5010
Deep Learning Based Rectal Tumor Localization and Segmentation on Multi-parametric MRI1Radiation Oncology, University of California, Irvine, CA, United States, 2Radiological Sciences, University of California, Irvine, CA, United States, 3Radiation Oncology, Sir Run Run Shaw Hospital, Zhejiang University School of Medicine, Hangzhou, China, 4Radiation Oncology, Rutgers-The State University of New Jersey, New Brunswick, NJ, United States
Synopsis
Keywords: Cancer, Cancer
Motivation: The study is motivated by need to improve rectal cancer treatment planning through deep-learning-based analysis of multiparametric MRI, replacing inconsistent and labor-intensive manual tumor delineation.
Goal(s): The study aims to develop a deep-learning algorithm for automated rectal cancer segmentation in MRI images to improve treatment response predictions.
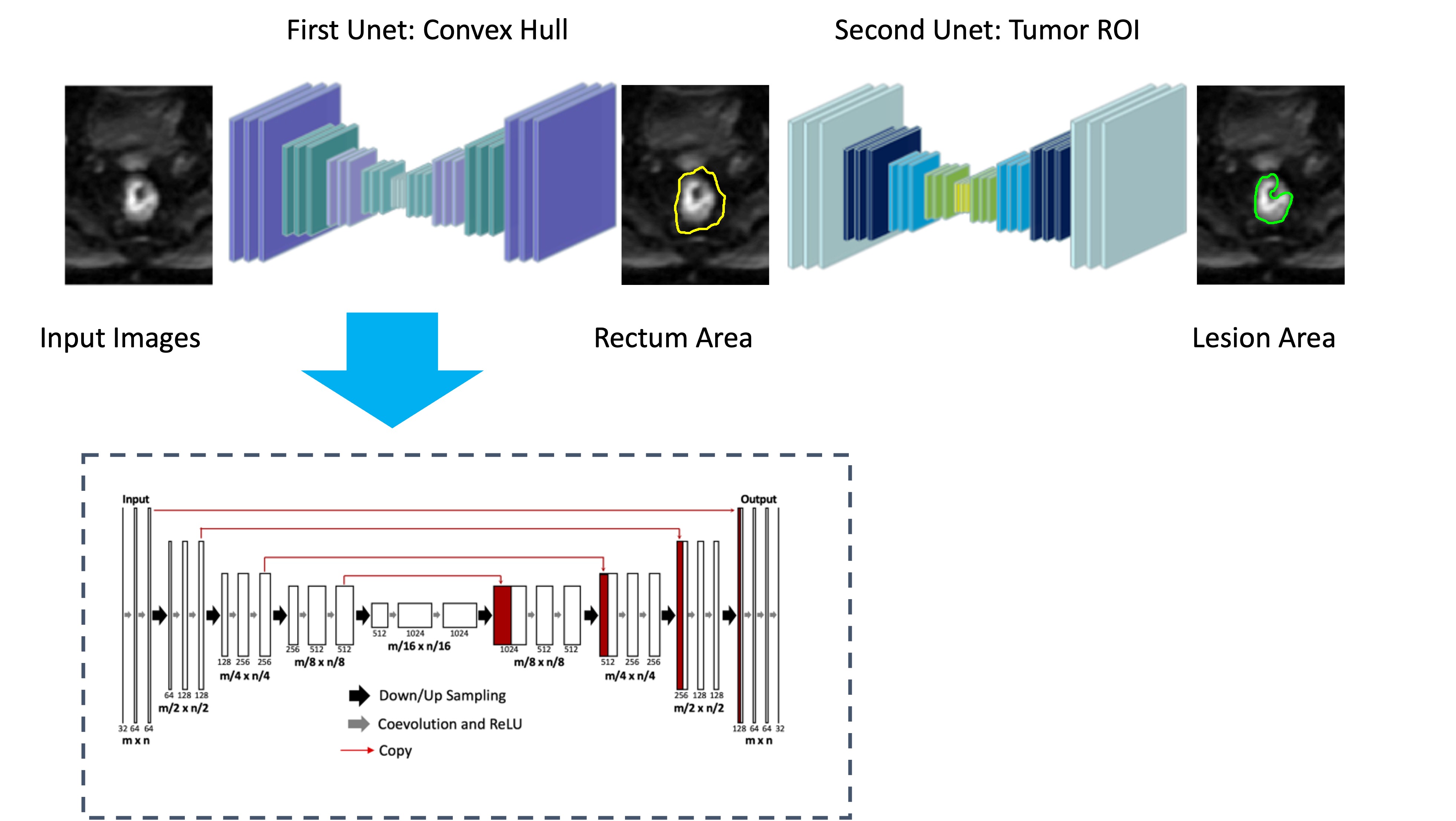
Approach: A two-tiered U-net architecture with attention gates, optimized through cross-validation, was applied to multi-parametric MRI data from 198 patients.
