4938
Implementation of a Data Analysis Pipeline for intraoperative fMRI1Department of Neurosurgery, Medical University of Vienna, Vienna, Austria, 2High-field MR Center, Department of Biomedical Imaging and Image-guided Therapy, Medical University of Vienna, Vienna, Austria, 3Computational Imaging Research Lab (CIR), Department of Biomedical Imaging and Image-guided Therapy, Medical University of Vienna, Vienna, Austria, 4Department of Pediatrics and Adolescent Medicine, Medical University of Vienna, Vienna, Austria, 5Department of Radiodiagnostics, Medical University of Vienna, Vienna, Austria, 6Christian Doppler Laboratory for MR Imaging Biomarkers, Vienna, Austria
Synopsis
Keywords: Other Interventional, Software Tools, fMRI Preprocessing
Motivation: Immediate changes in functionality during brain surgery in tumor and epilepsy patients are worth investigating in order to improve prediction of surgical outcomes.
Goal(s): We want to implement a preprocessing-pipeline for pre- and post-resection data that allows comparison between both scans and the application of further analysis methods.
Approach: We propose a two-step approach, where we first pre-register the anatomical data to MNI-space with consideration of the resection area and then use this data in a second step for preprocessing of fMRI data.
Results: The preprocessing gives satisfactory results that enable further analysis of intraoperative fMRI data, such as PICA.
Impact: We showed that the difficult case of pre- and post-resection data preprocessing is feasible and allows analysis of intraoperative fMRI data. This enables further investigation of changes in brain functionality during surgery which might lead to improvements in neurosurgery.
Introduction
Functional MRI (fMRI) can image eloquent functions and is often used to compare pre- and post-surgery brain functionality. Intraoperative MRI allows visualization of brain networks directly before and after resection of a lesion, offering the option of immediately correcting the surgical result (intraoperative second look surgeries), but fMRI on these systems was limited by low field strengths1,2. With the first intraoperative 3T MRI scanner3,4 in Austria, we are able to image patients with higher Signal-to-Noise ratio which enables further investigation of changes in functional brain networks during surgery. We perform T1-weighted anatomical and resting-state fMRI scans right before and immediately after resection of a lesion with patients under anesthesia. Our goal is to get more insight on processes in brain functionality during surgery in tumor and epilepsy patients, which might lead to improvements in planning and prediction of surgery outcome in the future.The intraoperative MRI setup and type of data pose difficult challenges for data processing. The main challenge is the non-linear deformation and brain shift between pre- and post-resection scans. Especially the registration between these two scans is where standard processing tools fail, which is why a robust preprocessing pipeline for this kind of data is needed.
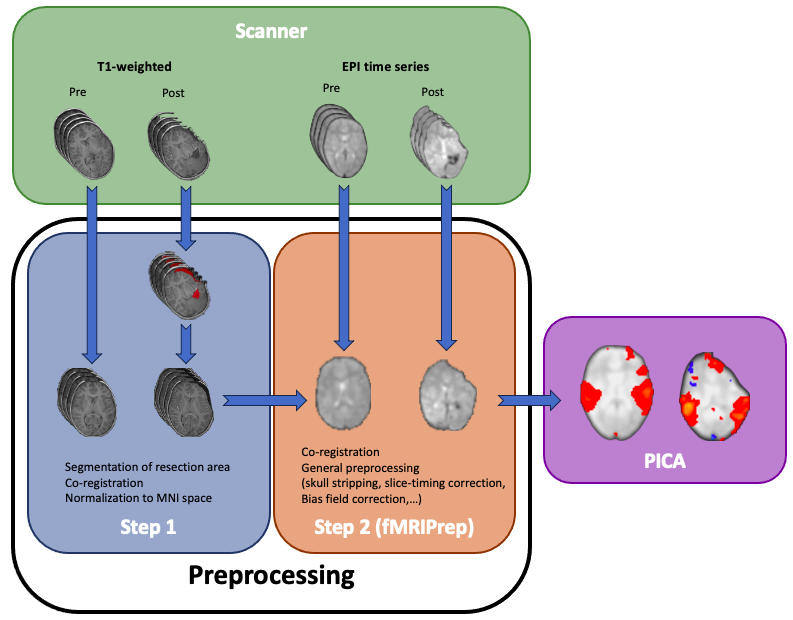
We propose a two-step approach to tackle this issue, where we first pre-register the anatomical data to the MNI-space with consideration of the resection area and use this data with fMRIPrep5 for preprocessing of the fMRI data, which can then be used for further analysis.
