4939
Predicting antiseizure medication treatment outcome using AI and Structural MRI1Neuroscience, Monash University, Melbourne, Australia
Synopsis
Keywords: MR-Guided Interventions, Machine Learning/Artificial Intelligence, drug outcome estimation, seizure freedom
Motivation: Implementation of AI-driven precision medicine and finding the most effective Antiseizure Medications.
Goal(s): To predict outcomes of drug interventions in epilepsy patients and categorize them into distinct seizure outcome groups.
Approach: The research employs both patient characteristic, clinical, and MRI features going throguh a feature selection step followed by binary classification using Support Vector Machine, Naïve Bayes, Decision Tree, and Ridge Regression.
Results: Ridge regression combined with genetic algorithm outperformed the others, achieving an accuracy of 0.77 and AUC (Area Under the Curve) of 0.80 in predicting seizure outcome. This success was attained using a total of 18 MRI features and 10 ASMs.
Impact: Our model may help selection of the most effective ASM for individual patients. This may reduce the need for consecutive drug trials involving ineffective medications, thereby alleviating associated burdens.
Introduction
Seizure-controlling medications, known as anti-seizure medications (ASMs), typically achieve a success (defined as no seizure for 12 months or more) rate of around 60%. ASMs are the first-line treatment for most individuals diagnosed with epilepsy [1]. However, for an additional 15%, it may take anywhere from 2 to 5 years to discover an ASM regimen that effectively manages their seizures [2]. This represents an unmet medical requirement in determining the most suitable ASM that balances seizure control and patient tolerability. A more precise method to predict the response to ASMs is crucial in selecting the most appropriate medication when therapy begins for each patient. There is an anticipation that machine learning could unveil correlations between treatment outcomes and MRI data of patients [3].Methods
Initial ASM therapy was administered to 79 patients with newly diagnosed epilepsy following standard clinical procedures including Valproic acid, Oxcarbazepine, Levetiracetam, Lamotrigine, Carbamazepine, Zonisamide, Topiramate, Perampanel, Lacosamide, and Brivaracetam [4]. Each patient was assigned a specific duration for the initial regimen. If the first treatment proved ineffective, the second ASM would be included. This study involved the construction of machine learning algorithms to classify treatment outcomes into