Results: This approach outperformed existing models, with the highest accuracy achieved by combining different MRI sequences. The results indicate that incorporating functional MRI data with anatomical imaging significantly enhances tumor delineation, potentially informing personalized treatment strategies.
Impact: This deep-learning model significantly improves rectal cancer MRI segmentation, offering a path to more accurate and personalized treatment strategies, potentially leading to better patient outcomes and streamlined workflows in oncological imaging and radiation therapy planning.
Introduction
The utilization of multiparametric Magnetic Resonance Imaging (mp-MRI) is pivotal for initial diagnosis and essential in the preoperative staging of rectal cancer. Radiomic data extracted from mp-MRI have been successfully utilized for early predictions regarding the response to treatment [1-4]. Nonetheless, the conventional approach of manual delineation of the region of interest (ROI) is both labor-intensive and susceptible to inter-reader variability. Hence, the development of an automated approach for tumor localization and segmentation is crucial for the construction of predictive models. Interest in deep learning models has surged, particularly in the context of medical image processing, including tasks like pulmonary nodule detection and segmentation. Nevertheless, rectal cancer segmentation presents unique challenges due to the variability in tumor location and morphology, as well as the mobility of adjacent tissues. Moreover, evidence from clinical trials suggests that dose escalation beyond the conventional 50.4 Gy is associated with a higher rate of