.Acquisition: Data were acquired on 3T Philips scanners (Achieva/Intera) using an 8-channel receive-only head coil. A 3D T1-weighted anatomical scan was acquired for registration purposes, and fMRI data were acquired using a single-shot echo-planar imaging sequence (TR/TE=2300/30ms, resolution=2.3×2.3×3mm, 39 sequential slices, FA=80°, dynamics=130).
Analysis:
Preprocessing was performed using FMRIPREP v1.2.38, including ICA-AROMA. White matter and cerebral spinal fluid signals were regressed out and high-pass-filtering (100s) was applied using FSL. fMRI scans were excluded from analysis if mean framewise displacement >0.2mm or if remaining volumes after scrubbing <104. Time courses were extracted using the Brainnetome atlas9 to construct connectivity matrices (absolutized Pearson correlations). The AN, DMN and FPN were defined based on the Yeo 7-network parcellation10 (Figure 1B). For each scan, connectivity strength (hereafter strength) and eigenvector centrality (hereafter centrality) were calculated to quantify within-network connectivity for each network. Network changes to an acute methylphenidate challenge were calculated as the difference between pre- and post-challenge for each measure. Linear mixed models were used (R4.2.111) to assess main- and interaction effects of age (adolescent/adult), treatment (methylphenidate/placebo) and visit (baseline/post-treatment) on pre-challenge rsFC and pre-to-post-challenge rsFC. Multiple comparison correction (number of networks) was performed using Sidak’s correction (ɑ*=0.017).