Methods
The data was acquired with a 3T Siemens Skyra (Siemens Healthineers, Erlangen, Germany) in a dual-room setup with a dockable patient transfer table and a combined 8-channel coil and head holder (NORAS, Hochberg, Germany). Intraoperative T2*-weighted EPI scans (3 mm isotropic resolution filtered to 3.3 mm with at least 24 slices) were done with a multiband factor and slice acceleration factor of 2 with 24 reference lines for a TR of 2s, a TE of 30 ms for 300 volumes resulting in a total scan time of 10 minutes. Pre- and post-resection data of 13 patients and 8 volunteers, which were measured with the 64-channel and intraoperative 8-channel coil, was used for development of most of the pipeline. The two-step approach was tested only on one patient so far. Data was converted to NIfTI-format and arranged as a BIDS-dataset6 using BIDScoin7. For preprocessing we decided on a two-stage approach, where in the first step a Matlab script based on SPM12 provided from the Monash University8 is used to non-linearly register the T1-weighted post-resection scan to the pre-resection scan with consideration of the resection area and then both images were normalized to the MNI-space8. In the second step, the pre-registered anatomical data was used as the input for fMRIPrep5, which again registers the anatomical data to MNI-space and also co-registers the functional data while additionally performing standard preprocessing steps (e.g. Bias field correction, slice-timing correction, etc.). The preprocessed data was then analyzed with FSL9, where a probabilistic independent component analysis (PICA)10,11 was performed on the fMRI resting-state data. A flowchart of the workflow is shown in figure 1.Results