complete response, albeit with acceptable toxicity levels. However, current algorithms, often predicated solely on pre-treatment diagnostic images, may not be versatile enough to discern boost target volumes on MRIs acquired towards the end of treatment. This study endeavors to develop a deep-learning algorithm that leverages pre-treatment mp-MRI data, aiming to discern which MRI sequences, or their combinations, are most efficacious for accurate rectal cancer delineation. Additionally, this research incorporates transfer learning models to bridge the gap from pre-treatment to near end-treatment images, potentially enabling escalated radiation dosing to enhance treatment outcomes.Methods
We gathered multi-parametric MRI data from 198 patients diagnosed with locally advanced rectal adenocarcinoma. These datasets included pre-treatment image sets, with 103 cases also having corresponding near end-treatment images. All imaging was performed on a 3.0 Tesla GE Signa HDxt scanner utilizing a phased-array body coil. The protocol incorporated T1-weighted (T1w), T2-weighted (T2w), dynamic contrast-enhanced (DCE-MRI) via a spoiled gradient echo sequence (LAVA), and diffusion-weighted imaging (DWI) with two b-values. An experienced rectal MRI radiologist outlined the ground-truth ROIs. Prior to analysis, we standardized the intensity across all images to a mean of zero and a standard deviation of one. We extracted image patches of 21x21 pixels, ensuring uniform position across all sequences for input into our models. A two-tiered U-net architecture was utilized, with each tier comprising 10 convolutional layers in both the descending and ascending phases. The convex hull