4918
Vulnerable plaques are associated with white matter hyperintensities: a finding on high-resolution vessel wall magnetic resonance imaging.1First Affiliated Hospital of Harbin Medical University, Harbin, China, 2Philips Healthcare, Beijing, China
Synopsis
Keywords: Atherosclerosis, Atherosclerosis
Motivation: Cerebral small vessel disease (CSVD) is a common disease in the elderly with uncertain causes. We wanted to explore whether intracerebral macrovascular disease is related to CSVD.
Goal(s): This study was to explore the relationship between atherosclerotic plaque characteristics and wall changes and white matter hyperintensities (WMH) associated with CSVD.
Approach: As a non-invasive technique, high-resolution vessel wall magnetic resonance imaging can display vascular image and measure plaque parameters and vascular wall changes. Using the tools, the differences between WMH groups were analyzed.
Results: WMH was associated with unstable plaques. Age, wide distribution and significant enhancement were independent factors affecting WMH.
Impact: Unstable atherosclerotic plaque may cause CSVD, suggesting that clinicians should pay more attention to patients with ischemic stroke. The plaque vulnerability parameter may be a new index to evaluate the degree of WMH.
Introduction
Subcortical white matter lesion is one of the common brain parenchyma manifestations of CSVD, which shows white matter hyperintensities (WMH) in the lateral ventricle and deep white matter on magnetic resonance images. Some studies have shown that large artery atherosclerosis is related to CSVD, but the exact pathogenesis is unknown1-2. As a new non-invasive vascular wall imaging technique, High-resolution vessel wall magnetic resonance imaging (HR-vwMRI) can show the short axis of intracranial and extracranial vascular walls and discover the morphological structure and composition of unstable plaques. The aim of the study is to measure the wall changes and plaque characteristics of the middle cerebral artery (MCA) in patients with different WMH groups and to explore the correlation between plaque vulnerability and WMH.Methods
We retrospectively collected patients with acute ischemic stroke from May 2021 to October 2023 who were suspected of MCA stenosis. All subjects underwent routine head MRI and HR-vwMRI using a 3.0 T Achieva MR scanner (Philips Healthcare, Best, Netherlands) and a 16-channel head and neck coil. Based on the T2 FLAIR-TRA imaging, WMH was divided into 2 groups according to the Fazekas score (0-6), which were the no and mild WMH group (Fazekas0-2), and the moderate and severe WMH group (Fazekas3-6)3. Plaque characteristics were analyzed by two radiologists. To determine the presence of intraplaque hemorrhage (IPH): IPH was defined as areas of high signal (>150% of the adjacent area of the vessel wall) on the T1W-3D-VISTA images4. Plaque enhancement was categorized into grades 0-2, we defined grade 0-1 enhancement as non-significant enhancement and grade 2 as significant enhancement. The plaque was considered to be wide when it was distributed in two or more vessel sidewalls and limited otherwise. The vessel area and the lumen area at the stenosis level, and the vessel area and the lumen area at the reference level, were recorded. According to the formulas, the stenosis degree, remodeling index, and plaque load were calculated. T-tests, nonparametric rank-sum tests, and chi-square analyses were used to compare the plaque vulnerability parameters between WMH groups. Spearman's correlation and binary logistic regression analysis were used to compare the correlation between WMH classifications and plaque parameters.Results
