4933
Intraoperative 3T MRI as navigator for laser interstitial thermal therapy in paediatric epilepsy and tumour surgery1High-field MR Center, Department of Biomedical Imaging and Image-guided Therapy, Medical University of Vienna, Vienna, Austria, 2Department of Neurosurgery, Medical University of Vienna, Vienna, Austria, 3Division of Neuroradiology and Musculoskeletal Radiology, Department of Biomedical Imaging and Image-guided Therapy, Medical University of Vienna, Vienna, Austria, 4Center for Rare and Complex Childhood Onset Epilepsies, Member of ERN EpiCARE, Department of Pediatrics and Adolescent Medicine, Medical University of Vienna, Vienna, Austria
Synopsis
Keywords: Thermometry/Thermotherapy, Interventional Devices, MR-guided LITT
Motivation: MR-guided laser interstitial thermal therapy (LITT) uses laser fibres to ablate lesions under MR-thermometry monitoring. Distance between OR and MRI complicates this procedure, but previous generations of intraoperative MRIs were limited to fields up to 1.5T.
Goal(s): We investigated a dual-room setup for intraoperative 3T MRI as navigation/monitoring for LITT.
Approach: In eleven paediatric patients, we demonstrated this setup as navigation/monitoring for LITT.
Results: We quantified achievable time and precision parameters, e.g., a mean total surgery time of 4.9 hours.
Impact: Minimised surgery time and complications as well as improved treatment monitoring for laser interstitial thermal therapy make dual-room intraoperative 3T MRIs beneficial for paediatric patients.
Introduction
MR-guided laser interstitial thermal therapy (LITT)1,2 is a minimally invasive surgical technology that can ablate tumours and epileptogenic regions3–5. Using optical fibre cables, a laser heats up a target volume in order to destroy tissues and only requires a small cranial opening. Minimal surgical trauma, shorter hospitalisation, and reduced chance of negative side effects make it beneficial for patients6. A prerequisite for LITT is the utilisation of an MRI to monitor the placement of optical fibres by structural MRI and thermal ablation of tissue by MR-thermometry7. Using general-purpose MRI requires transferring patients