4920
Altered blood pulsatility & small vessel disease marker associations in obstructive sleep apnoea post-continuous positive airway pressure1Centre for Clinical Brain Sciences and UK Dementia Research Institute, University of Edinburgh, Edinburgh, United Kingdom, 2School of Applied Sciences, University of the West of England, Bristol, United Kingdom, 3University for Foreigners of Perugia, Perugia, Italy, 4School of Health in Social Science, University of Edinburgh, Edinburgh, United Kingdom, 5Department of Medical Biophysics, University of Toronto, Toronto, ON, Canada, 6Hurvitz Brain Sciences Program, Sunnybrook Research Institute, Toronto, ON, Canada, 7Institute of Cognitive Neurology and Dementia Research, Otto-Von-Guericke University and DZNE Magdeburg, Madgeburg, Germany, 8Institute of Medical Sciences, University of Toronto, Toronto, ON, Canada, 9Department of Sleep Medicine, Royal Infirmary of Edinburgh, NHS Lothian, Edinburgh, United Kingdom
Synopsis
Keywords: Neurofluids, Blood vessels, Phase contrast MRI
Motivation: Sleep affects vascular health and brain waste clearance. Sleep disorders, including obstructive sleep apnoea (OSA), are associated with higher small vessel disease (SVD) burden increasing stroke/dementia risk. OSA treatment relies on continuous positive airway pressure (CPAP).
Goal(s): We aimed to assess the effect of CPAP on MRI-based blood pulsatility index (PI) measures and associations with SVD burden.
Approach: We assessed arterial/venous PI using phase-contrast MRI in patients with moderate/severe OSA before and after 4 months CPAP.
Results: Arterial PI tended lower post-CPAP, consistent with better vascular health. Post-CPAP patients with higher venous PI had less severe basal ganglia perivascular space burden.
Impact: Few studies have investigated MRI-based blood pulsatility index (PI) in obstructive sleep apnoea (OSA). We found effective treatment may improve brain vascular health, altering blood PI. Higher venous PI post-treatment may link to brain waste clearance, but requires further study.
Introduction
Sleep is thought to be important for brain vascular health, including waste clearance.1-3 Impaired brain waste clearance is linked to higher vascular pulsatility in rodent studies.1,3,4 Sleep disorders are associated with higher SVD burden,5,6 increased stroke and dementia risk.2,7 Obstructive sleep apnoea (OSA) is a sleep disorder where the airway becomes blocked, leading to lack of oxygen. Treatment typically relies on continuous positive airway pressure (CPAP).2 Effective OSA treatment might help improve brain health including vascular pulsatility. However, to our knowledge the effect of CPAP therapy on MRI-based blood pulsatility index (PI) has not been investigated in OSA. We assessed arterial and venous PI in patients with OSA pre- and post-CPAP, investigating whether blood PI differed and associations with key markers of SVD.Methods
We recruited patients with moderate/severe OSA diagnosed using level 1 polysomnography/level 3 home sleep apnoea testing. The patients underwent WatchPAT sleep studies (WatchPAT200, Itamar Medical, Israel) before and after CPAP to assess sleep quality.We scanned patients pre- and post- 4 months CPAP on a 3 T Siemens Prisma MRI scanner (Fig.1). The imaging protocol included: T1-weighted, T2-weighted, FLAIR, SWI and diffusion MRI. We visually rated: Fazekas score, perivascular space (PVS) score in the basal ganglia (BG) and centrum semiovale, microbleeds, lacunes and atrophy using the STRIVE-1 criteria.8 We calculated the SVD score, a summary SVD burden metric based on the visual scores.9 We segmented subcortical grey, normal-appearing white matter and white matter hyperintensity masks, using validated methods, checked and manually corrected as necessary.10 We calculated percentage WMH normalised to intracranial volume (ICV). PVS volume and count were computationally segmented in the BG and CSO using validated techniques.11,12
Additionally, we acquired 2D phase-contrast MRI (PC-MRI) axially perpendicular to the carotid arteries at the C2-3 level of the spine (TR/TE: 19.6/5.8 ms, flip angle: 12°, spatial res.: 1.0 x 1.0 mm2, temp res.: 39.2 ms, venc: 70 cm/s) and coronally perpendicular to the superior sagittal sinus (SSS) (TR/TE: 21.7/6.6 ms, flip angle: 12°, spatial res.: 0.71 x 0.71 mm2, temp res.: 43.4 ms, venc: 50 cm/s). We interpolated the phase images across 32 timeframes, covering the cardiac cycle, using a finger pulse oximeter for retrospective cardiac gating.