Results
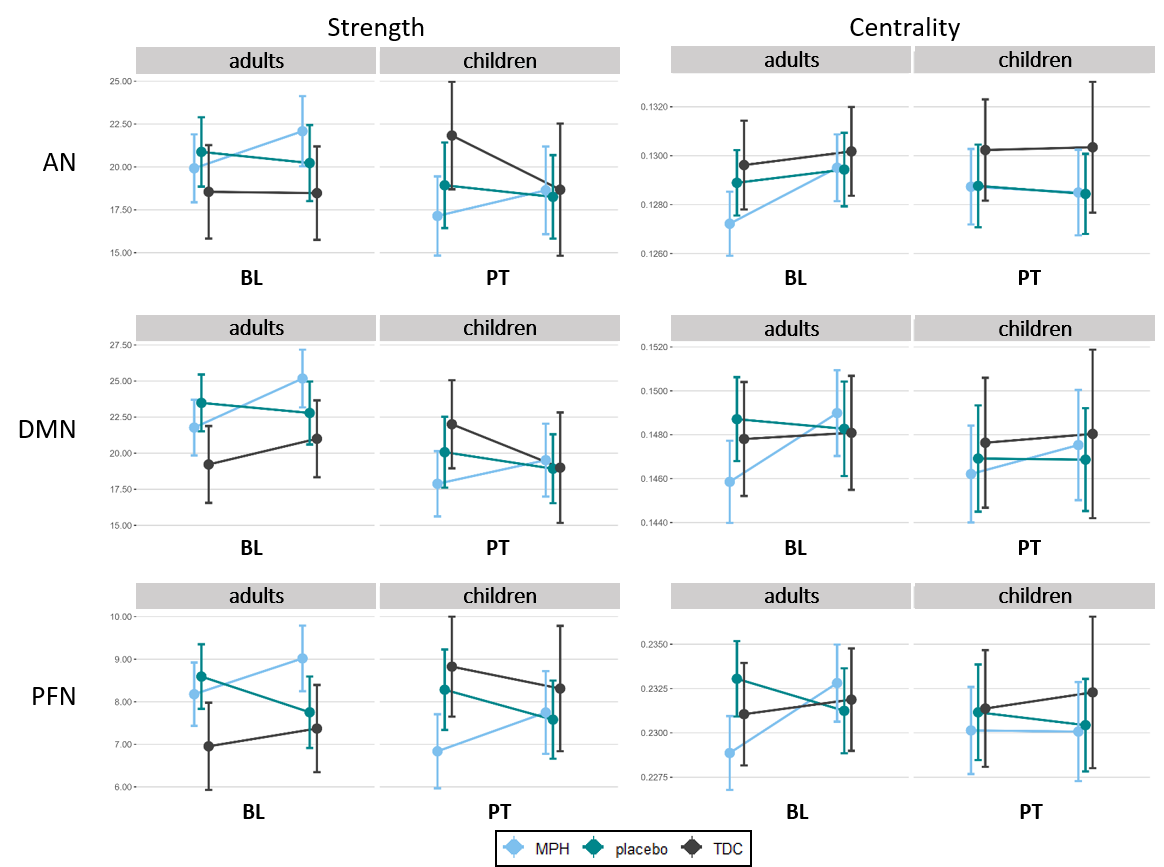
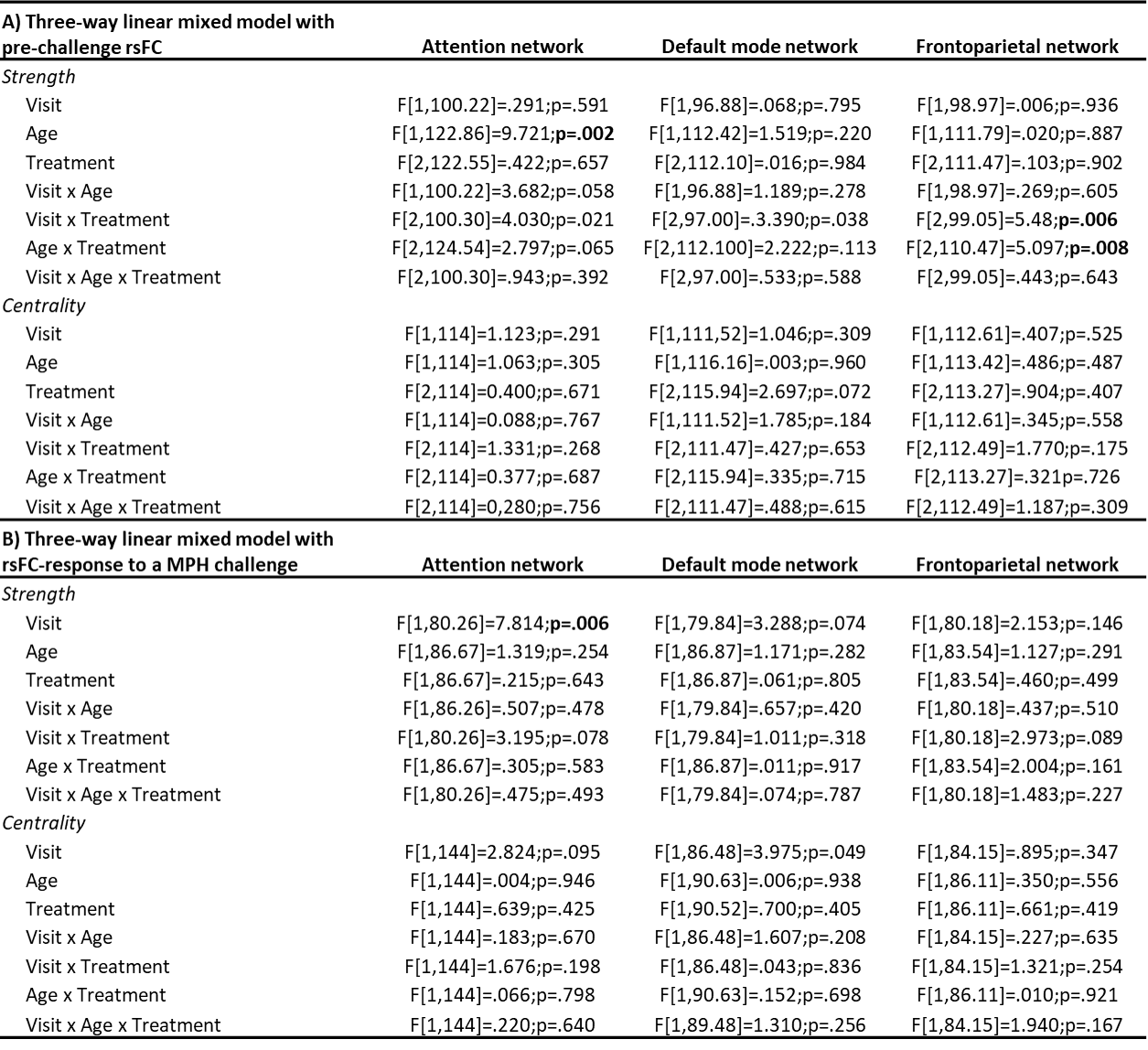
A final sample size of 82 participants (33 children, 49 adults) was retained. Participants were excluded from analysis due to excessive motion as determined during pre-processing. Participant characteristics of the final sample are shown in Table 1.Pre-acute challenge connectivity: For within-FPN rsFC, we found group-by-visit (p=.006) and age-by-treatment (p=.008) interaction effects on strength (Table 2A). Post-hoc analysis revealed opposite changes in strength in the ADHD-methylphenidate (decrease) and ADHD-placebo (increase) groups between baseline and post-treatment, whereas the controls showed no change in strength. Notably, the ADHD-methylphenidate group became more similar in strength to the controls. Moreover, across visits, in the methylphenidate groups, adults had higher strength than children. In contrast, in controls children had higher strength than adults. In addition, we found a main effect of age on within-AN strength (p=.002), with adults showing higher strength than children across visits and treatment groups. No main or interaction effects were identified for within-DMN rsFC or centrality (Figure 2).
