4997
Advancing 3D DWI Imaging with the 3D Radial-EPI(RAZER) Trajectory1UCAIR, Department of Radiology and Imaging Sciences, University of Utah, Salt Lake City, UT, United States
Synopsis
Keywords: Pulse Sequence Design, Atherosclerosis, 3D DWI
Motivation: Non-Cartesian sampling offers advantages in motion robustness and speed, crucial in 3D DWI.
Goal(s): We aimed to improve 3D DWI using RAZER trajectory to improve the 3D DWI imaging with reducing scan time while preserving imaging quality.
Approach: We implemented 3D DW RAZER sequence with integrated radial and EPI sampling and conducted 3D DWI studies in a phantom and human carotid arteries.
Results: The RAZER DWI sequence offered a clearer depiction of the carotid arterial structure and reliable ADC measurements without geometric distortion when compared to 2D ss-DW EPI, all within a scan time of less than two minutes.
Impact: This study introduces a motion-robust 3D DWI with faster imaging capabilities, potentially improving vulnerable plaque identification. It addresses conventional DWI limitations, providing a valuable resource for the detection of possible events and improved patient outcomes in ischemic stroke.
PURPOSE
While conventional MRI commonly relies on Cartesian sampling, non-Cartesian approaches, such as radial1 or spiral sampling2, have gained recognition for their distinct advantages. These non-Cartesian acquisitions, particularly those that emphasize oversampling central region of k-space, exhibit inherent resilience to motion artifacts and the potential to generate high spatio-temporal resolution images from limited data3,4. To achieve greater flexibility, speed, and robustness against motion in 3D sampling, innovative hybrid trajectory techniques have been recently introduced5-8. The RAZER technique which combines the radial sampling in-plane with the Cartesian echo-train in partition direction offers the potential to decrease acquisition time, leading to improved sampling efficiency. By integrating the radial and Cartesian components, it becomes less sensitive to motion-related distortions during acquisition, making it suitable for multishot DWI. In this study, we have implemented diffusion preparation in conjunction with 3D RAZER sequence, aiming to address the challenges associated with motion artifacts in multishot DWI.METHODS
