5011
Ultrafast breast MRI for predicting lymph node metastases in breast cancers1The Fourth Affiliated Hospital of Hebei Medical University, Shijiazhuang, China, 2MR Research Collaboration, Siemens Healthineers Ltd, Beijing, China, 3MR Application Predevelopment, Siemens Healthineers AG, Erlangen, Germany
Synopsis
Keywords: Breast, Breast, breast tumor; dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI); Ultrafast Breast MRI
Motivation: Studies of ultrafast dynamic contrast-enhanced (DCE)-MRI were previously focused primarily on differentiating between benign and malignant breast tumors, with little research on lymph node metastases.
Goal(s): We searched for noninvasive biomarkers to predict lymph node metastases in patients with breast cancer using ultrafast DCE-MRI.
Approach: Ultrafast DCE-MRI was performed using a GRASP sequence, and the proprietary kinetic indicators were calculated to quantitatively diagnose lymph node metastases.
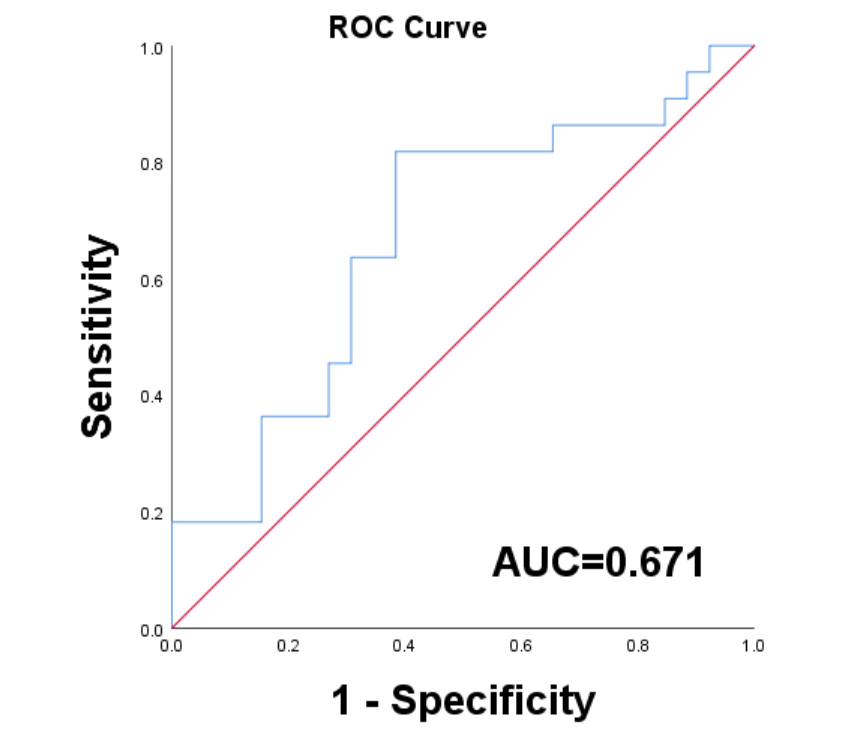
Results: The relative peak enhancement of patients with lymph node metastasis was significantly higher than that of those without metastasis (area under the curve: 0.671)
Impact: In this feasibility study, we preliminarily explored the role of ultrafast breast MRI in diagnosing lymph node metastasis in patients with infiltrating ductal carcinoma. We found that relative peak enhancement can be used to predict lymph node metastasis.