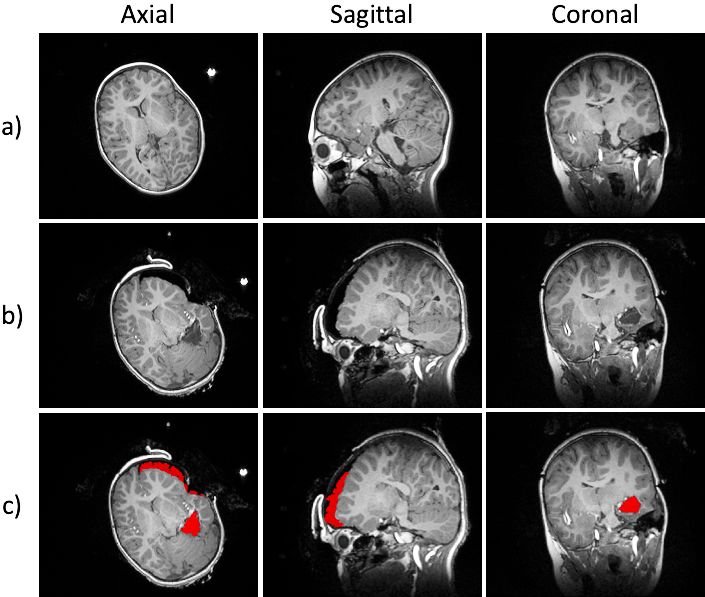
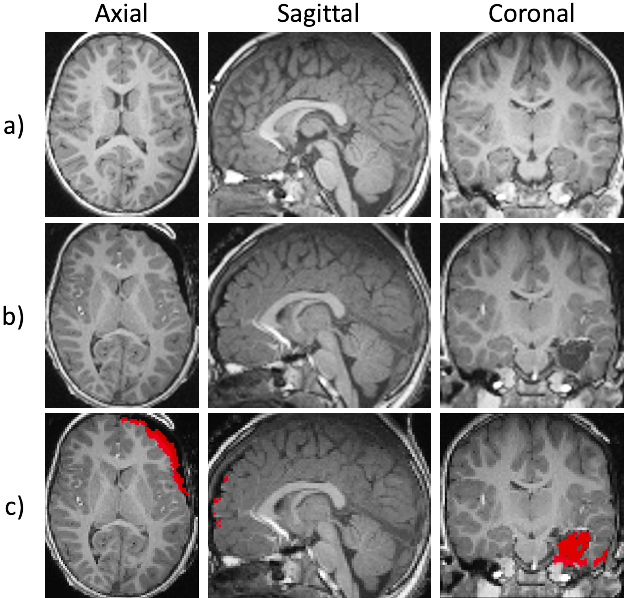
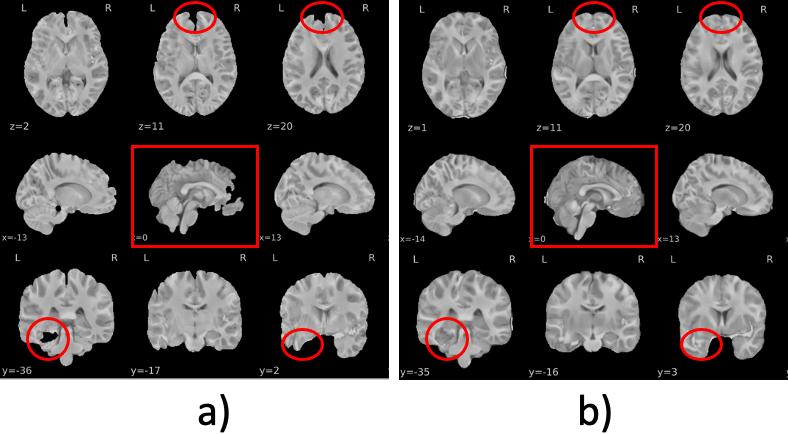
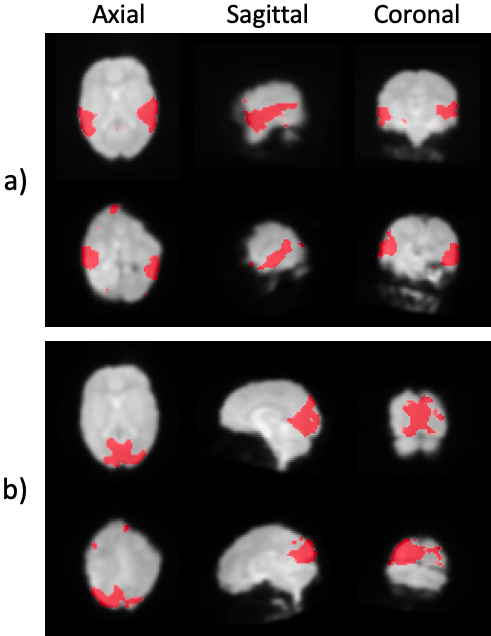
Figure 2 shows the original T1-weighted pre- and post-resection scans and the segmented resection area done in the first preprocessing step. The automatic segmentation gives good results and the registration of pre- and post-resection scans to MNI-space are satisfactory. Results after co-registration and normalization are shown in figure 3 for both scans. A significant improvement in the performance of fMRIPrep in co-registration and brain-extraction of anatomical data can be seen in figure 4, where a comparison with and without the first step is depicted. Red marked areas show that further analysis is not feasible without the first step in preprocessing.Figure 5 visualizes two components of PICA in pre- and post-resection scans, respectively. As shown, the identification of different networks is possible and it allows a comparison between pre- and post-resection resting-state networks, in order to further investigate changes in functionality during brain surgery.
Discussion
The two-step approach in preprocessing gives satisfactory results that enable further analysis of intraoperative fMRI data, such as PICA. However, the used tools might still not be powerful enough for this difficult case of co-registration, which is why we are planning to compare the registration performance of different deep-learning approaches.More analysis methods (e.g. functional connectivity) are also planned in the future, so that processes in brain functionality can be further investigated with the idea to improve neurosurgery in planning and surgical outcome.