Based on established methods,13 we manually delineated regions of interest including the internal carotid and vertebral arteries and superior sagittal sinus. We calculated the blood flow across the cardiac cycle by multiplying the pixel velocity by the area and summing across each ROI. We calculated arterial and venous PI using a modified version of Gosling’s equation as PI=(flowmax-flowmin)/flowmean.14
We tested for differences pre- vs post-CPAP using paired t-tests. We assessed associations between arterial or venous PI and each SVD marker using separate linear mixed models (LMM) and an interaction term between the SVD marker and visit. We also assessed associations between peripheral apnoea-hyponea index (pAHI), and arterial or venous PI including an interaction term for PI and visit. We adjusted all LMM for age and body-mass index (BMI).
Results
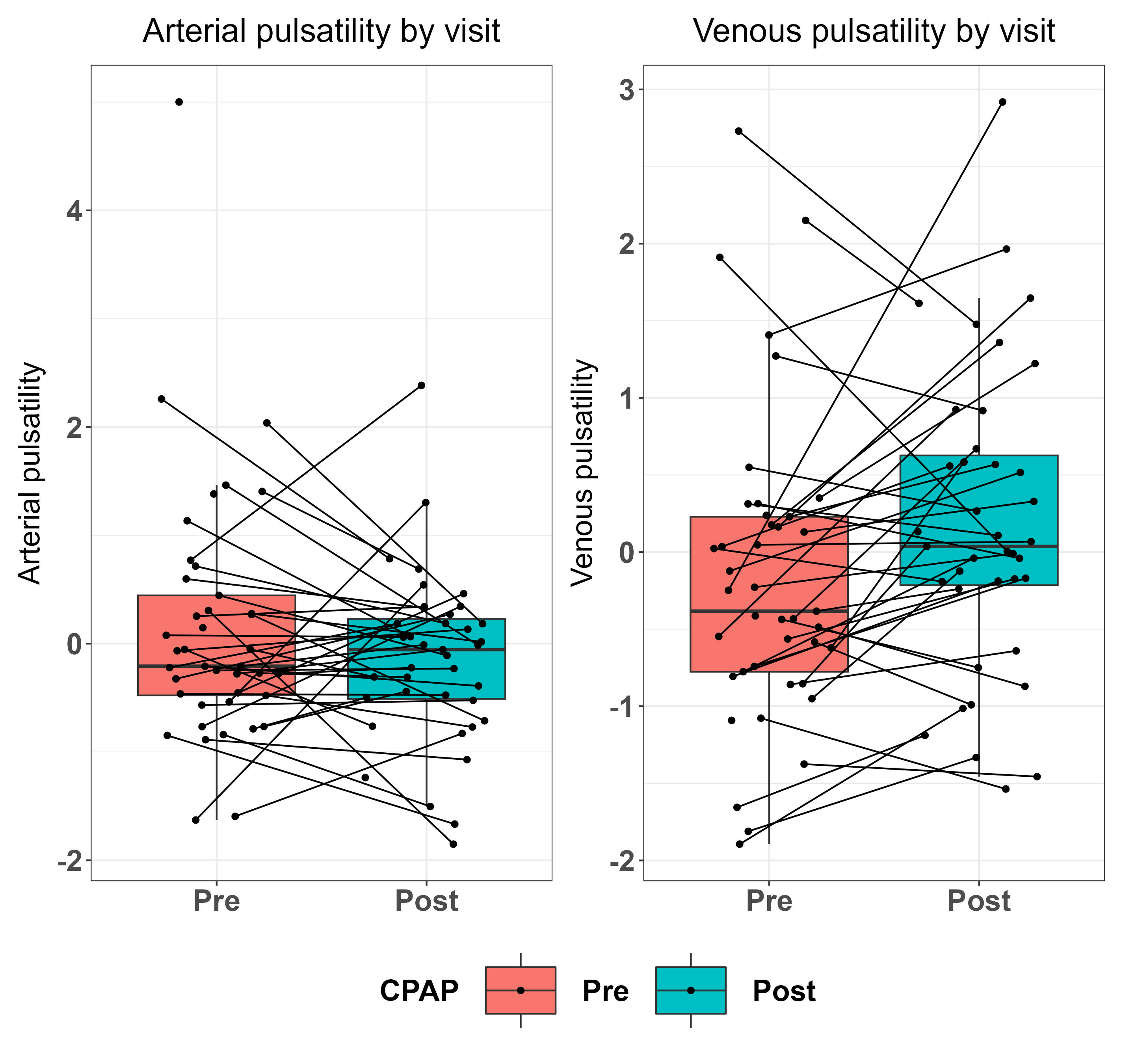
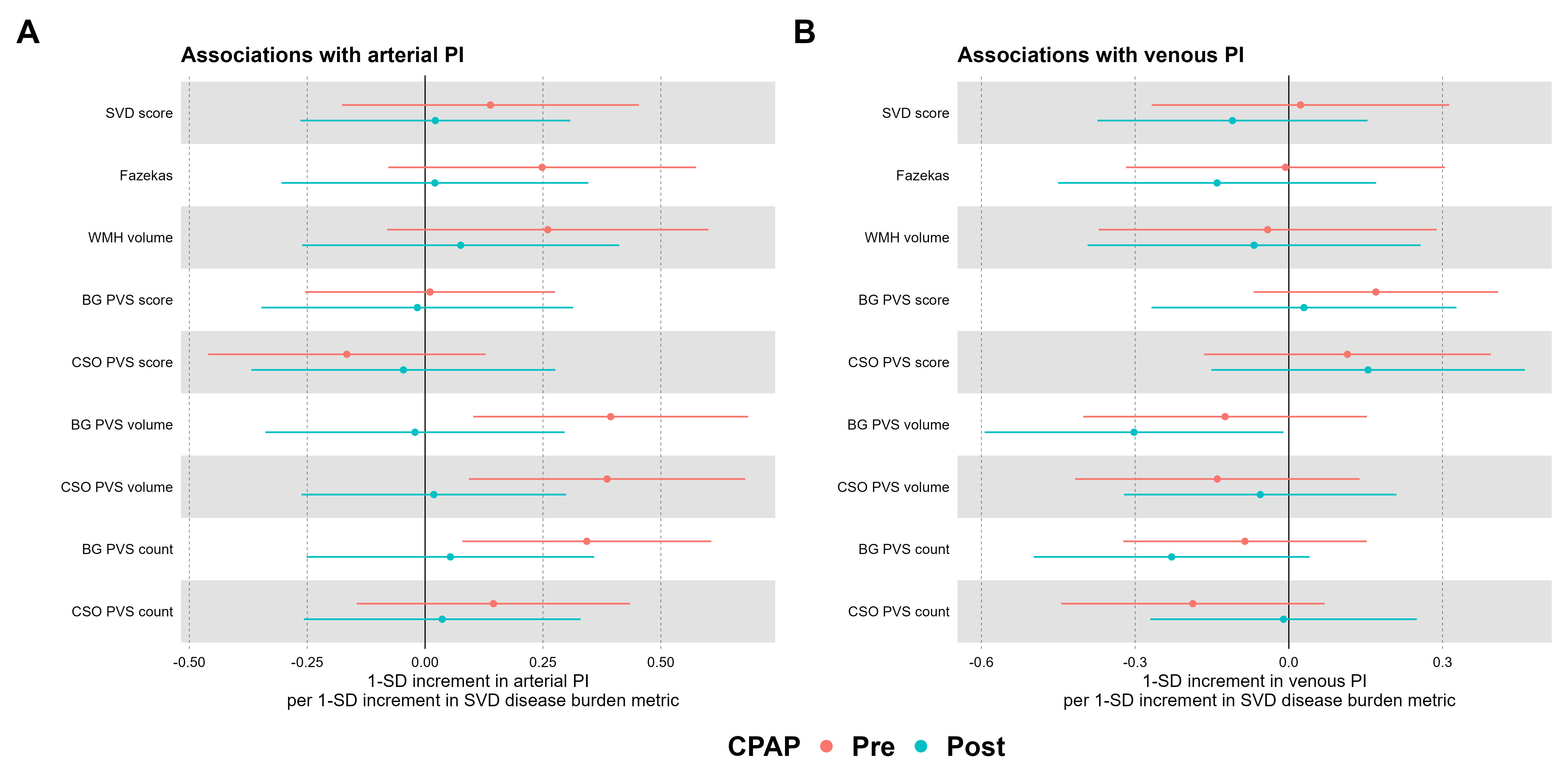
We recruited 44 patients (30 male, 14 female; Age: 49.55±9.63 years). 2 patients could not be scanned due to physical constraints, 2 did not attend for scans post-CPAP. After 4 months CPAP, arterial pulsatility tended lower (t=-1.041, 95% confidence interval (95%CI):-0.126,0.040, p=0.305) and venous pulsatility higher (t=1.967, 95%CI:-0.001,0.087, p=0.056) (Fig.2).Pre-CPAP