Introduction
The recently introduced golden-angle radial sparse parallel MRI (GRASP) technique balances the temporal resolution and spatial resolution of dynamic contrast-enhanced (DCE)-MRI to achieve multiphase dynamic continuous scanning with free breathing. Ultrafast DCE-MRI dynamics provide early kinetic information on breast lesions by collecting only the very early phase after administration of the contrast agent (approximately 1 minute). Ultrafast DCE-MRI greatly reduces the scanning time from that of conventional breast DCE-MRI, which requires collecting pre-contrast, initial, and delayed phase post-contrast images for fitting the time-signal intensity curve for Breast Imaging Reporting and Data System diagnosis1. Previously, ultrafast DCE-MRI studies focused primarily on differentiating benign from malignant breast tumors, with minimal research on lymph node metastases2. Axillary lymph node metastases are an important reference index for predicting the prognosis of patients with breast cancer. However, in current clinical practice, the evaluation criteria for sentinel lymph node biopsies in breast cancer are inefficient and often require invasive surgery, resulting in surgery-related complications3 in many patients. Therefore, we investigated the role of ultrafast DCE-MRI for diagnosing preoperative lymph node metastases in patients with breast cancer.Methods
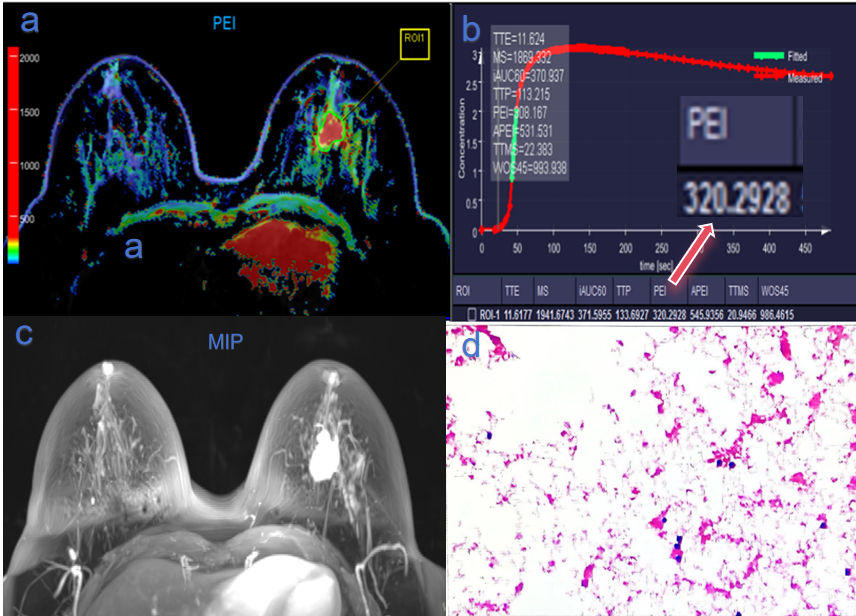
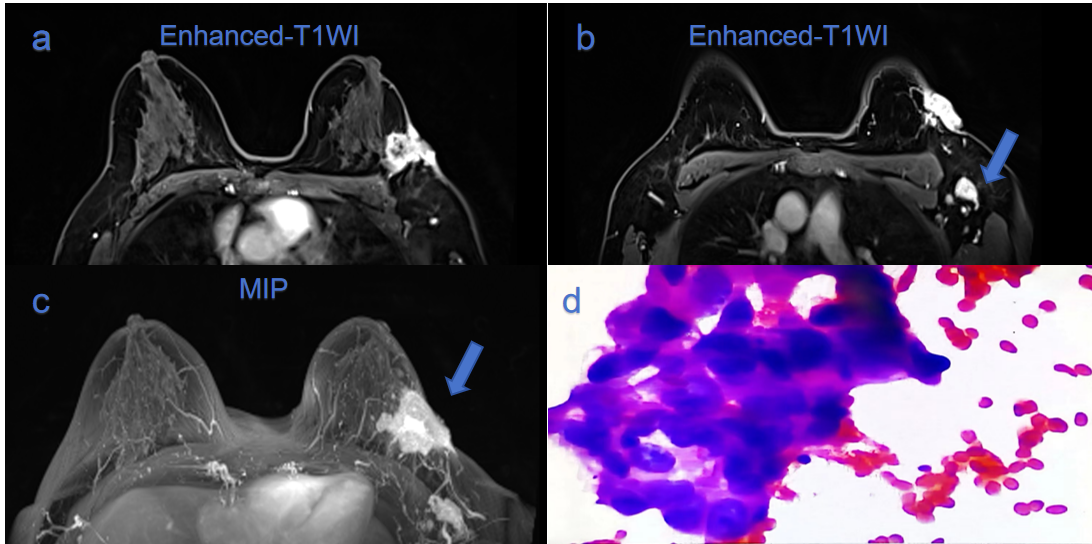
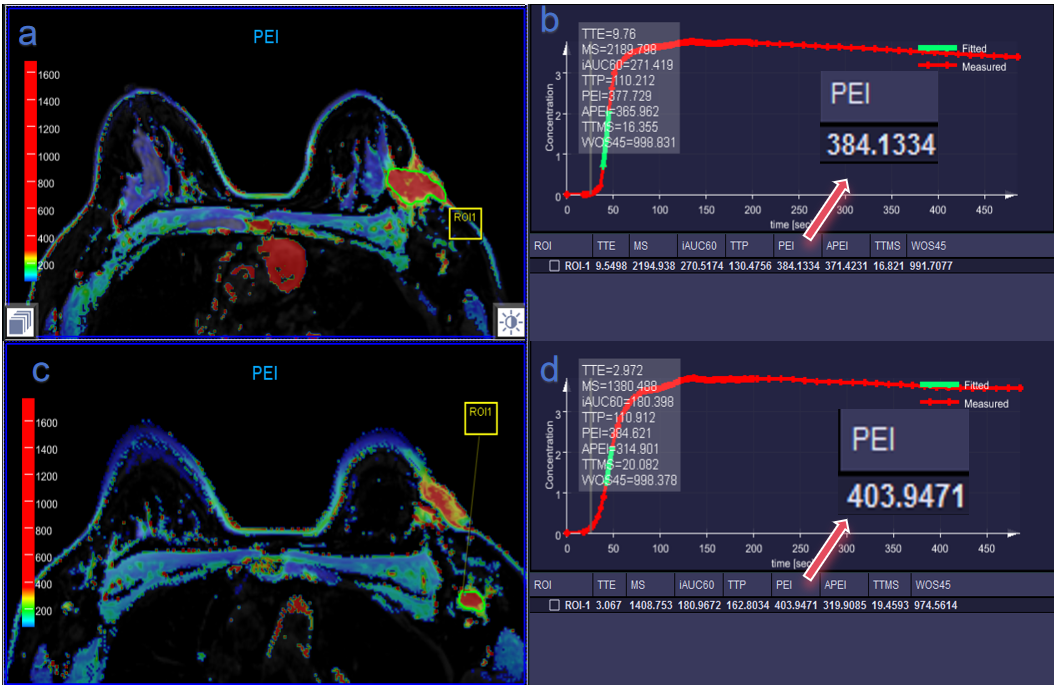
Forty-eight patients with surgically and pathologically confirmed invasive ductal carcinoma were enrolled, including 26 patients without lymph node metastasis and 22 with lymph node metastasis. All patients underwent breast MRI on a 3T MR scanner (MAGNETOM Vida, Siemens Healthineers, Erlangen, Germany). Contrast media (0.2 mmol/kg, Gadovist, Bayer) was injected at 3 mL/s, followed by a 10-mL saline chaser. T1 mapping was obtained using a T1-weighted volumetric interpolated breath-hold examination (VIBE) sequence before enhancement. Ultrafast DCE-MRI was acquired using a free-breathing GRASP sequence for 8 minutes and 25 seconds before and after enhancement. The scanning parameters were as follows: variable time resolution = 12.5 s for the first 20 s, then 3 s, and 12.5 s again for the last 300 s, field of view = 380 mm × 380 mm, matrix = 380 × 320, and voxel size = 1.2 mm × 1.2 mm × 2.5 mm. Time-to-enhancement (TTE), maximum slope (MS), area under the curve 60 sec after enhancement (iAUC60), time-to-peak after enhancement (TTP), relative peak enhancement (PEI), absolute peak enhancement (APEI), time to center of MS (TTMS), wash-out slope for 45 sec after peak or last 45 sec of scan (WOS45) were calculated using the “Breast” model of the research software (MR DCE, version 1.1.2, Siemens Healthineers, Erlangen, Germany). All parameters are expressed as means ± standard deviation. Inter-group differences were assessed with independent-sample t-tests using SPSS software (SPSS Inc., Chicago, IL, USA). P<0.05 was considered statistically significant.Results
The PEI differed significantly between patients with and without lymph node metastasis (P=0.037; Table 1, Figures 1–3)The AUC of the PEI was 0.671(Table 2, Figure 4), indicating that the PEI can predict lymph node metastasis. No other indicators were statistically significant (P>0.05).Discussion
In this preliminary study, we explored the feasibility of ultrafast breast MRI for diagnosing lymph node metastasis in infiltrating ductal carcinoma of the breast. Few studies have previously reported these results. We found that the PEI differed significantly between patients with and without metastasis. Previous literature suggested that invasive tumors have an abundance of new vascularization and increased immature vascular permeability4. In our study, the number of patients with lymph node metastasis was significantly higher than the number without metastasis, likely due to the richer neovascularization in patients with lymph node metastasis along with worsened basement membrane integrity in the microvessels and higher early relative enhancement values on the dynamic enhancement curve. Natsuko et al. reported that compared with patients with ductal carcinoma, patients with invasive carcinoma in situ exhibited a significantly larger MS and shorter bolus arrival time5. In our study, although the new parameters for ultrafast DCE-MRI, including MS and TTE, were increased in patients with metastasis, the differences were not statistically significant. Thus, these indicators may not be sufficiently sensitive for detecting metastasis. All enrolled patients had infiltrating ductal carcinoma; however, the total number of cases was relatively small. Further analysis of additional patients is warranted.Conclusion
The PEI index for ultrafast breast MRI has important implications for diagnosing lymph node metastasis in patients with breast cancer and provides a noninvasive reference tool for clinical diagnosis of lymph node metastasis.Acknowledgements
No acknowledgement found.References
1. Mann RM, Cho N, Moy L. Breast MRI: State of the Art. Radiology. 2019;292(3):520-536. doi:10.1148/radiol.2019182947. Epub 2019 Jul 30. PMID:31361209.