between OR and radiology and removing the stereotactic frame, decreasing precision and increasing infection risks5. Previous generations of dedicated intraoperative MRI (ioMRI) systems offered fields only up to 1.5T, limiting spatial and temporal resolution.For our dual-room intraoperative 3T MRI8,9 that minimises transport distance and maximises SNR, we quantified its use in the LITT-workflow and patient safety.
Methods
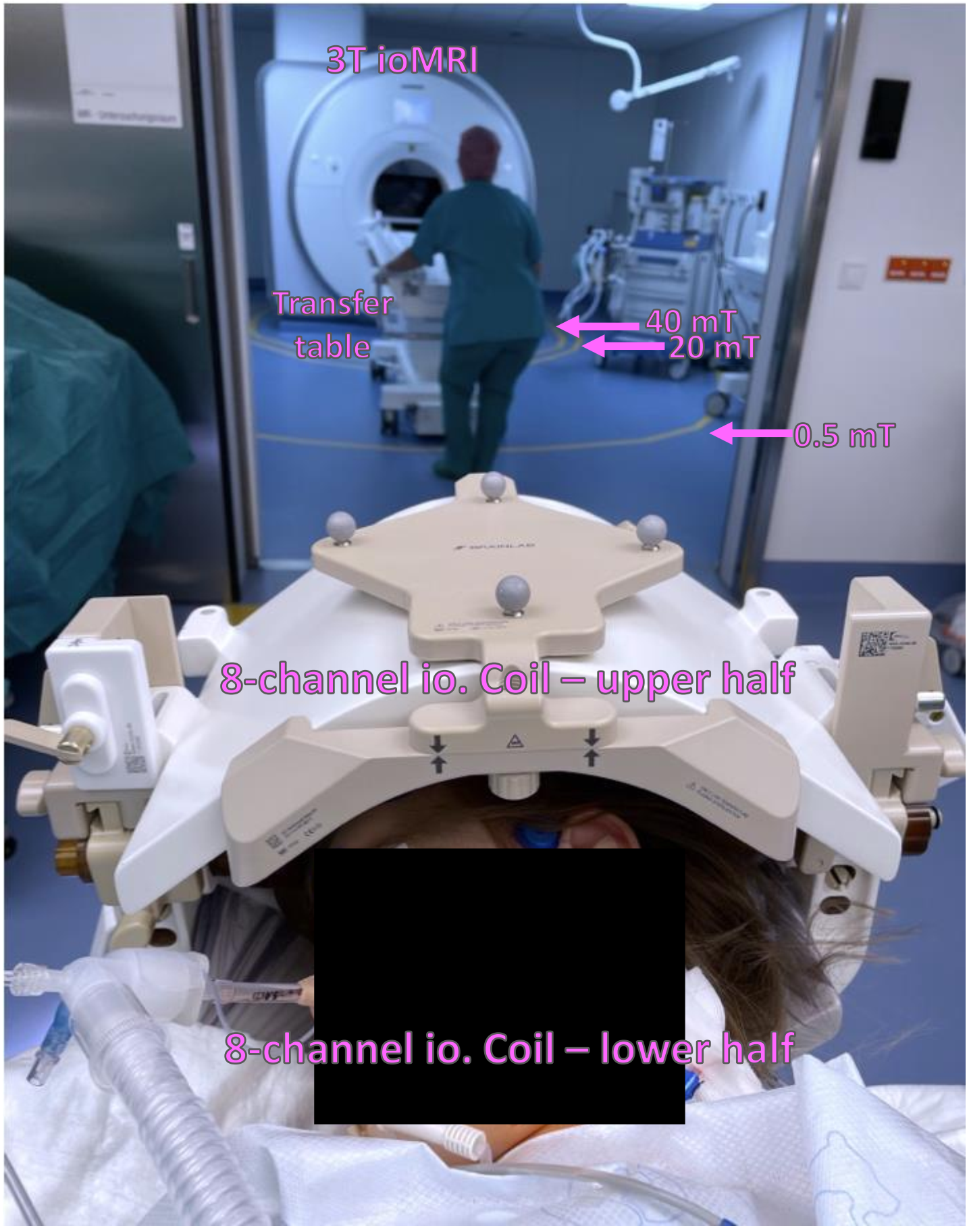
For this study, evaluated LITT procedures performed from January 2021 to June 2022 in paediatric patients with focal cortical dysplasia, tuberous sclerosis, or gliomas. We used a 3T Skyra (Siemens Healthineers) system with XQ gradients (45 mT/m gradient strength and 200 mT/m/s slew rate), adjacent to an OR in a dual-room setup and equipped with a dockable patient transfer table and a combined 8-channel coil/head holder (NORAS). After patient fixation under anaesthesia (Fig.1), we performed a routine ioMRI protocol consisting of T1-weighted imaging (T1w, TR 2000 ms, TE 2.78 ms, TI 1100 ms, GRAPPA factor 2, flip angle 8 degrees, 1×1×1 mm resolution, 6:48 minutes) with and without contrast enhancement, and T2-weighted imaging (T2w, TR 3200 ms, TE 299 ms, variable flip angle, 0.5×0.5×1 mm resolution, 6:48 minutes).Based on these images, laser fibres were stereotactically implanted using a neuronavigation system (either StealthStation S8, Medtronic or Curve, BrainLab) (Fig.2). Patients were then moved back into the MRI, where T1w FLASH MRI centred around the target region (TR 44 ms, TE 2.48 ms, flip angle 70 degrees, 3 slices at 1×1×1 mm resolution, 9 averages, 1:22 min) was acquired. We then performed LITT using a Visualase system (Medtronic) monitored by MR-thermometry7 in two planes (TR 24 ms, TE 10 ms, flip angle 30 degrees, 1×1×3 mm resolution, continuous acquisition during LITT), heating the target volume between 50°C and 70°C10. Post-LITT, ablation extent was confirmed using T1w contrast-enhanced imaging and T2w-imaging, then the patient was moved back into the OR for the surgical finish. We measured ablation volume, entry point error, and target point error in the neuronavigation software.