of each lesion ROI was calculated, scaled up by 1.5 times, and used to train the initial U-net. The output from the first U-net informed the training of the subsequent U-net, which focused on predicting the lesion boundary. The primary U-net functioned as a localizer, indicating the probable sites of rectal tumors. Each image was then transformed into a corresponding probability map. After this model, we added attention gates (AG) at each layer on desceding phases which makes it as attend gated U-net (AG U-net)。 Our evaluation protocol involved: 1. Comparing our proposed algorithm U-net and AG-Unet to utilizing all pre-treatment sequences as input.2. Assessing the efficacy of using all available image sequences versus individual sequences to determine the most informative set for tumor delineation.3. Implementing transfer learning to adapt the pre-treatment model to near end-treatment data for boost volume identification. The training of these models was conducted via five-fold cross-validation. Hyperparameters such as learning rate, decay rate, and number of epochs were optimized based on the maximization of the objective function. After initial training with pre-treatment images, the models were fine-tuned with one-third of the near end-treatment data and validated against the remainder. We compared the performance of models trained on individual sequences (T2, DWI, LAVA) versus those trained on the entire sequence suite. To gauge the segmentation performance, we employed the DSC as metrics, comparing the proposed algorithm's output with the expert radiologist-defined ROIs.Results
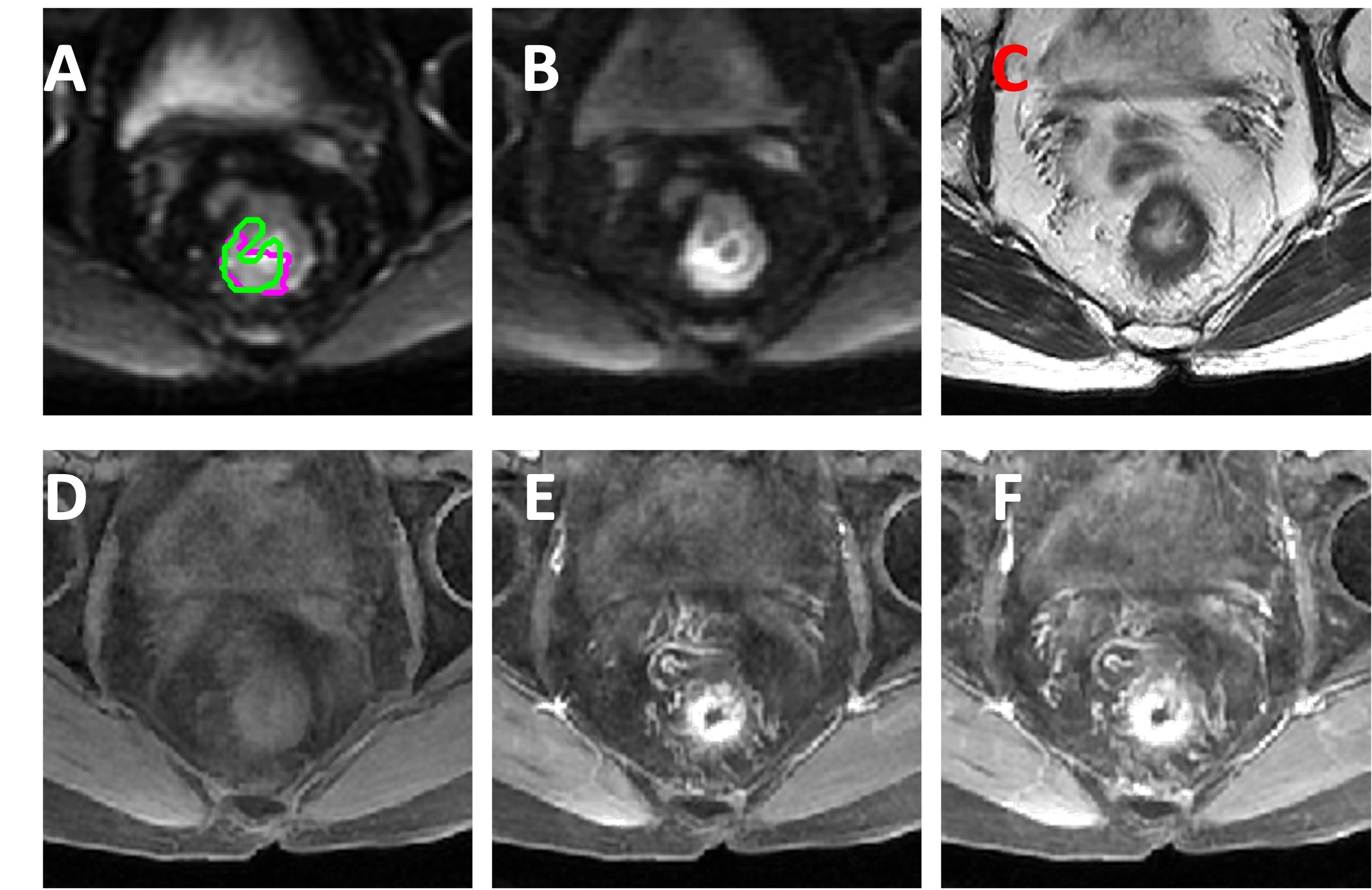
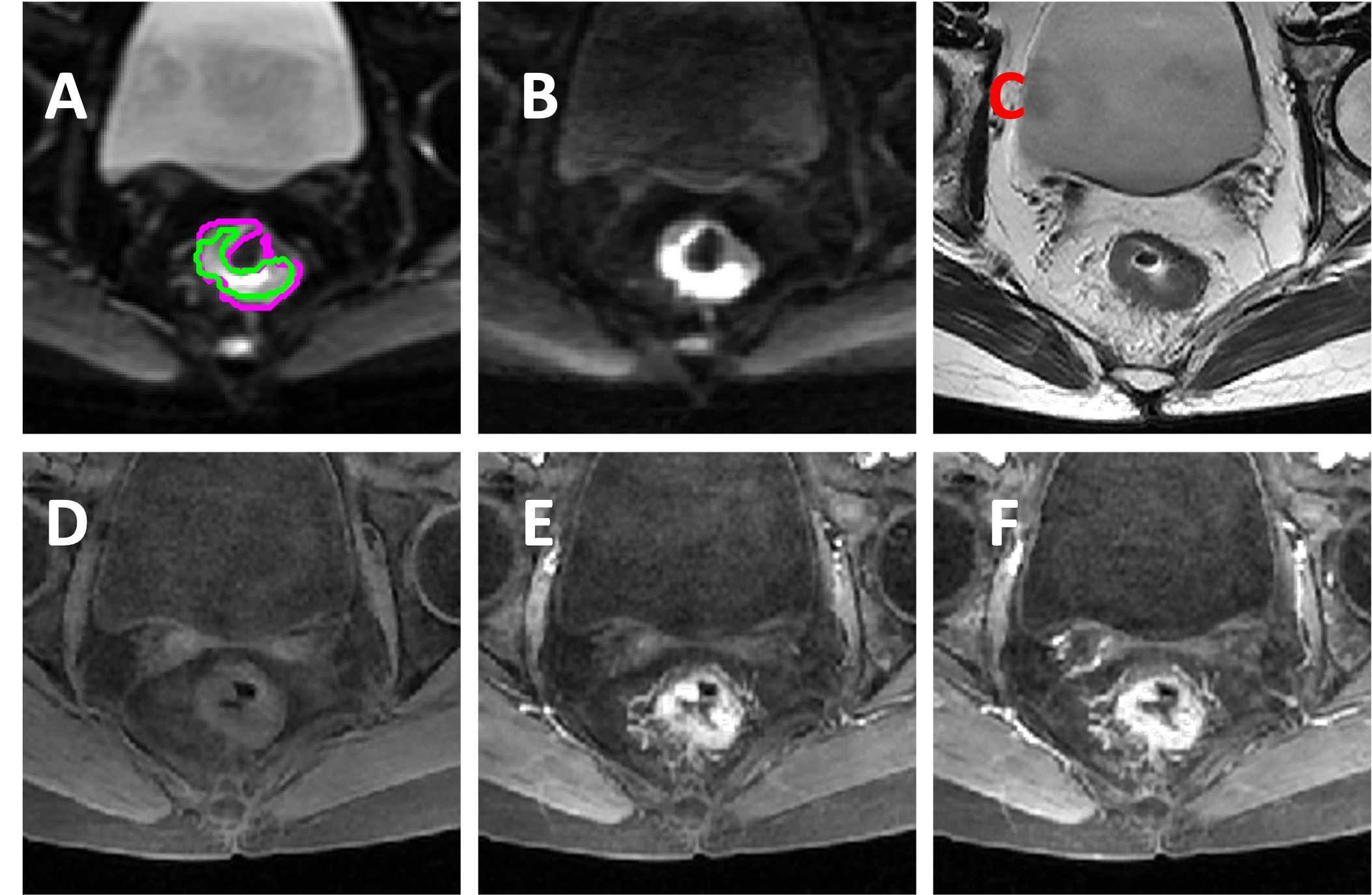