patients with higher arterial PI had higher PVS volume (e.g. BG:β=0.394, 95%CI:0.102,0.685, p=0.005) and count (e.g. BG:β=0.343, 95%CI=0.0790,0.607, p=0.013), but arterial PI differed little with SVD markers post-CPAP (Fig.3A). Venous PI showed no sustained associations with SVD markers pre-CPAP, but post-CPAP patients with higher venous PI had lower BG PVS volume (β=-0.302, 95%CI=-0.594,-0.010, p=0.031) and count (β=-0.229, 95%CI=-0.498,0.041, p=0.103) (Fig.3B).
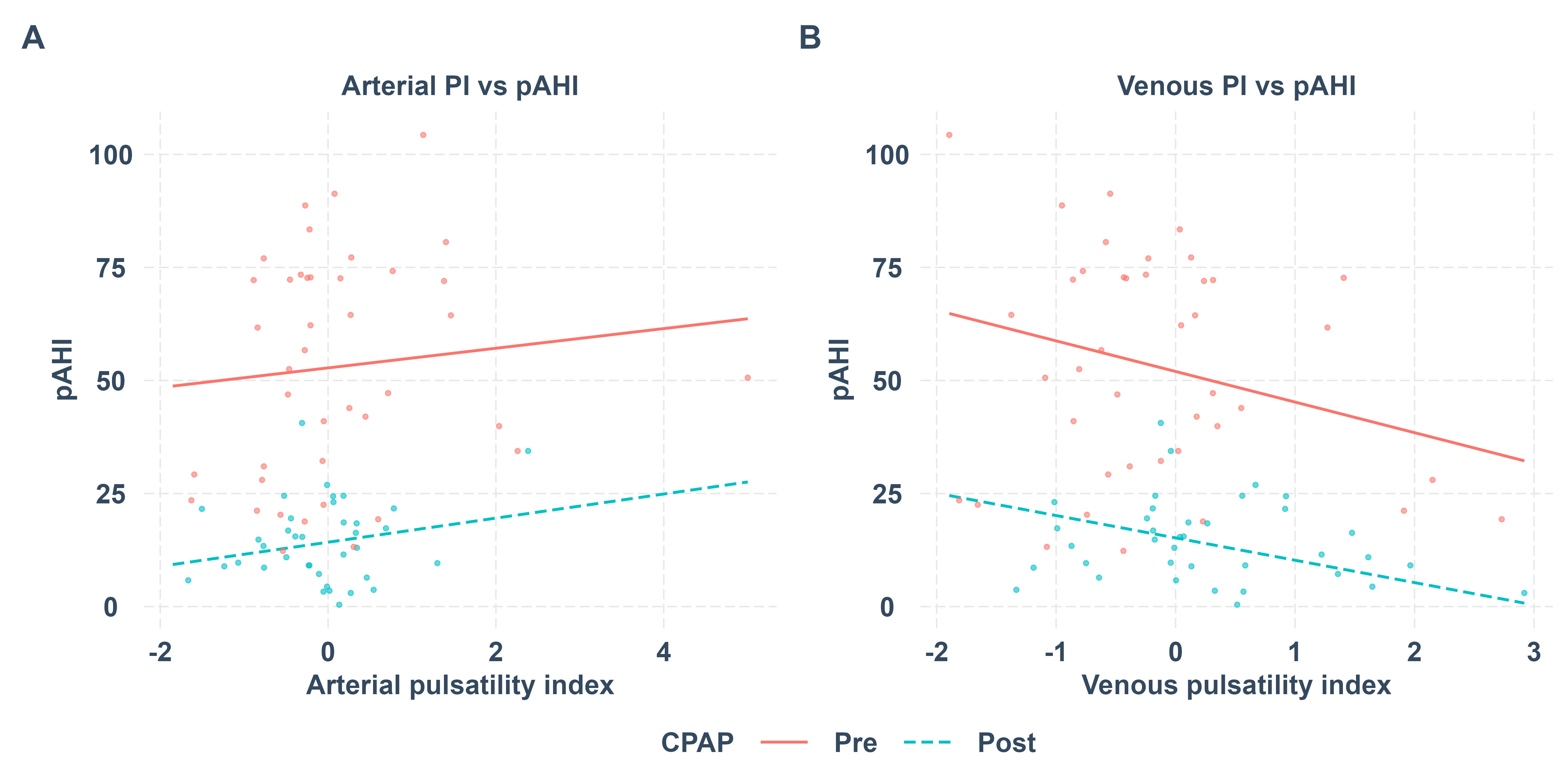
Patients with higher pAHI had lower venous PI (e.g. Pre-CPAP:β=-0.252, 95%CI=-0.476,-0.028, p=0.028) pre- and post-CPAP, but arterial PI differed little (Fig.4).
Discussion
We found altered blood PI and SVD markers associations pre- versus post-CPAP in OSA. Patients with worse SVD have generally higher arterial PI,15-17 lower arterial PI post-CPAP is consistent with improved vascular health. Associations between venous PI and SVD burden are less widely explored.13,15 As PVS and sleep are implicated in brain waste clearance associations between higher venous PI and lower BG PVS post-CPAP may reflect this.1 In rodents glymphatic clearance and intracranial pressure were higher during CPAP,18 which could be consistent with increased venous pulsatility.Conclusion