We integrated the radial sampling component for the in-plane (kx-ky) acquisition and Cartesian echo-train component for the partition (kz) direction into 3D segmented EPI. This sequence provides versatility to capture the entire kz space for each view angle either in a single acquisition or through segmented multi-shot approaches.All MRI studies were conducted using a 3T MRI scanner (Prisma, Siemens Healthineers) equipped with either 20-channel head coils or 8-channel dedicated carotid coils. This study was approved by the institutional review board and signed consent was obtained. We applied our 3D DW Radial-EPI sequences to both a cylindrical phantom filled with a uniform solution and featuring plastic structural inserts and the carotid arteries of a healthy subject. For comparative purposes, we also conducted a 2D single-shot (ss-) EPI sequence on the same phantom and subject. The 3D Radial-EPI acquisition parameters included TE/TR=8.2/75ms, voxel dimension=1x1x2 mm3, 302 radial views, and an ETL of 11, resulting in a scan time of 82 seconds for two b-values (10 and 450 sec/mm²). The imaging parameters for the 2D ss-EPI sequence were TE/TR=75/4500 ms, matrix size=160x160, the number of slices was 24, and the scan time was 44 seconds. We additionally conducted a scan on a subject with carotid disease.All reconstructions were performed offline using code written in MATLAB (MathWorks, Natick, MA) on a Linux workstation. The k-space data was gridded using a Kaiser-Bessel kernel and density compensated using a Voroni-based approach. Data from the multiple receive coils were reconstructed using an optimal coil combine utilizing the inverse covariance matrix derived from coil noise.9,10RESULTS
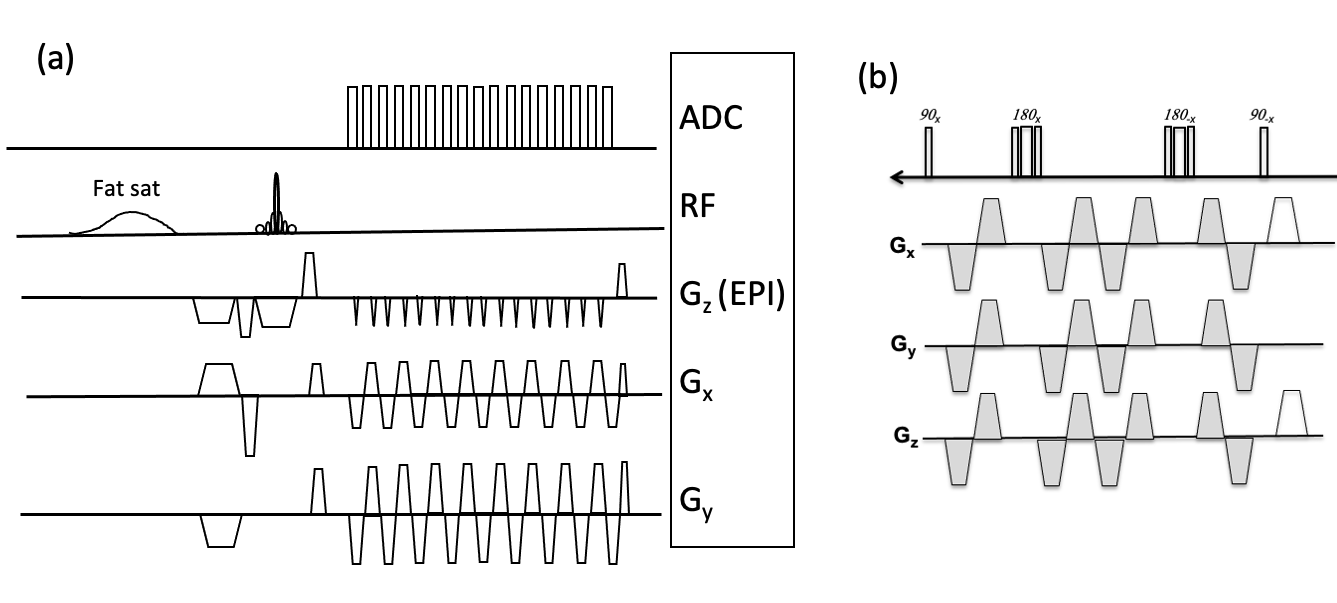
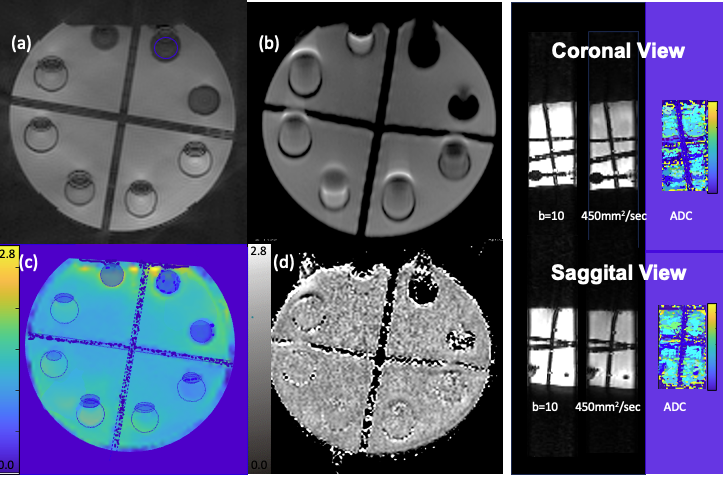
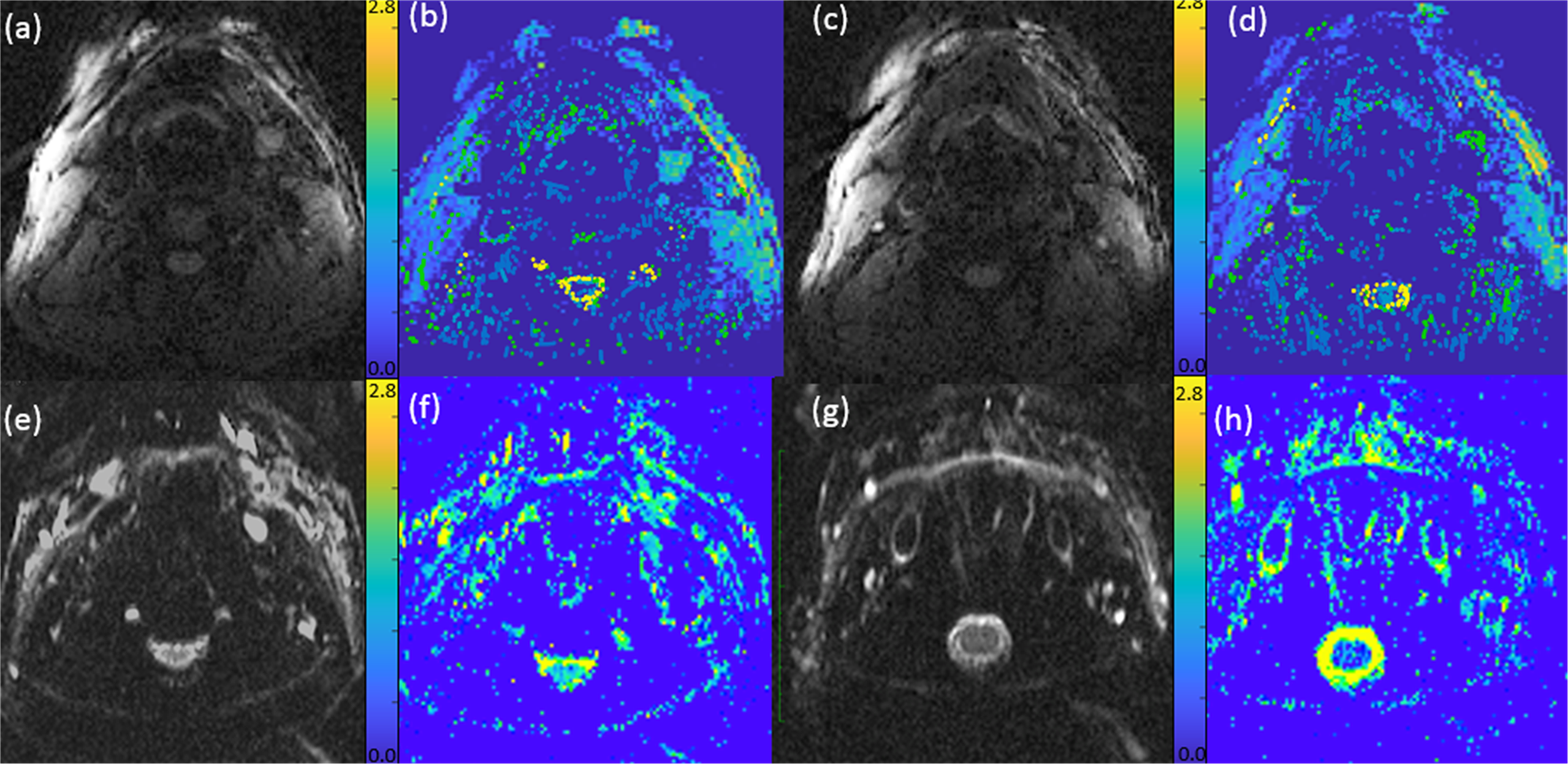