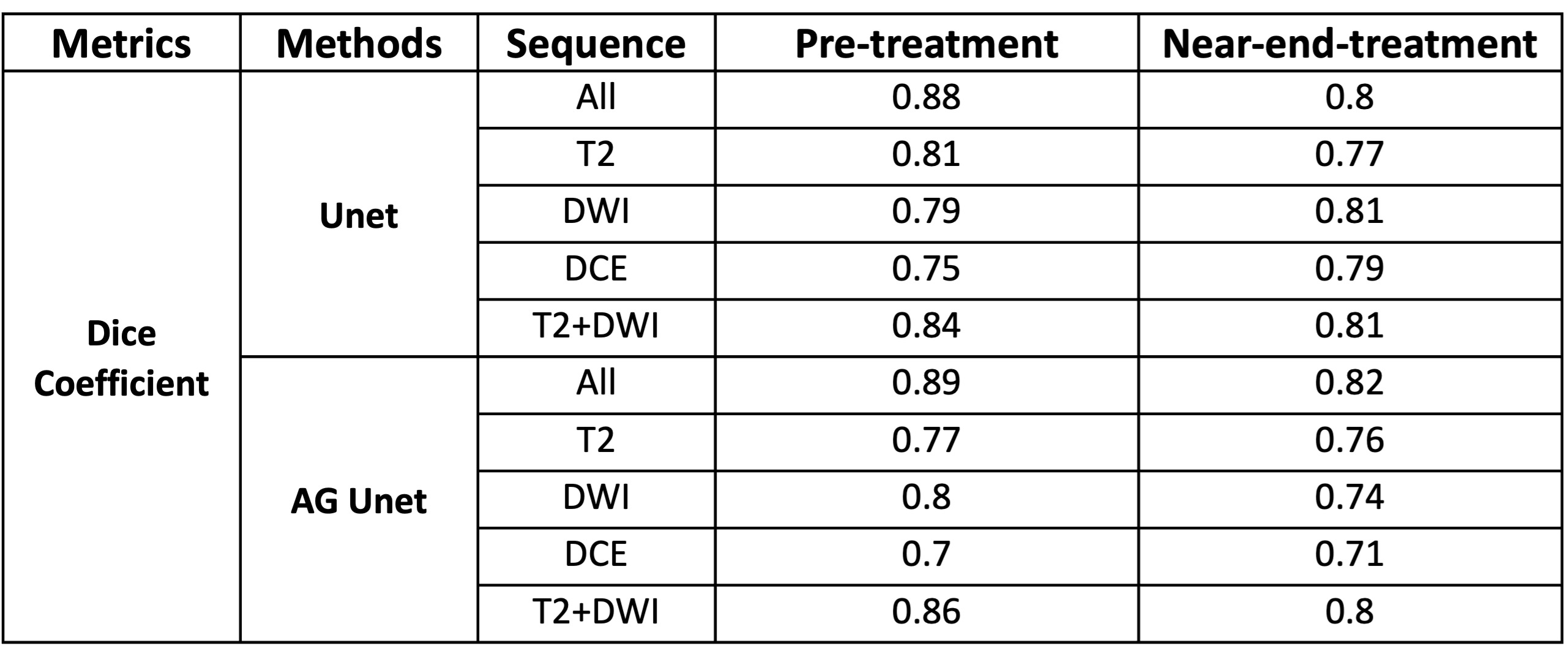
The developed AG U-net model achieved a mean DSC of 0.89, outperforming U-net algorithm, which recorded a DSC of 0.88. Utilizing solely T2w MRI data yielded a DSC of 0.77, which improved to 0.86 with the incorporation of functional DWI, and further to 0.89 upon adding DCE-MRI. However, using only DCE or DWI did not match the tumor delineation accuracy achieved with high-resolution T2w MRI. A decline in DSC to 0.82 was observed when applying the pre-treatment model directly to near end-treatment images. Nonetheless, fine-tuning the model with a combination of paired pre-treatment and near end-treatment images increased the DSC to 0.85. Detailed results are presented in Table 1, with illustrative examples in Figures 3-4.Discussion
The advent of efficient and reliable rectal tumor segmentation methods is a crucial advancement toward the quantitative extraction of imaging biomarkers and subsequent personalized treatment assessment. Although several deep learning models based on T2W images or DWI alone have been proposed [5-6], with barely acceptable DSC scores, our study tested two convolutional neural networks harnessing combined multi-parametric imaging sequences. The results underscore that our deep-learning approach, particularly the serial U-Net model, holds promise for fully automated and precise tumor segmentation. This marks a significant stride in reliably extracting both morphological and functional tumor data, thereby facilitating a deeper comprehension of individual tumor characteristics. Furthermore, our study is among the first to apply deep learning for the delineation of boost volumes using transfer learning, setting a precedent for the potential of personalized treatment stratification through radiation dose escalation.Acknowledgements