We found CPAP altered associations between blood pulsatility and SVD markers in OSA which may be consistent with improved vascular health and perhaps link to brain waste clearance, though further validation is needed.Acknowledgements
We thank the Edinburgh Imaging Facility (Royal Infirmary of Edinburgh) radiographers for their involvement, and the patients for taking part in this study.References
1. Brown R, Benveniste H, Black SE, Charpak S, Dichgans M, Joutel A, et al. Understanding the role of the perivascular space in cerebral small vessel disease. Cardiovasc Res. 2018;114:1462-1473
2. Ercolano E, Bencivenga L, Palaia ME, Carbone G, Scognamiglio F, Rengo G, et al. Intricate relationship between obstructive sleep apnea and dementia in older adults. Geroscience. 2023
3. Agarwal N, Lewis LD, Hirschler L, Rivera LR, Naganawa S, Levendovszky SR, et al. Current understanding of the anatomy, physiology, and magnetic resonance imaging of neurofluids: Update from the 2022 "ISMRM imaging neurofluids study group" workshop in rome. J Magn Reson Imaging. 2023
4. Wardlaw JM, Benveniste H, Nedergaard M, Zlokovic BV, Mestre H, Lee H, et al. Perivascular spaces in the brain: Anatomy, physiology and pathology. Nat Rev Neurol. 2020;16:137-153
5. Song TJ, Park JH, Choi KH, Chang Y, Moon J, Kim JH, et al. Moderate-to-severe obstructive sleep apnea is associated with cerebral small vessel disease. Sleep Med. 2017;30:36-42