Acknowledgements
This study was supported by the City of Vienna Fund for Innovative Interdisciplinary Cancer Research grant 22142. The financial support by the Austrian Federal Ministry for Digital and Economic Affairs, the National Foundation for Research, Technology and Development and the Christian Doppler Research Association is gratefully acknowledged.References
- Gasser, Thomas, Erol Sandalcioglu, Beate Schoch, Elke Gizewski, Michael Forsting, Dietmar Stolke, and Helmut Wiedemayer. “Functional Magnetic Resonance Imaging in Anesthetized Patients: A Relevant Step toward Real-Time Intraoperative Functional Neuroimaging.” Operative Neurosurgery 57, no. suppl_1 (July 1, 2005): 94–99. https://doi.org/10.1227/01.NEU.0000163488.91335.C5.
- Yamamoto, Adam Kenji, Joerg Magerkurth, Laura Mancini, Mark J. White, Anna Miserocchi, Andrew W. McEvoy, Ian Appleby, et al. “Acquisition of Sensorimotor fMRI under General Anaesthesia: Assessment of Feasibility, the BOLD Response and Clinical Utility.” NeuroImage: Clinical 23 (2019): 101923. https://doi.org/10.1016/j.nicl.2019.101923.
- Pamir, M. Necmettin. “3 T ioMRI: The Istanbul Experience.” In Intraoperative Imaging, edited by M. Necmettin Pamir, Volker Seifert, and Talat Kiris, 109:131–37. Acta Neurochirurgica Supplementum. Vienna: Springer Vienna, 2011. https://doi.org/10.1007/978-3-211-99651-5_20.
- Ginat, Daniel Thomas, Brooke Swearingen, William Curry, Daniel Cahill, Joseph Madsen, and Pamela W. Schaefer. “3 Tesla Intraoperative MRI for Brain Tumor Surgery: 3 Tesla Intraoperative MRI for Brain Tumor Surgery.” Journal of Magnetic Resonance Imaging 39, no. 6 (June 2014): 1357–65. https://doi.org/10.1002/jmri.24380.
- Esteban, Oscar, Christopher J. Markiewicz, Ross W. Blair, Craig A. Moodie, A. Ilkay Isik, Asier Erramuzpe, James D. Kent, et al. “fMRIPrep: A Robust Preprocessing Pipeline for Functional MRI.” Nature Methods 16, no. 1 (January 2019): 111–16. https://doi.org/10.1038/s41592-018-0235-4.
- Gorgolewski, Krzysztof J., Tibor Auer, Vince D. Calhoun, R. Cameron Craddock, Samir Das, Eugene P. Duff, Guillaume Flandin, et al. “The Brain Imaging Data Structure, a Format for Organizing and Describing Outputs of Neuroimaging Experiments.” Scientific Data 3, no. 1 (June 21, 2016): 160044. https://doi.org/10.1038/sdata.2016.44.
- Zwiers, Marcel Peter, Stefano Moia, and Robert Oostenveld. “BIDScoin: A User-Friendly Application to Convert Source Data to Brain Imaging Data Structure.” Frontiers in Neuroinformatics 15 (January 13, 2022): 770608. https://doi.org/10.3389/fninf.2021.770608.
- Cahill, Varduhi, Benjamin Sinclair, Charles B. Malpas, Anne M. McIntosh, Zhibin Chen, Lucy E. Vivash, Marie F. O’Shea, et al. “Metabolic Patterns and Seizure Outcomes Following Anterior Temporal Lobectomy.” Annals of Neurology 85, no. 2 (February 2019): 241–50. https://doi.org/10.1002/ana.25405.
- Jenkinson, Mark, Christian F. Beckmann, Timothy E.J. Behrens, Mark W. Woolrich, and Stephen M. Smith. “FSL.” NeuroImage 62, no. 2 (August 2012): 782–90. https://doi.org/10.1016/j.neuroimage.2011.09.015.
- Beckmann, C.F., and S.M. Smith. “Probabilistic Independent Component Analysis for Functional Magnetic Resonance Imaging.” IEEE Transactions on Medical Imaging 23, no. 2 (February 2004): 137–52. https://doi.org/10.1109/TMI.2003.822821.
- Hyvarinen, A. “Fast and Robust Fixed-Point Algorithms for Independent Component Analysis.” IEEE Transactions on Neural Networks 10, no. 3 (May 1999): 626–34. https://doi.org/10.1109/72.761722.
Figures