5016
Predictive value of Intravoxel incoherent motion diffusion-weighted MR imaging in different expression states of HER2 in breast cancer1First Affiliated Hospital of Dalian Medical University, Dalian, China, 2GE Healthcare,MR Research China, Beijing, China
Synopsis
Keywords: fMRI Analysis, Breast, Breast cancer;HER2;IVIM
Motivation: This study aimed to predict HER2 expression states in breast cancer patients using IVIM imaging, offering valuable guidance for anti-HER2 treatment.
Goal(s): To categorize patients into HER2-positive, HER2-low, and HER2-zero groups, analyze IVIM parameters, and assess their relationship with clinicopathological features.
Approach: 67 breast cancer patients were retrospectively analyzed, with IVIM imaging and data collection. Statistical tests were employed to compare the groups.
Results: While no significant differences emerged in clinicopathological features, ADCfast values differed significantly. Both HER2-positive and HER2-low subgroups exhibited higher ADCfast values than HER2-zero cases. ADC, ADCslow, and f showed no significant variations.
Impact: This study demonstrates that ADCfast can predict HER2 expression noninvasively, assisting in personalized treatment planning and prognosis assessment for breast cancer patients pre-surgery, providing valuable insights for clinical decision-making.
Inturoduction
HER2-low breast cancer is defined as having immunohistochemically (IHC) 1+ or 2+ expression and the absence of HER2 gene amplification as determined by in situ hybridisation[1]. Breast cancer cases with different HER2 expression levels, including HER2-zero, HER2-low, and HER2-positive, exhibit distinct clinicopathological features, biological behavior, chemosensitivity, and prognosis[1]. This study aims to investigate the prediction of these three different HER2 expression states using intravoxel incoherent motion (IVIM) diffusion-weighted MR imaging, providing imaging-based guidance for clinical identification of breast cancer patients suitable for anti-HER2 treatment.Methods
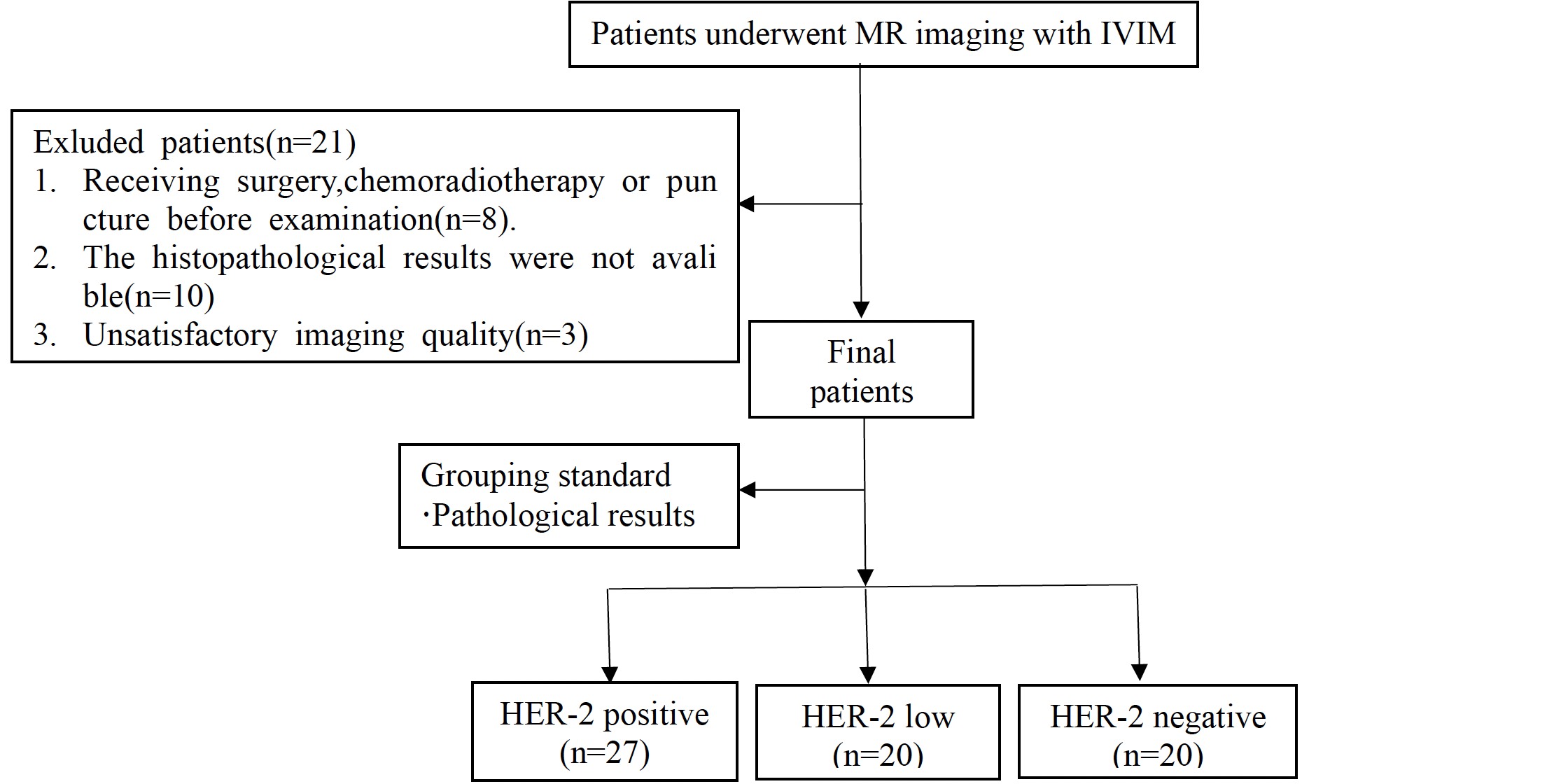
This study involved a retrospective analysis of 67 breast cancer patients who reveived pathological confirmation from January 2019 to February 2023. Patients were divided into three groups based on immunohistochemistry results: HER2 positive group, HER2 low expression group, and HER2 zero group. Before surgery, all patients underwent IVIM imaging. The clinical data, including lymph node metastasis, Ki-67 expression, and hormone receptor status, were collected and analyzed among the three HER2 expression groups. Quantitative IVIM parameters were assessed, including the real diffusion coefficient (ADCslow), perfusion-related diffusion coefficient (ADCfast), and perfusion fraction (f). To compare