6. Huang Y, Yang C, Yuan R, Liu M, Hao Z. Association of obstructive sleep apnea and cerebral small vessel disease: A systematic review and meta-analysis. Sleep. 2020;43
7. Marin JM, Carrizo SJ, Vicente E, Agusti AG. Long-term cardiovascular outcomes in men with obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway pressure: An observational study. Lancet. 2005;365:1046-1053
8. Wardlaw JM, Smith EE, Biessels GJ, Cordonnier C, Fazekas F, Frayne R, et al. Neuroimaging standards for research into small vessel disease and its contribution to ageing and neurodegeneration. Lancet Neurol. 2013;12:822-838
9. Staals J, Makin SD, Doubal FN, Dennis MS, Wardlaw JM. Stroke subtype, vascular risk factors, and total mri brain small-vessel disease burden. Neurology. 2014;83:1228-1234
10. Clancy U, Garcia DJ, Stringer MS, Thrippleton MJ, Valdes-Hernandez MC, Wiseman S, et al. Rationale and design of a longitudinal study of cerebral small vessel diseases, clinical and imaging outcomes in patients presenting with mild ischaemic stroke: Mild stroke study 3. Eur Stroke J. 2021;6:81-88
11. Ballerini L, Lovreglio R, Valdes Hernandez MDC, Ramirez J, MacIntosh BJ, Black SE, et al. Perivascular spaces segmentation in brain mri using optimal 3d filtering. Sci Rep. 2018;8:2132
