4978
Fontan Patients Exhibit Altered CBF and ATT Measurements in Gray and White Matter: an ASL Study.1Cardiology, Children's Hospital Los Angeles, Los Angeles, CA, United States, 2Ming Hsieh Department of Electrical and Computer Engineering, University of Southern California Viterbi School of Engineering, Los Angeles, CA, United States, 3Department of Biomedical Engineering, University of Southern California, Los Angeles, CA, United States, 4Institute of Imaging Science, Vanderbilt University, Nashville, TN, United States, 5Department of Radiology and Nuclear Medicine, Amsterdam UMC, Amsterdam, Netherlands, 6Pediatric Neurosurgery, Children's Hospital Los Angeles, Los Angeles, CA, United States, 7Pediatrics CHLA, Keck School of Medicine of USC, Los Angeles, CA, United States
Synopsis
Keywords: Blood Vessels, Arterial spin labelling, Fontan, CBF, ATT, Oxygen Delivery
Motivation: Patients with Fontan palliation of single ventricular heart disease have significant cognitive deficits that may result from their chronically low cardiac output.
Goal(s): To determine whether global and regional brain oxygen delivery is normal in young adults after Fontan palliation.
Approach: We measured cerebral blood flow (CBF) and arterial transit time (ATT) in 28 young adult Fontan patients and 31 age and sex matched control subjects using pseudocontinuous time-encoded arterial spin labeling (PCASL).
Results: CBF and arterial transit time were increased, in Fontan subjects compared with controls. Oxygen delivery was decreased in the anterior and middle cerebral artery distribution.
Impact: These data suggest that physiologic compensation to the low cardiac output state produced by Fontan circulation is insufficient to maintain cerebral oxygen delivery. Time-encoded PCASL potential provides an important biomarker to judge surgical and medical interventions in these patients.
Introduction
The Fontan palliation surgery is the last of a series of three surgeries needed to correct underdeveloped, missing, or malfunctioning ventricles in patients with single ventricular heart disease (SVHD)1,2. Although the procedure intends to restore fully oxygenated blood flow to the brain, post-Fontan SVHD patients commonly develop white matter injury and related neurocognitive deficits3,4. In this work, we used arterial spin labeling (ASL) to measure cerebral blood flow (CBF), arterial transit time (ATT), and cerebral oxygen delivery (O2Del) to investigate cerebral physiology in Fontan patients compared to controls.Methods
Participants: 28 Fontan patients (FP, age=19.9±1.9 y; Hb=15.4±2.2; Hct=47.2±4.9; F=10) and 31 control subjects (CTL, age=22.6±4.2 y; Hb=14.0±1.4; Hct=42.4±3.9; F=15).Neuroimaging data: MRI data were acquired on a 3T Philips Achieva using a 32-channel head coil at Children’s Hospital Los Angeles. 3D T1-w: TR/TE=8.3/3.8 ms with isotropic voxel size (VS) of 1 mm3. 2D Echo Planar Imaging Time-encoded pCASL: TR/TE = 5040/16 ms, Hadamard-8 matrix with seven blocks, PLD=100 ms, SENSE=2.5, VS=3×3×6 mm3, 2 FOCI background suppression pulses, SPIR fat suppression, NSA=12. The ASL imaging volume was placed parallel to the AC-PC line, and the labeling plane was positioned 9 cm below imaging plane center to avoiding labeling at siphons. M0 scans: acquired using the same imaging parameters as pCASL with a TR= 2500 ms, with labeling and background suppression switched off.
MRI modeling: T1-w cortical surface delineation, registration, and parcellation to the BCI-DNI anatomical atlas was performed using BrainSuite (http://brainsuite.org/). Anatomical segmentations (designated ROIs, white/gray matter maps) were transformed to ASL native space, along with the arterial territory atlas5. ASL scans were motion corrected using SPM12, followed by subtraction according to the Hadamard-8 matrix to obtain seven perfusion weighted images (PWI; corresponding to PLDs of 100, 250, 450, 700, 1000, 1500 and 2300ms). Quantification of the seven PWIs was performed using the FSL based BASIL toolbox which uses Bayesian inference to fit CBF and ATT maps6. Oxygen delivery to the brain was calculated as a product of CBF and oxygen content, using hemoglobin values measured by phlebotomy7.