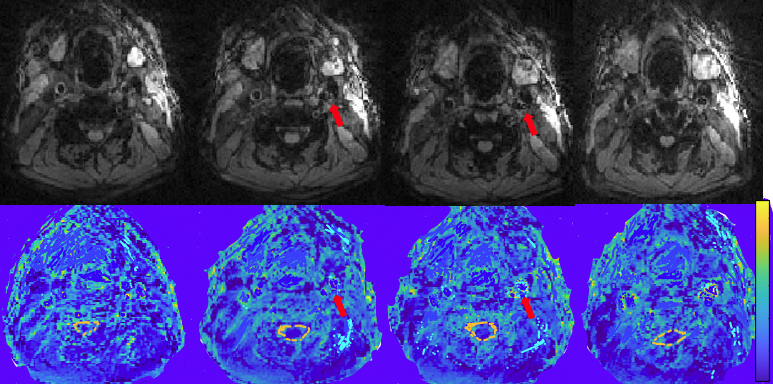
Figure 1 shows the sequence diagram of the RAZER. Figure 2 displays a representative DWI (b=10 sec/mm²) and the ADC of the phantom, acquired in a transverse acquisition plane. Additionally, coronal and sagittal plane images were presented. A comparison between the 3D RAZER trajectory and the 2D ss-EPI sequence reveals that RAZER trajectory delivers a clearer depiction of the internal structure of the phantom, free from the geometric distortion seen in the 2D ss-EPI acquisition. The mean ADC of the solution was 1.21±0.32 and 1.15±0.02 x10-3 mm2/sec from RAZER and 2D ss-EPI, respectively. Figure 3 displays carotid DWI and ADC maps at two distinct slice locations along carotid arteries, acquired using 3D Radial-EPI and 2D-ss EPI. Despite the higher SNR demonstrated by 2D ss-EPI DWI (e, g) and ADC maps (f, h), 3D Radial-EPI ADC maps (b, d) offer a superior depiction of arterial shape and other anatomical details without geometric distortion.The mean ADC of arterial wall was 1.43±0.62 and 1.38±0.18 x10-3mm2/sec from RAZER and 2D ss-EPI acquisition, respectively. Figure 4 presents 3D Radial-EPI carotid DWI and ADC maps obtained from the patient subject. The mean ADC of the plaque was 0.62 ±0.21 x10-3mm2/sec.DISCUSSION
The mean ADC derived from the RAZER sequence closely matched those obtained with 2D ss-EPI with a slightly higher standard deviation. The reduced SNR in RAZER contributes to the increased variability in ADC measurements. Nevertheless, the ability to acquire data for two b values within a two minute is a promising development that could facilitate the widespread adoption of the 3D DWI technique in clinical settings. To further increase both SNR and the precision of diffusion measurements, 3D radial-EPI can be implemented with signal averaging across multiple measurements, effectively reducing phase errors originating from motion discrepancies between different averages. We will improve this sequence to incorporate other view orderings, phase correction of the EPI readouts8, and gradient delay adjustment11 .CONCLUSION