success or failure by using a binary vector that encapsulated the prescription of 10 specific ASMs for each individual. Success was defined as no seizure while taking the prescribed ASM at 12 months. All patients underwent baseline structural T1 weighted images to extract subcortical volumes, cortical gray matter volume, surface data, and thickness across different brain lobes. These extracted features were then combined with binary vectors representing all ten ASMs, along with characteristics obtained from the investigation conducted by Hakeem et al [5]. In total, 113 input data were prepared, each encompassing 315 features along with their respective outcomes. These data sets were further subjected to feature selection and classification processes. Initially, each feature in the dataset, excluding the drug-related variables, underwent normalization to achieve a consistent scale with zero mean and unit variance. For the feature selection process, two methods were employed: Step-wise Multiple Linear Regression (SMLR) and Genetic Algorithm (GA). In SMLR, the initial filtering phase eliminated features that exhibited a significant linear relationship (p-value<0.05) with the outcome. Following this, a backward sequential feature ranking approach was implemented to exclude features that displayed a high correlation with other variables. The GA approach involved generating a population of potential solutions, assessing their fitness using an objective function or heuristic, selecting "parents," reproducing via natural genetic operators, and ultimately returning the best solution as the optimal set of features for the machine learning model. Then, we applied various machine learning techniques including support vector machines (SVM), decision trees (DT), ridge regression (RR), and naïve Bayes (NB). To ensure the robustness of our models and reduce the influence of random variability, we conducted 50 iterations of 5-fold cross-validation. For model evaluation, we employed two key metrics: accuracy and Area Under the Curve (AUC).Result
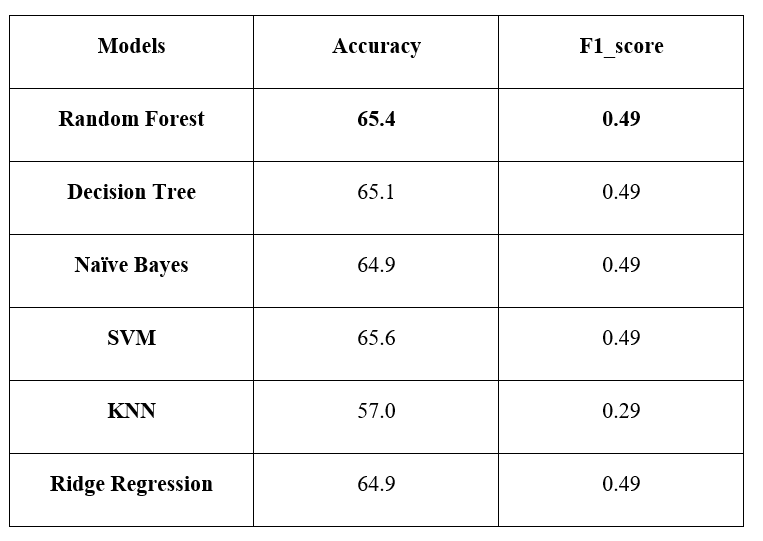
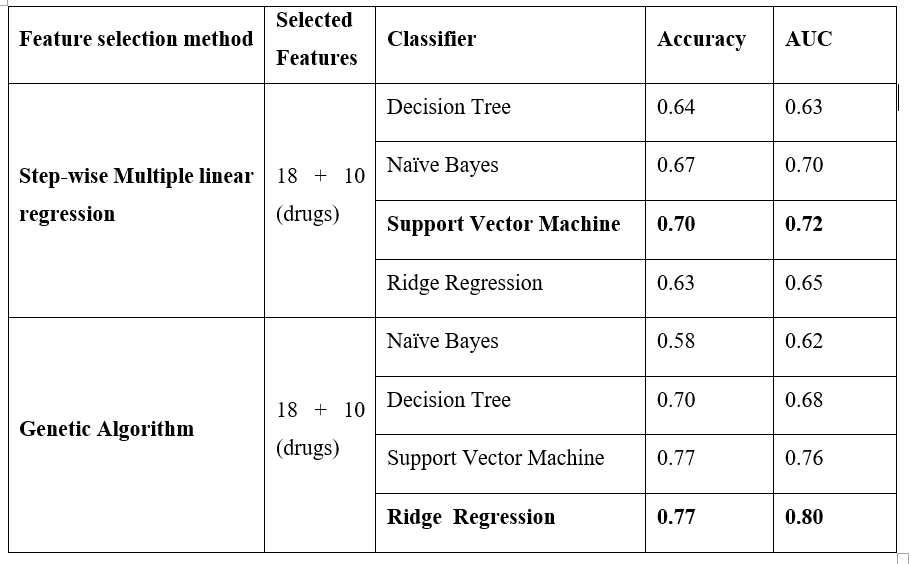
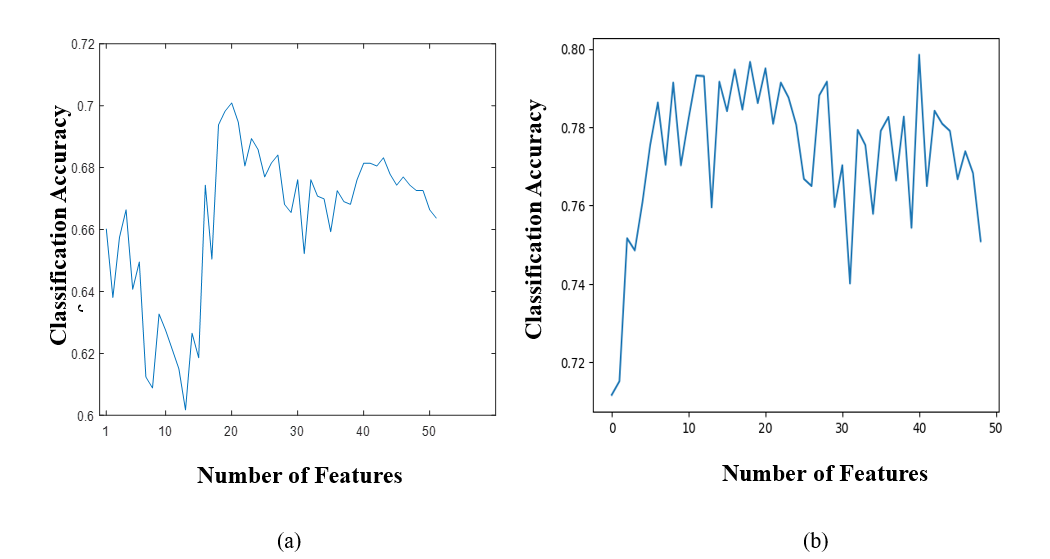
The RF classifier exhibited superior performance in classifying outcomes when exclusively considering ASMs. Using an optimal selection comprising eighteen features by SMLR, the SVM outperformed models based solely on drugs, achieving an accuracy of 0.70 and an AUC of 0.72. While GA applied to characteristics and MRI-extracted data identified the most effective features, when combined with ASM ones, the RR classifier outperformed all other methods achieving an accuracy of 0.77 and an AUC of 0.80.Discussion