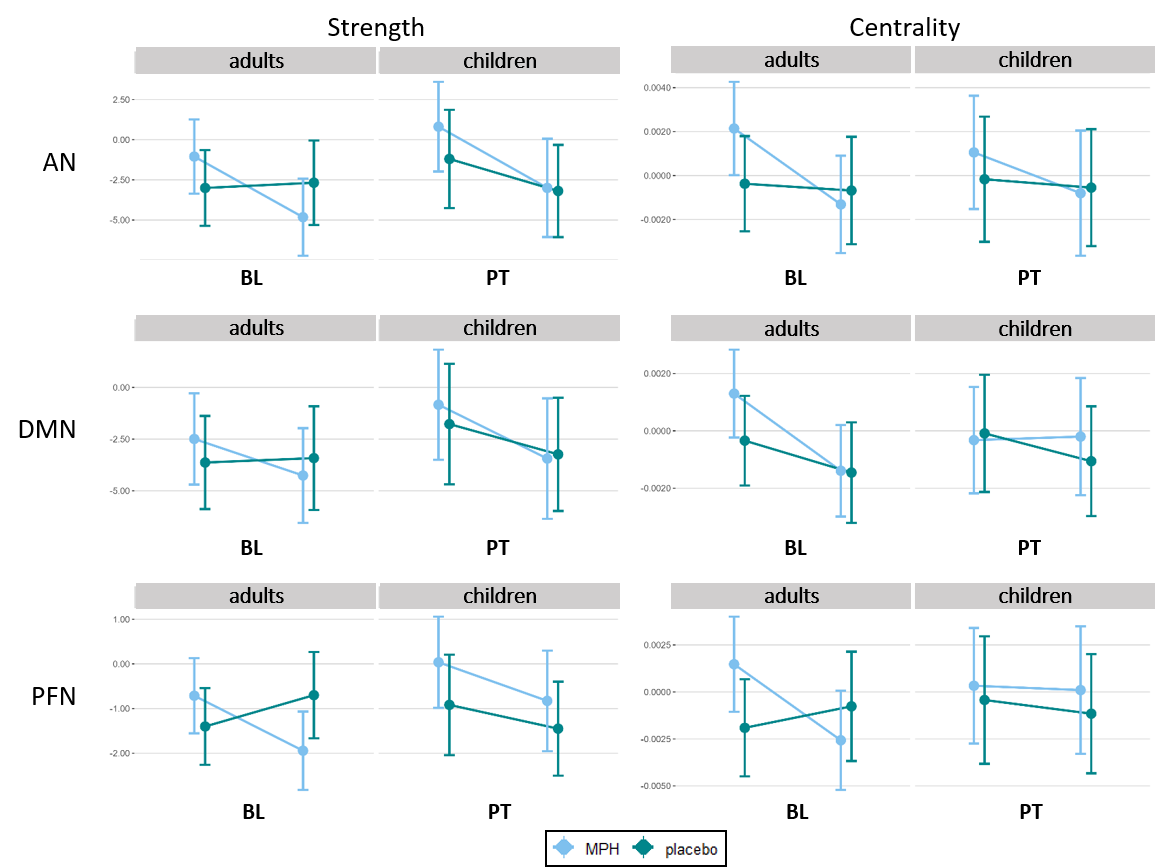
RsFC-response to an acute methylphenidate challenge: We found a main effect of visit on within-AN strength (p=.006; Figure 3, Table 2B). Across all age and treatment groups, we found a larger rsFC-response after a methylphenidate-challenge (i.e., more reduction in strength) at post-treatment compared with baseline. No further main or interaction effects were found.