12. Bernal J, Valdes-Hernandez MDC, Escudero J, Duarte R, Ballerini L, Bastin ME, et al. Assessment of perivascular space filtering methods using a three-dimensional computational model. Magn Reson Imaging. 2022;93:33-51
13. Shi Y, Thrippleton MJ, Blair GW, Dickie DA, Marshall I, Hamilton I, et al. Small vessel disease is associated with altered cerebrovascular pulsatility but not resting cerebral blood flow. J Cereb Blood Flow Metab. 2020;40:85-99
14. Gosling RG, King DH. Arterial assessment by doppler-shift ultrasound. Proc R Soc Med. 1974;67:447-449
15. Shi Y, Thrippleton MJ, Marshall I, Wardlaw JM. Intracranial pulsatility in patients with cerebral small vessel disease: A systematic review. Clin Sci (Lond). 2018;132:157-171
16. Lee WJ, Jung KH, Nam HW, Lee YS. Effect of obstructive sleep apnea on cerebrovascular compliance and cerebral small vessel disease. PLoS One. 2021;16:e0259469
17. Wong B, Tong JY, Schulz AM, Graham SL, Farah CS, Fraser CL. The impact of continuous positive airway pressure treatment on retinal vascular changes in obstructive sleep apnea. J Clin Sleep Med. 2021;17:983-991
18. Ozturk B, Koundal S, Al Bizri E, Chen X, Gursky Z, Dai F, et al. Continuous positive airway pressure increases csf flow and glymphatic transport. JCI Insight. 2023;8
Figures