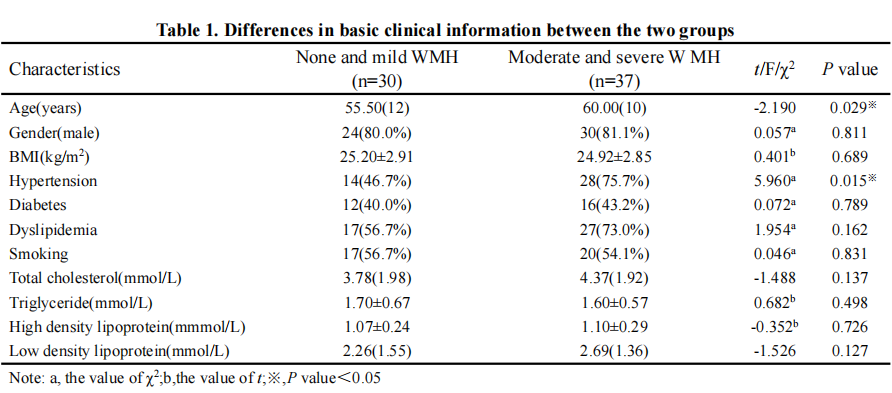
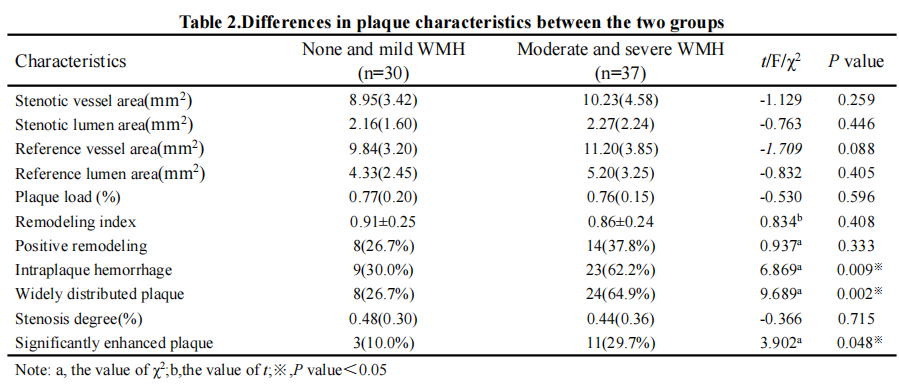
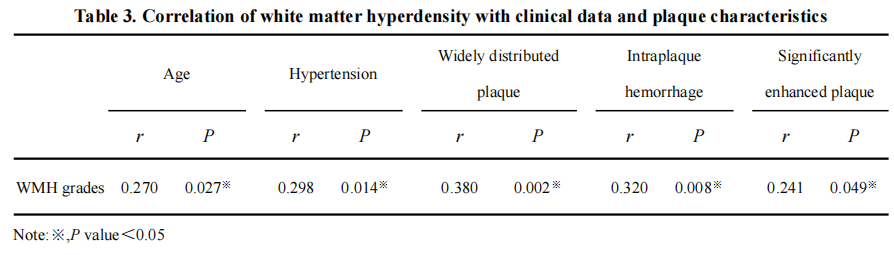
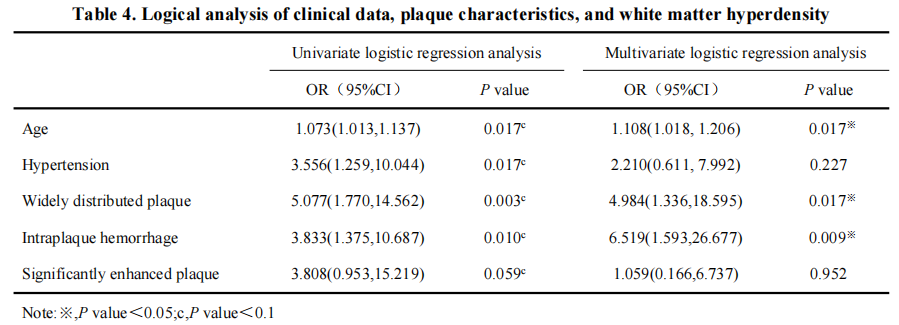
The differences between the two groups in terms of gender, BMI, diabetes mellitus, dyslipidemia, and smoking were not statistically significant(P>0.05). The difference between the two groups in terms of age and hypertension was statistically significant (P<0.05), as shown in Table 1. The comparison of the IPH, widely distributed plaque, and the significantly enhanced plaque between the two groups were significantly different (P=0.009, P=0.002, P=0.048), as shown in Table 2. Spearman correlation analysis showed that WMH grade was positively correlated with age, hypertension, IPH, widely distributed plaque, and significantly enhanced plaque (r=0.270, 0.298, 0.320, 0.390, 0.241, P<0.05), as shown in Table 3. Multivariate logistic regression analysis showed that age, widely distributed plaque, and intraplaque hemorrhage were independent risk factors for WMH [OR (95% CI), P] [1.108 (1.018, 1.206), P = 0.017; 4.984 (1.336, 18.595), P = 0.017; 6.519 (1.593, 26.677), P = 0.09], and See Table 4.Discussion
WMH is usually detected during physical examination, and relevant studies have shown that age and hypertension are important factors for WMH 5. The WMH groups in this experiment have a correlation with age and hypertension, which is consistent with the findings of previous studies6-7. Vulnerable plaques are unstable plaques typically characterized by imaging features such as thin or incomplete fibrous caps, large lipid cores, positive remodeling, IPH or thrombosis, neovascularization or plaque enhancement, and large plaque load 8. Wang et al. demonstrated that carotid intraplaque hemorrhage is independently associated with WMH exacerbation, as assessed by contrast enhancement of intraplaque neovascularization using a semiquantitative visual grading scale 9. Our study showed that plaque significant enhancement was significantly higher in the moderate and severe WMH group than in the no and mild WMH group, which may be attributed to the increase in vascular permeability, which further damages the cerebral white matter. Zhu et al. explored the plaque characteristics of small subcortical infarcts and large subcortical infarcts in the MCA and found that the extent of plaque distribution was more restricted in the small infarct group 10. Wide plaques may represent intraplaque microvascular infiltration and active inflammation, all of which lead to increased shear forces, resulting in irregularities and mechanical vulnerability of the plaque surface.Conclusion
The severity of WMH is related to age, hypertension, wide distribution, intraplaque hemorrhage, and significantly enhanced plaque. Age, wide distribution, and intraplaque hemorrhage are important factors affecting the severity of WMH.Acknowledgements
All authors of this abstract declare that they have no conflict of interest with any organization or individual.