Results
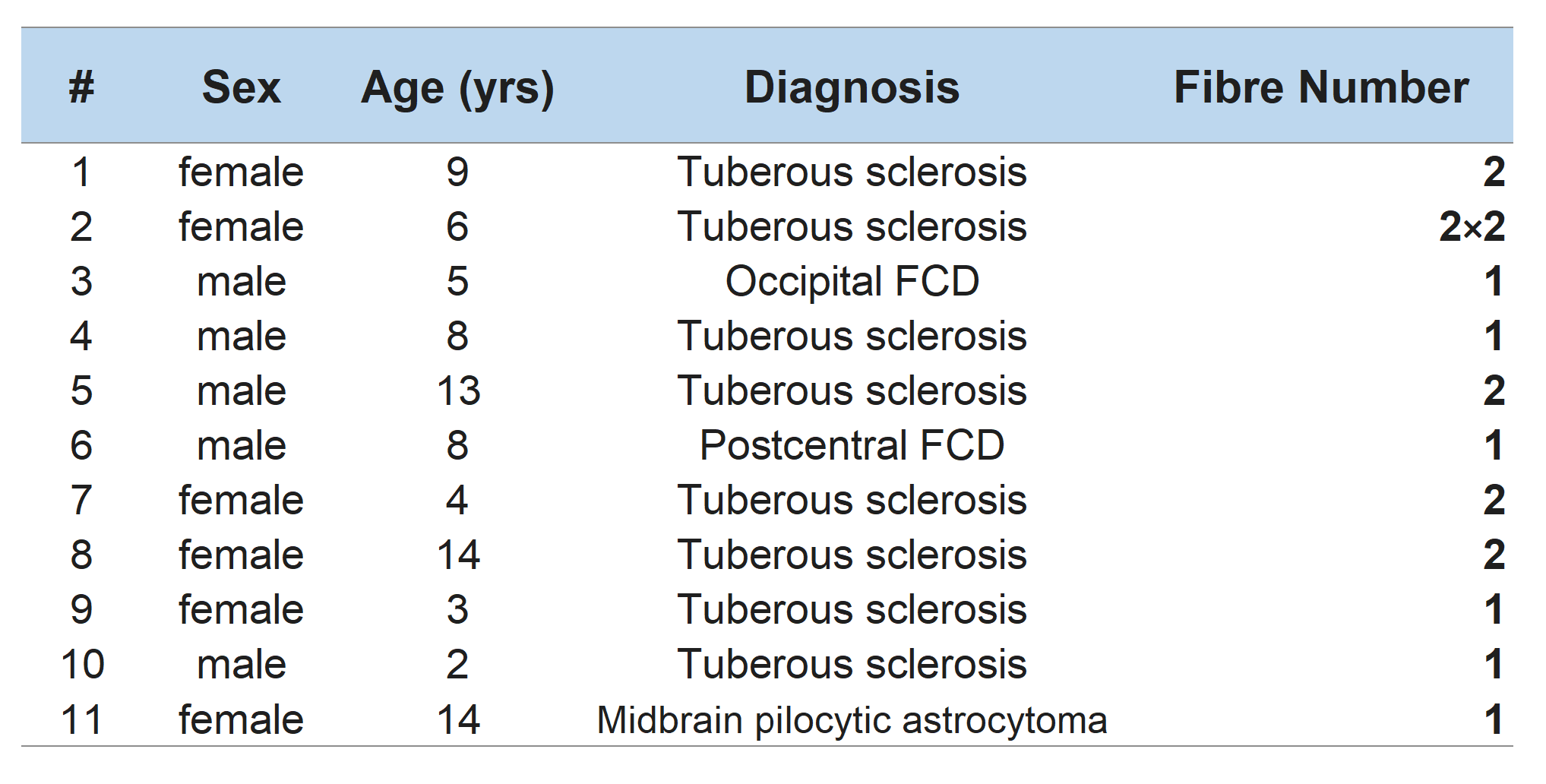
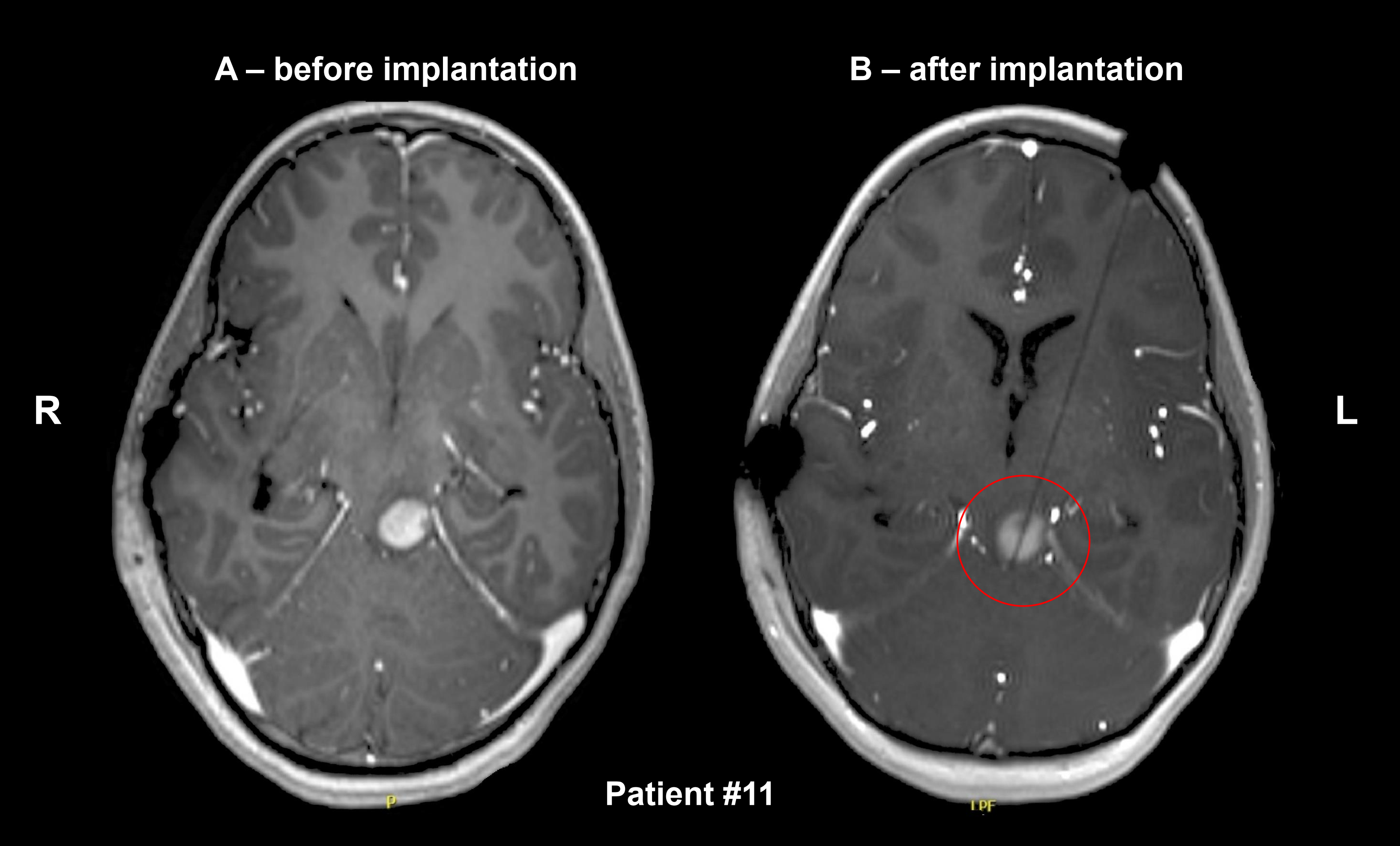
In total, we performed 12 LITT procedures in 11 children (mean age 7.1 years [range 2-14 years], pathologies and fibre counts listed in Fig.3). MR-thermometry was successful to vendor specifications.Of a mean total surgery time of 4.9 hours [range: 3.5 to 5.5 hours], the mean transfer time from OR to MRI and vice versa was 9.0±1.6 minutes, the mean fibre insertion time was 32±14 min and the mean ablation time was 19.4 minutes. Fig.4 demonstrates fibre placement into a midbrain pilocytic astrocytoma.
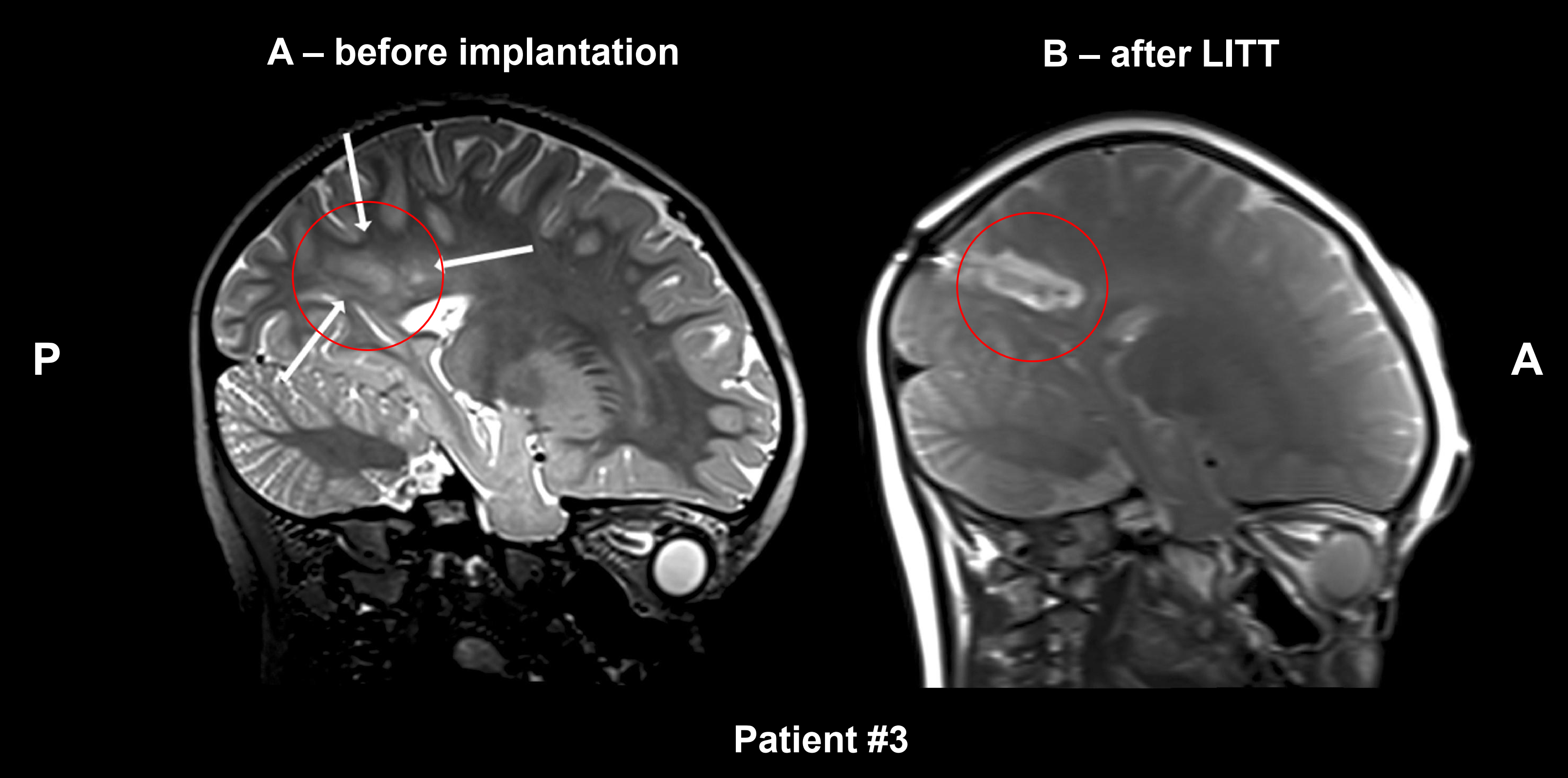
With an entry point error of 2.8±1.7 mm and a target point error of 3.7±2.4 mm the mean ablation volume was 6.93 cm³. Fig.5 shows the effect of LITT-induced ablation onto an occipital focal cortical dysplasia.