RAZER DWI enhances neurovascular disease imaging, addressing limitations and improving patient outcomes, particularly in ischemic stroke and vulnerable plaque identification.Acknowledgements
Supported by funds from Huntsman endowed chair, S10 for Prisma.References
1. Glover GH, Pauly JM. Projection reconstruction techniques for reduction of motion effects in MRI. Magn Reson Med. 1992;28(2):275-289.
2. Liao JR, Pauly JM, Brosnan TJ, Pelc NJ. Reduction of motion artifacts in cine MRI using variable-density spiral trajectories. Magn Reson Med. 1997;37(4):569-575.
3. Vigen KK, Peters DC, Grist TM, Block WF, Mistretta CA. Undersampled projection-reconstruction imaging for time-resolved contrast-enhanced imaging. Magn Reson Med. 2000;43(2):170-176.
4. Sarty GE, Bennett R, Cox RW. Direct reconstruction of non-Cartesian k-space data using a nonuniform fast Fourier transform. Magn Reson Med. 2001;45(5):908-915.
5. Kim SE, Parker DL, Roberts JA, et al. Differentiation of symptomatic and asymptomatic carotid intraplaque hemorrhage using 3D high-resolution diffusion-weighted stack of stars imaging. NMR Biomed. 2021;34(11).
6. Seo N, Park SJ, Kim B, et al. Feasibility of free-breathing dynamic contrast-enhanced MRI of the abdomen: a comparison between CAIPIRINHA-VIBE, Radial-VIBE with KWIC reconstruction and conventional VIBE. Br J Radiol. 2016;89(1066).
7. Jeong HJ, Eddleman CS, Shah S, et al. Accelerating time-resolved MRA with multiecho acquisition. Magn Reson Med. 2010;63(6):1520-1528.
8. Graedel NN, McNab JA, Chiew M, Miller KL. Motion correction for functional MRI with three-dimensional hybrid radial-Cartesian EPI. Magn Reson Med. 2017;78(2):527-540.
9. Roemer PB, Edelstein WA, Hayes CE, Souza SP, Mueller OM. The NMR phased array. Magn Reson Med. 1990;16(2):192-225.
10. Parker DL, Payne A, Todd N, Hadley JR. Phase reconstruction from multiple coil data using a virtual reference coil. Magn Reson Med. 2014;72(2):563-569.
11. Johnson KM. Hybrid radial-cones trajectory for accelerated MRI. Magn Reson Med. 2017;77(3):1068-1081.
Figures