differences, statistical analysis was conducted using the χ2 test for categorical data and independent sample t test for continuous data. A significance level of P ≤ 0.05 was applied for statistical significance determination.Furthermore, subgroup analyses were performed within the HER2 low expression group, distinguishing between HER2-low (IHC score 1+) and HER2-low (IHC score 2+) cases. Comparative assessments were made between these subgroups and HER2-zero cases.The study adhered to ethical guidelines, and informed consent was obtained from all participants. The research protocol received approval from the Institutional Review Board of our institution. Data analysis was conducted using statistical software, and the results were carefully interpreted to provide meaningful insights into the predictive capabilities of IVIM parameters for HER2 expression in breast cancer, facilitating personalized treatment planning and prognostic evaluation before surgical intervention.Result
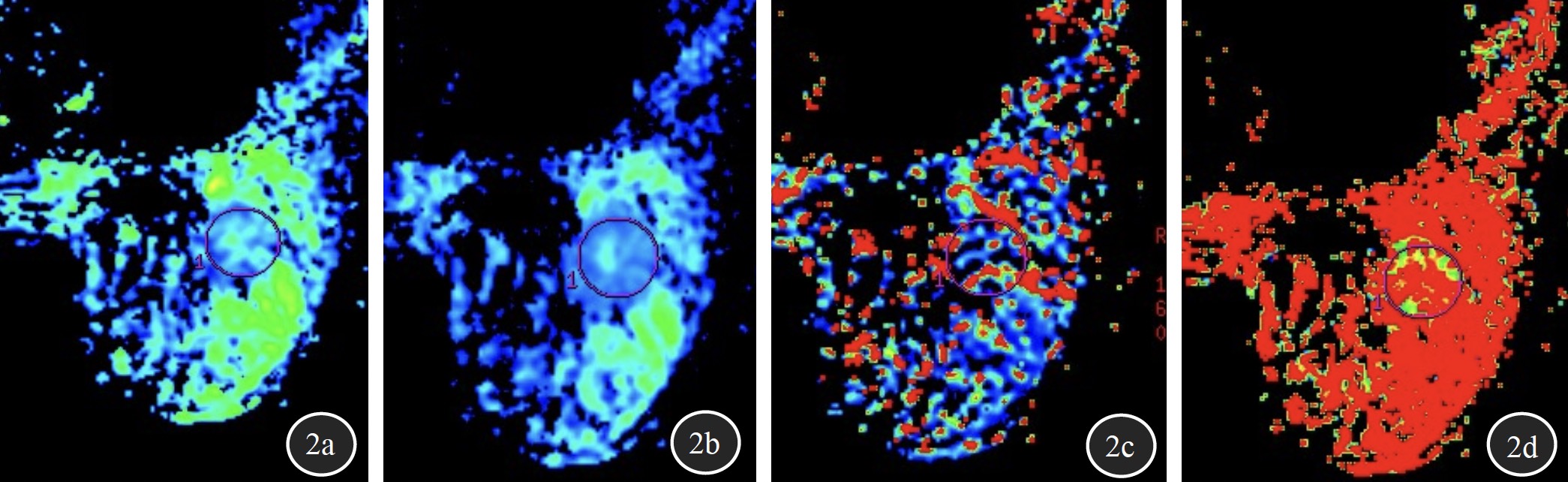
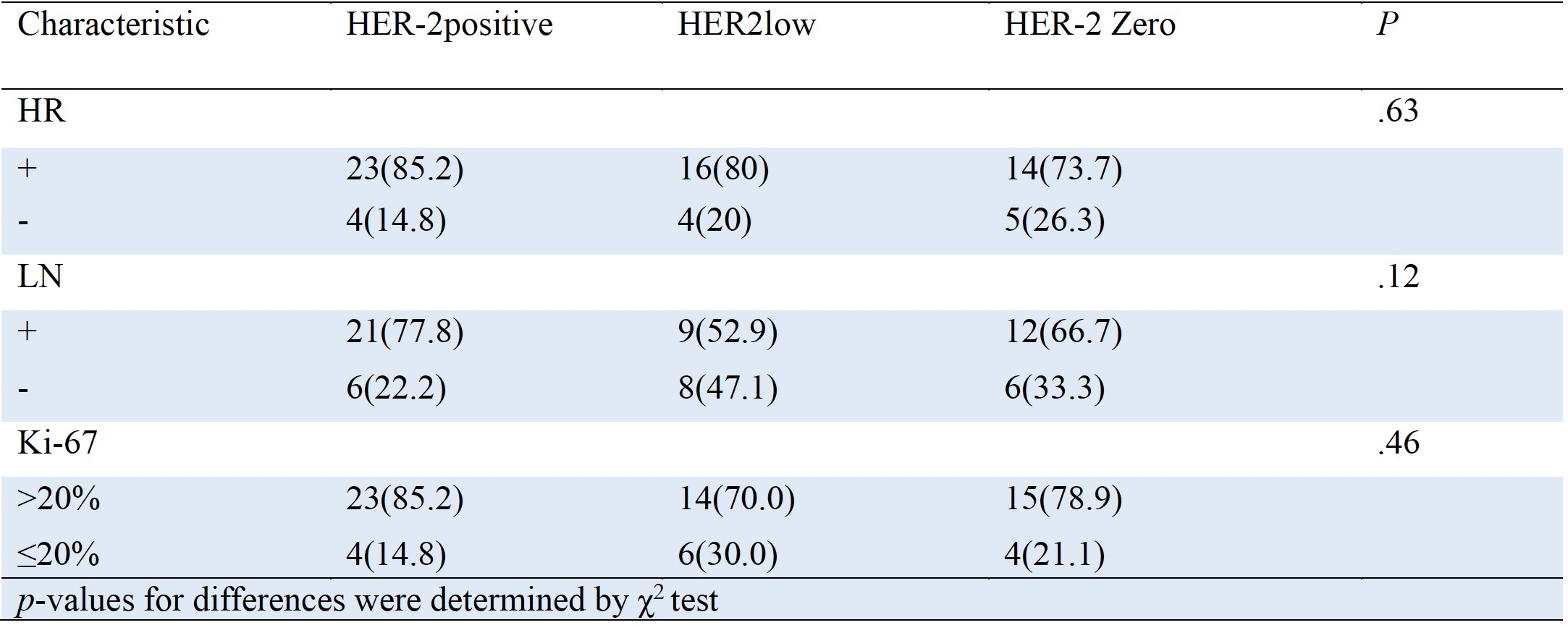
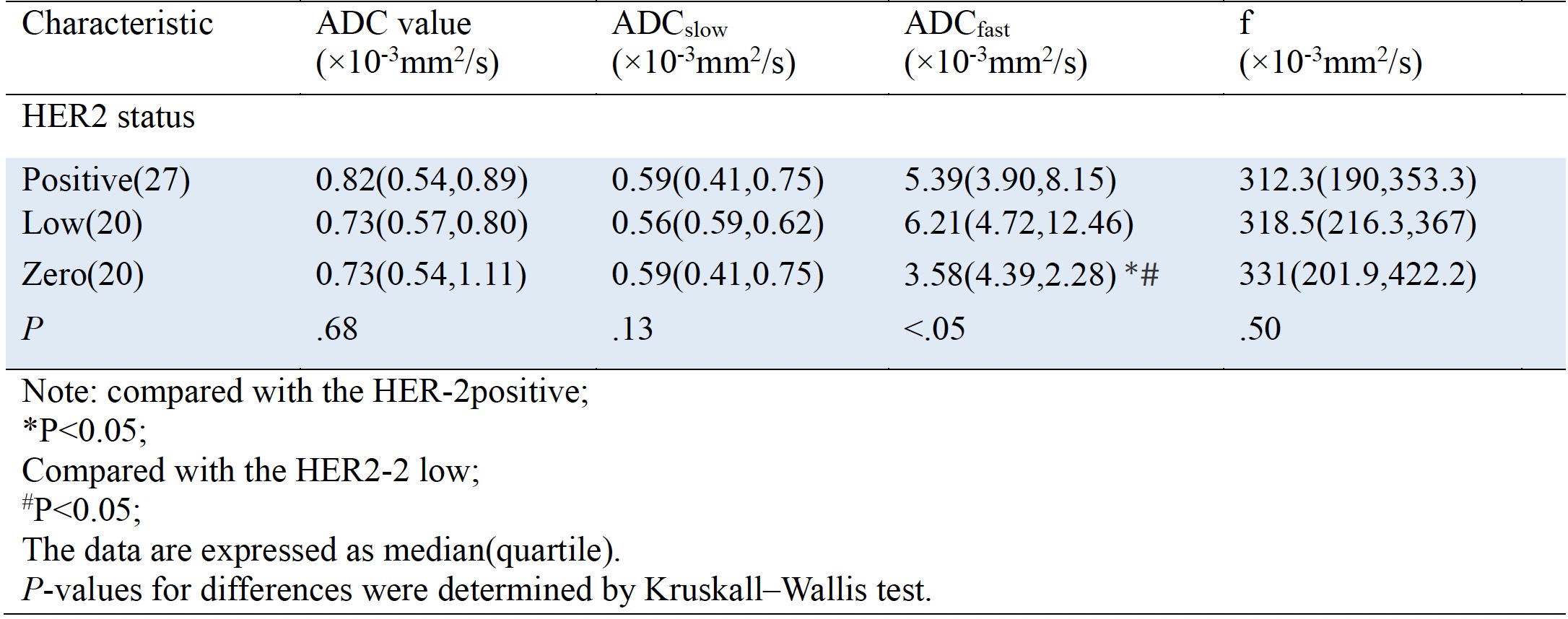
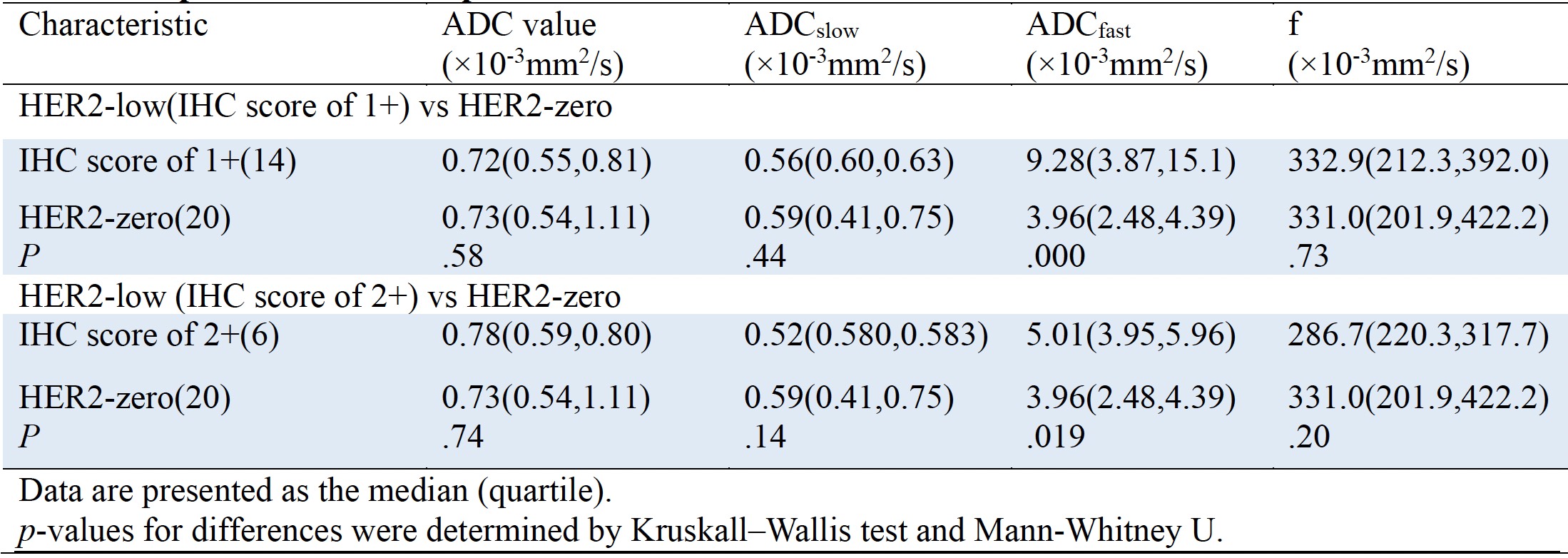
Our study findings revealed important insights into the relationship between HER2 expression and IVIM parameters in breast cancer. Notably, there were no significant differences observed among the three HER2 expression groups regarding lymph node metastasis, high