2. Mus RD, Borelli C, Bult P, et al. Time to enhancement derived from ultrafast breast MRI as a novel parameter to discriminate benign from malignant breast lesions. Eur J Radiol. 2017;89:90-6.
3. Yu Y, He Z, Ouyang J, et al. Magnetic resonance imaging radiomics predicts preoperative axillary lymph node metastasis to support surgical decisions and is associated with tumor microenvironment in invasive breast cancer: A machine learning, multicenter study. EBioMedicine. 2021;69:103460.
4. Mori N, Abe H, Mugikura S, et al. Ultrafast dynamic contrast-enhanced breast MRI: kinetic curve assessment using empirical mathematical model validated with histological microvessel density. Acad Radiol. 2018.
5. Onishi N, Sadinski M, Hughes MC, et al. Ultrafast dynamic contrast-enhanced breast MRI may generate prognostic imaging markers of breast cancer. Breast Cancer Res. 2020;22(1):58.
Figures
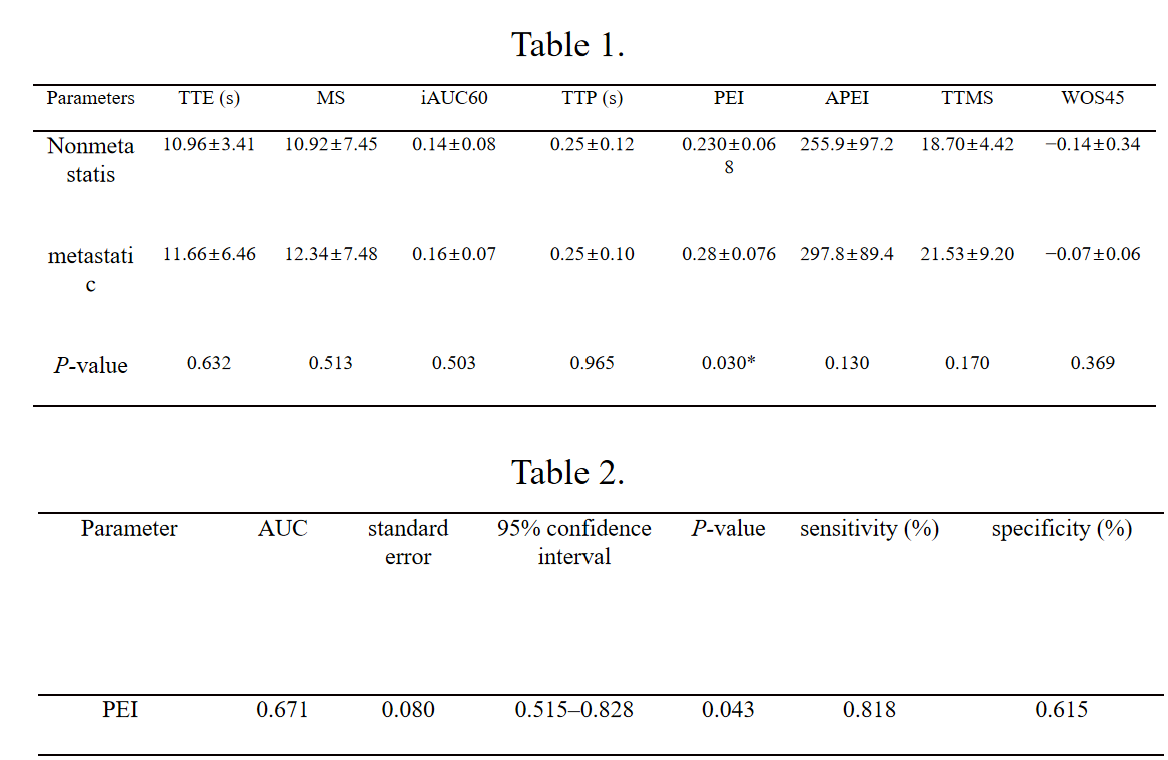
Table 1. Comparison of quantitative parameters of ultrafast DCE scan for malignant breast cancer with and without lymph node metastasis.
Note: Values are means ± standard deviation. *P<0.05, difference is statistically significant.
Table 2. Performance of PEI in finding lymph node metastasis in patients with breast cancer