No surgical site or intracranial infections occurred, yet there was one haemorrhagic event during implantation, which did not require surgical evacuation. At a follow-up time of 22 months, 50% of the patients with seizures were seizure free (Engel grade I).
Discussion and Conclusions
As LITT applications are rising11, efficient and safe procedures directly impact clinical practice. Our intraoperative MRI suite successfully minimised transport times and supplied navigation/monitoring images that allowed a successful and fast LITT procedure in all cases of our cohort12 with an accuracy comparable to literature13–15.While the inherent design of MR-guided LITT does not allow to directly compare 3T intraoperative scanners to lower field systems in the same subject, comparison to 0.5T16 and 1.5T17 studies shows that a 3T intraoperative MRI with an 8-channel coil allows higher resolution and lower TR for thermometry sequences, therefore enhancing precision. Using a dedicated head holder / MR-coil does increase surgical accuracy compared to separate OR/MRI solutions.
The benefits of our approach, especially for children, can be summarised as decreased risks of moving patients under anaesthesia, staying within an OR environment, the possibility to quickly insert additional fibres, and minimisation of total surgical time. This study was limited by cohort size and the fact that in tuberous sclerosis the primary surgical goal is only a reduction in seizure frequency.
Acknowledgements
This study was supported by the City of Vienna Fund for Innovative Interdisciplinary Cancer Research grant 22142.References
17. Cernicanu A, Lepetit-Coiffe M, Roland J, Becker CD, Terraz S. Validation of fast MR thermometry at 1.5 T with gradient-echo echo planar imaging sequences: phantom and clinical feasibility studies. NMR Biomed. 2008;21(8):849-858. doi:10.1002/nbm.1267
Figures