expression of Ki-67, or negative hormone receptor (HR) expression(Table1). These results suggest that HER2 status does not necessarily correlate with these clinicopathological features. However, significant differences were observed in the ADCfast values between the HER2 positive group and HER2 low expression group compared to the HER2-zero group, indicating higher perfusion-related diffusion coefficients in the former two groups. Furthermore, within the HER2 low expression group, both HER2-low (IHC score of 1 +) and HER2-low (IHC score of 2+) subgroups exhibited higher ADCfast values than HER2-zero cases, with statistical significant (P<.05). This suggests that IVIM parameters, particularly ADCfast, may be indicative of HER2 expression status. In contrast, no significant differences was found in ADC, ADCslow, or f among the three HER-2 groups. Refer to Table2 for comprehensive datails. Additionally, there was no significant difference in these IVIM parameters when comparing HER2 positive and HER2 low expression groups to HER2-zero or when comparing HER2-low (IHC score of 1+) and HER2-low (IHC score of 2+) subgroups to HER2 (P>.05)(Table3). Refer to Figure 1 and 2 for patient selection process and ROI sketch.Discussion
In this study, we analyzed the diagnostic value of quantitative parameters of IVIM in breast cancer. The results indicated that ADCfast values were higher in HER2 positive group and HER2 low expression group compared to the HER2-zero group. Further subgroup analysis based on immunohistochemical criteria showed that HER2-low (IHC score of 1+) and HER2-low (IHC score of 2+) within the HER2 low expression group also had higher ADCfast values than HER2-zero group. This could be attributed to ADCfast reflecting microvascular perfusion, which may be related to HER2-associated overexpression of vascular endothelial growth factor, promoting immature neovascularization[2]. While previous studies reported lower ADCslow in HER2 positive compared to HER2-zero cases, this study did not observe a significant difference[3,4], possibly due to the small sample size and ROI variability. Furthermore, the study findings indicated that the ADC values cannot reliably predict HER2 expression , consistent with the previous research results[3-5]. Tumor cells with HER2 positive expression exhibit heterogeneous characteristics, restricting water molecule diffusion within tumor tissue, while the abundant blood supply in the tumor facilitates water molecules movement, resulting in varying ADC values[6].Conclusion
IVIM quantitative parameter ADCfast can noninvasively predict the HER2 expression in breast cancer before surgery, assisting in the development of individualized treatment plans and prognosis assessment for patients prior to surgery.Acknowledgements