References
1. Lindenholz A, de Bresser J, van der Kolk AG, et al. Intracranial Atherosclerotic Burden and Cerebral Parenchymal Changes at 7T MRI in Patients with Transient Ischemic Attack or Ischemic Stroke[J]. Front Neurol. 2021; 12:637556.
2. Delano-Wood L, Bondi MW, Sacco J, et al. Heterogeneity in mild cognitive impairment: differences in neuropsychological profile and associated white matter lesion pathology[J]. J Int Neuropsychol Soc. 2009;15(6):906-914.
3. Fazekas F, Chawluk JB, Alavi A, et al MR signal abnormalities at 1.5 T in Alzheimer's dementia and normal aging[J]. Am J Neuroradiol, 1987, 8:421-426.
4. Wang JN, Börnert P, Zhao HL et al. Simultaneous non-contrast angiography and intraplaque hemorrhage (SNAP) imaging for carotid atherosclerotic disease evaluation. [J]. Magn Reson Med, 2013, 69: 337-45.
5.Fang M, Feng C, Xu Y, et al. Microbleeds and silent brain infarctions are differently associated with cognitive dysfunction in patients with advanced periventricular leukoaraiosis[J]. Int J Med Sci. 2013;10(10):1307-1313.
6.Keller J, Kant I, Slooter A, et al. Different cardiovascular risk factors are related to distinct white matter hyperintensity MRI phenotypes in older adults. [J]. Neuroimage Clin, 2022, 35: 103131.
7. Nam KW, Kwon HM, Jeong HY, et al. Cerebral white matter hyperintensity is associated with intracranial atherosclerosis in a healthy population[J].Atherosclerosis,2017:179-183.
8. Naghavi M, Libby P, Falk E, et al. From vulnerable plaque to vulnerable patient: a call for new definitions and risk assessment strategies: Part I.[J]. Circulation, 2003, 108: 1664-72.
9.Wang Y, Jiang C, Huang H, et al. Correlation of Cerebral White Matter Lesions with Carotid Intraplaque Neovascularization assessed by Contrast-enhanced Ultrasound.[J]. J Stroke Cerebrovasc Dis. 2020;29(8):104928.
10.Zhu TT, Ren LJ, Zhang Lei, et al. Comparison of plaque characteristics of small and large subcortical infarctions in the middle cerebral artery territory using high-resolution magnetic resonance vessel wall imaging. [J]. Quant Imaging Med Surg, 2021, 11: 57-66.
Figures
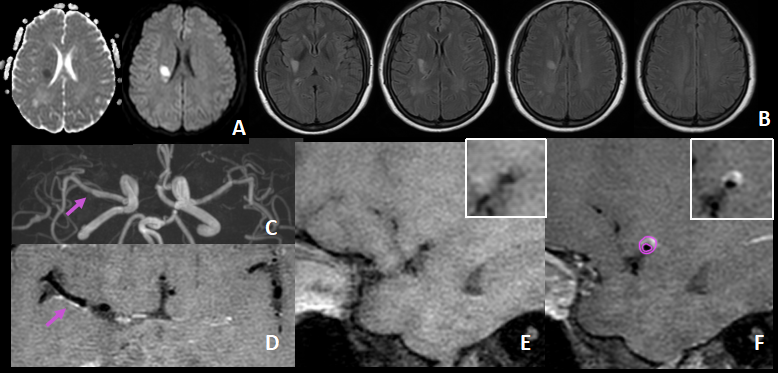
Figure 1: A patient with mild white matter hyperintensities
A female patient with acute ischemic stroke, 55 years old. The right basal ganglia region has restricted diffusion (A); a "hat-shaped" high signal in the anterior horns of the lateral ventricles bilaterally (B); an arrow on the MIP image shows mild stenosis in the M1 segment (c); post-enhancement long-axis T1 VISTA image suggesting increased plaque signal along the M1 (D); pre-enhancement (E) and post-enhancement (F) short-axis T1 VISTA shows limited distribution of plaques and non-significant enhancement of the plaques.