Artificial intelligence has seen increased application in forecasting epilepsy treatment responses. A prior study employed both conventional machine learning techniques and newer transformer models to anticipate outcomes based on initial regimen and patient characteristics [5]. In a related study, a SVM classifier exhibited a high accuracy of 72% and an AUC of 0.96, successfully predicting seizure freedom for patients treated with levetiracetam monotherapy [1]. In this study, we utilized multiple machine-learning models to predict the clinical responses of epilepsy patients to ASMs. Comparatively, models integrating patient characteristics and MRI-derived features outperformed models reliant solely on ASM data. Notably, the inclusion of MRI characteristics significantly enhanced the model performance. Upon analyzing the feature importance within our models, certain features emerged as more substantial in predicting outcomes. Features such as "right temporal pole gray Matter volume," "psychiatric disorder comorbidity," and "left inferotemporal cortical thickness" were identified as crucial predictors in determining the medication response.Conclusion
This study effectively tackles the critical necessity for more precise methods to predict the response of individuals with epilepsy to ASMs. The integration of ASM data with patient characteristics and MRI-derived features can notably boost the accuracy of outcome predictions.Acknowledgements
No acknowledgement found.References
1. Zhang JH, Han X, Zhao HW, Zhao D, Wang N, Zhao T, He GN, Zhu XR, Zhang Y, Han JY et al: Personalized prediction model for seizure-free epilepsy with levetiracetam therapy: a retrospective data analysis using support vector machine. Br J Clin Pharmacol 2018, 84(11):2615-2624.
2. Wanted: a global campaign against epilepsy. Lancet 2012, 380(9848):1121.
3. Chen Z, Rollo B, Antonic-Baker A, Anderson A, Ma Y, O'Brien TJ, Ge Z, Wang X, Kwan P: New era of personalised epilepsy management. Bmj 2020, 371:m3658.
4. Devinsky O, Dilley C, Ozery-Flato M, Aharonov R, Goldschmidt Y, Rosen-Zvi M, Clark C, Fritz P: Changing the approach to treatment choice in epilepsy using big data. Epilepsy Behav 2016, 56:32-37.
5. Hakeem H, Feng W, Chen Z, Choong J, Brodie MJ, Fong SL, Lim KS, Wu J, Wang X, Lawn N et al: Development and Validation of a Deep Learning Model for Predicting Treatment Response in Patients With Newly Diagnosed Epilepsy. JAMA Neurol 2022, 79(10):986-996.
Figures