All authors read and approved the final manuscript.References
1 de Nonneville A, Houvenaeghel G, Cohen M, et al. Pathological complete response rate and
disease-free survival after neoadjuvant chemotherapy in patients with HER2-low and HER2-0
breast cancers. Eur J Cancer. 2022;176:181-188
2 Kim JJ, Kim JY, Suh HB, et al. Characterization of breast cancer subtypes based on quantitative
assessment of intratumoral heterogeneity using dynamic contrast-enhanced and diffusion-weighted
magnetic resonance imaging. Eur Radiol. 2022; 32(2):822-33
3 Yu ZX, Liu JK, Zhou H, et al. Prediction of ImmunohistochemicaMarkers of Breast Cancer Based on
Intravoxel Incoherent Motion Diffusion Weighted Imaging and Dynamic Contrast Enhancement.
Chinese Journal of Medical Imaging. 2019; 27(7):522-526,528
4 Yang ZL, Shao K, Zhu LM, et al. Correlation between multiple paraments of mangnetic resonancer
imaging and HER-2 expression status of breast cancer. Radiol Practic. 2023; 38(8):1006-1012
5 Kim Y, Ko K, Kim D et al. Intravoxel incoherent motion diffusion-weighted MR imaging of breast
cancer: association with histopathological features and subtypes. Br J Radiol. 2016;
89(1063):20160140
6 Meng N, Wang X, Sun J, et al. A comparative study of the value of amide proton transfer-weighted
imaging and diffusion kurtosis imaging in the diagnosis and evaluation of breast cancer. Eur Radiol.
2021; 31(3):1707-17
Figures