Statistical analysis: Global CBF, ATT and O2Del were calculated in white and gray matter (only) voxels (removing the partial-volume effects). Additional quantification of CBF and ATT was performed within bilateral territories of the main cerebral arteries (ACA, MCA, PCA).
Results
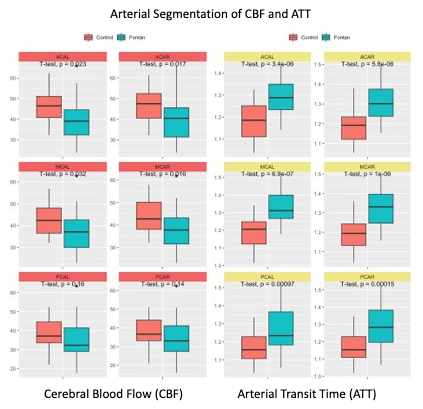
Global grey matter CBF was significantly lower in Fontan patients compared to healthy controls. A similar (albeit not statistically significant) trend was observed for global CBF in white matter as well as the total oxygen delivery to both regions, Fig.1. CBF (Fig. 2) and O2Del (not shown) were significantly decreased in ACA and MCA territories in patients compared to healthy individuals, Fig. 2. Data in PCA territory followed the same trend, although the difference did not achieve statistical significance.Fontan patients demonstrated significantly increased global ATT in both gray and white matter, Fig. 1, as well as within individually examined arterial territories (ACA, MCA, and PCA), Fig. 2.
Discussion
Fontan palliation in SVHD improves cyanosis, but creates by necessity a circulatory physiology similar to right heart failure. The absence of a pulmonary pump limits flow of blood through the lungs, reducing cardiac output. Cerebral venous drainage is affected by back pressure from pulmonary vascular resistance, with expected effects on cerebral nutrient delivery, as well as clearance of metabolic waste byproducts. The body partially compensates for low cardiac output by raising hemoglobin levels and by selective cerebral vasodilation (“brain sparing”), although limited data is currently available regarding the impact of these changes on normalizing cerebral oxygen delivery.The current work suggests that cerebral circulation remains hindered in Fontan patients, with significantly decreased flow and prolonged arterial transit time. We observed similar CBF/ATT behavior in both white and grey matter, across individual vascular territories. Oxygen delivery was significantly lower in anterior and middle cerebral artery territories in Fontan patients, with a similar but non-significant trend in the posterior circulation. Further assessment of oxygen extraction will be necessary to fully interpret the oxygen delivery results.
Conclusion
Cerebral blood flow is decreased and arterial transit time increased in young adults with single ventricular heart disease palliated by the Fontan procedure. Ongoing work will examine regional blood flow in relation to cognitive function, brain morphometry, white matter integrity, and functional connectivity.Acknowledgements
This work was supported by Additional Ventures Single Ventricular Fund, the National Heart Lung and Blood Institute (1RO1HL136484-A1), and the National Center for Research Resources (UL1 TR001855-02) of the National Institutes of Health. Philips Healthcare provided support for protocol development and applications engineering on a support-in-kind basis.References
1. Feinstein J, Benson D, et al. Hypoplastic left heart syndrome: current considerations and expectations. J. Am. Coll Cardiol. 2012; 59.
2. Fruitman D. Hypoplastic left heart syndrome: Prognosis and management options. Paediatr Child Health. 2000; 5(4): 219-25.
3. Marelli A, Miller S, et al. Brain in Congenital Heart Disease Across the Lifespan: The Cumulative Burden of Injury. Circulation. 2016; 133(20): 1951-62.
4. Verrall C, Blue G, Loughran-Fowlds A, et al. 'Big issues' in neurodevelopment for children and adults with congenital heart disease. Open Heart. 2019; 6(2).
5. Liu C, Hsu J, et al. Digital 3D Brain MRI Arterial Territories Atlas. Sci Data. 2023; 10(1): 74.
6. Chappell M, MacIntosh B, et al. Separation of macrovascular signal in multi-inversion time arterial spin labelling MRI. Magn Reson Med. 2010; 63(5): 1357-65.
7. Afzali-Hashemi L, Baas K, et al. Impairment of Cerebrovascular Hemodynamics in Patients With Severe and Milder Forms of Sickle Cell Disease. Front Physiol. 2021;12.
Figures