No acknowledgement found.References
[1] Kim YH, Kim DY, Kim TH, Jung KH, Chang HJ, Jeong SY, Sohn DK, Choi HS, Ahn JB, Kim DH, Lim SB. Usefulness of magnetic resonance volumetric evaluation in predicting response to preoperative concurrent chemoradiotherapy in patients with resectable rectal cancer. International Journal of Radiation Oncology* Biology* Physics. 2005 Jul 1;62(3):761-8.
[2] Seierstad T, Hole KH, Grøholt KK, Dueland S, Ree AH, Flatmark K, Redalen KR. MRI volumetry for prediction of tumour response to neoadjuvant chemotherapy followed by chemoradiotherapy in locally advanced rectal cancer. The British journal of radiology. 2015 May 28;88(1051):20150097.
[3] Nie K, Shi L, Chen Q, Hu X, Jabbour SK, Yue N, Niu T, Sun X. Rectal Cancer: Assessment of Neoadjuvant Chemoradiation Outcome based on Radiomics of Multiparametric MRI. Clin Cancer Res. 2016 Nov 1;22(21):5256-5264.
[4] Liu Z, Zhang XY, Shi YJ, Wang L, Zhu HT, Tang ZC, Wang S, Li XT, Tian J, Sun YS. Radiomics Analysis for Evaluation of Pathological Complete Response to Neoadjuvant Chemoradiotherapy in Locally Advanced Rectal Cancer. Clin Cancer Res. 2017 Sep 22. [Epub ahead of print]
[5] Trebeschi S, van Griethuysen JJ, Lambregts DM, Lahaye MJ, Parmer C, Bakers FC, Peters NH, Beets- Tan RG, Aerts HJ. Deep Learning for Fully-Automated Localization and Segmentation of Rectal Cancer on Multiparametric MR. Scientific Reports. 2017 Jul 13;7(1):5301.
[6] Kingma D, Ba J. Adam: A method for stochastic optimization. arXiv preprint arXiv:1412.6980. 2014 Dec 22.
Figures