Discussion
Our findings show that within-FPN strength in children became more similar to that of controls after 4-months of methylphenidate treatment. Moreover, rsFC-response to an acute methylphenidate challenge increased over time across all ADHD groups. However, the lack of change in response to the methylphenicate challenge after treatment suggests that there is no tolerance in this neurobiological parameter. Future studies would benefit from longer treatment intervals to investigate the mid-to-long-term effects on rsFC. Additionally, pre-clinical models can provide information on neurochemical alterations following a long-term treatment with methylphenidate, allowing for making direct inferences on the development of tolerance.Acknowledgements
The RCT was funded by a personal research grant awarded to LR by the Academic Medical Center, University of Amsterdam, and 11.32050.26ERA-NET PRIOMEDCHILD FP 6 (EU). We would like to thank the participants of the effects of Psychotropic drugs On the Developing brain (ePOD-MPH) study for their participation in the study.References
[1] Matthijssen, A.M., Dietrich, A., Bierens, M., Kleine Deters, R., van de Loo-Neus, G.H.H., van den Hoofdakker, B.J., Buitelaar, J.K., Hoekstra, P.J. Continued Benefits of Methylphenidate in ADHD After 2 Years in Clinical Practice: A Randomized Placebo-Controlled Discontinuation Study. Am J Psychiatry. 2019 Sep 1;176(9):754-762.
[2] Gao, Y., Shuai, D., Bu, X., Hu, X., Tang, S., Zhang, L., Li, H., Hu, X., Lu, L., Gong, Q., & Huang, X. (2019). Impairments of large-scale functional networks in attention-deficit/hyperactivity disorder: a meta-analysis of resting-state functional connectivity. Psychological medicine, 49(15), 2475–2485. https://doi.org/10.1017/S003329171900237X
[3] Schrantee, A., Tamminga, H.G., Bouziane, C., Bottelier, M.A., Bron, E.E., Mutsaerts, H.-J.M., Zwinderman, A.H., Groote, I.R., Rombouts, S.A., Lindauer, R.J., Klein, S., Niessen, W.J., Opmeer, B.C., Boer, F., Lucassen, P.J., Andersen, S.L., Geurts, H.M., Reneman, L., 2016. Age-dependent effects of methylphenidate on the human dopaminergic system in young vs adult patients with attention-deficit/hyperactivity disorder. JAMA Psychiatry 73, 955.
[4] Kaiser, A., Broeder, C., Cohen, J. R., Douw, L., Reneman, L., & Schrantee, A. (2022). Effects of a single-dose methylphenidate challenge on resting-state functional connectivity in stimulant-treatment naive children and adults with ADHD. Human brain mapping, 43(15), 4664–4675. https://doi.org/10.1002/hbm.25981
[5] Bottelier, M. A., Schouw, M. L., Klomp, A., Tamminga, H. G., Schrantee, A. G., Bouziane, C., de Ruiter, M. B., Boer, F., Ruhé, H. G., Denys, D., Rijsman, R., Lindauer, R. J., Reitsma, H. B., Geurts, H. M., & Reneman, L. (2014). The effects of Psychotropic drugs On Developing brain (ePOD) study: methods and design. BMC psychiatry, 14, 48.
[6] Pelham WE Jr, Gnagy EM, Greenslade KE, Milich R. Teacher ratings of DSM-III-R symptoms for the disruptive behavior disorders. J Am Acad Child Adolesc Psychiatry. 1992 Mar;31(2):210-8. DOI: 10.1097/00004583-199203000-00006.
[7] Kooij JJS. Diagnostic Instruments. In: Adult ADHD. London: Springer; 2013. DOI: 10.1007/978-1-4471-4138-9_3.
[8] Esteban,O., Ciric,R., Finc,K., Blair,R.W., Markiewicz,C.J., Moodie,C.A., Kent, J. D., Goncalves, M., DuPre, E., Gomez, D. E. P., Ye, Z., Salo, T.,Valabregue, R., Amlien, I. K., Liem, F., Jacoby, N., Stojic, H., Cieslak, M.,Urchs, S.,... Gorgolewski, K. J., 2020. Analysis of task-based functional MRI data preprocessed with fMRI Prep. Nature Protocols, 15,1–17.
[9] Fan, L., Li, H., Zhuo, J., Zhang, Y., Wang, J., Chen, L., Yang, Z., Chu, C.,Xie, S., Laird, A. R., Fox, P. T., Eickhoff, S. B., Yu, C., & Jiang, T., 2016.The human Brainnetome atlas: A new brain atlas based on connectional architecture. Cerebral Cortex, 26, 3508–3526.
[10] Yeo BT, Krienen FM, Sepulcre J, Sabuncu MR, Lashkari D, Hollinshead M, Roffman JL, Smoller JW, Zöllei L, Polimeni JR, Fischl B, Liu H, Buckner RL. The organization of the human cerebral cortex estimated by intrinsic functional connectivity. J Neurophysiol. 2011 Sep;106(3):1125-65. doi: 10.1152/jn.00338.2011. Epub 2011 Jun 8. PMID: 21653723; PMCID: PMC3174820.
[11] R Core Team (2022). R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. URL https://www.R-project.org/.
Figures