4917
The clinical application of 5.0 T 3D TOF MRA in the imaging of AChA and related cerebrovascular diseases1Shandong Provincial Third Hospital, Cheeloo College of Medicine, Shandong University, JINAN, China, 2Department of Radiology, Shandong Provincial Third Hospital, Cheeloo College of Medicine, Shandong University, Jinan, China, 3Department of Radiology, Shandong Provincial Third Hospital, Cheeloo College of Medicine, Shandong University, JINAN, China, 4United Imaging Research Institute of Intelligent Imaging, Beijing, People’s Republic of China, Beijing, China
Synopsis
Keywords: Vascular, Brain, magnetic resonance imaging; TOF MRA; Anterior choroidal artery AChA; 5.0 T
Motivation: Improved cerebrovascular disease diagnosis requires enhanced imaging of the anterior choroidal artery (AChA).
Goal(s): To evaluate the effectiveness of a 5.0T ultra-high-field MR scanner for cerebrovascular imaging compared to traditional 3.0T scanners.
Approach: Retrospective analysis using 5.0T MR imaging to assess AChA visualization in patients with cerebrovascular complaints.
Results: The 5.0T scanner significantly outperformed the 3.0T in image quality and detail, providing superior AChA delineation, which is essential for diagnosing related cerebrovascular diseases.
Impact: The 5.0T MR imaging's superior visualization of AChA paves the way for better diagnosis and management of deep brain vascular diseases, potentially influencing treatment outcomes and advancing neurovascular research.
Introduction
The anterior choroidal artery (AChA), despite its small size, is integral for brain motor and sensory functions. Infarcts in the AChA territory, particularly affecting the internal capsule, can cause the AChA syndrome - leading to severe motor and sensory deficits. Traditional magnetic resonance angiography (MRA) techniques often fail to depict the AChA clearly due to its size and complex location. Time-of-flight (TOF) MRA, however, offers a non-invasive, higher resolution alternative without the use of contrast agents. Although 7.0T MR provides even greater detail, its high cost and limited scope of application restrict its clinical use. This study aims to assess the effectiveness of 5.0T TOF MRA for depicting the AChA to aid in the diagnosis and treatment of cerebrovascular diseases, addressing a previously unexplored area of research.Method
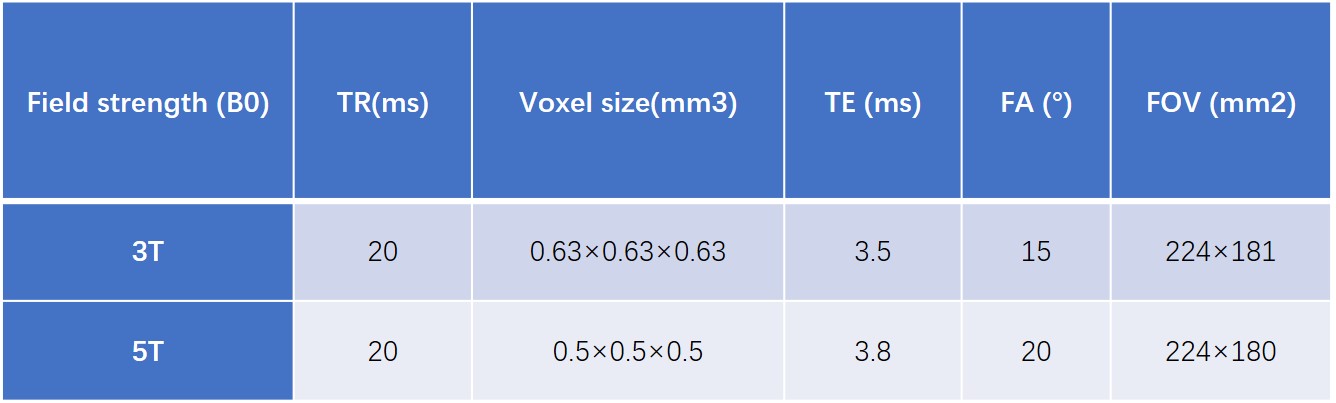
This retrospective study included 80 patients who presented with headache, dizziness, hemisensory disturbances, or focal epilepsy between May 15 and August 1, 2023. They were divided into two groups for imaging: 42 underwent 3.0T MR (Ingenia, Philips), and 38 underwent 5.0T MR (uMR Jupiter, United Imaging Healthcare), with two patients receiving both scans within 24 hours. Exclusions were made for those with aneurysm surgery, cerebral hemorrhage, heart surgery, or those pregnant, planning pregnancy, lactating, or with claustrophobia. TOF MRA was conducted with parameters detailed in Table 1, differing slightly between the 3.0T and 5.0T MR groups to optimize image quality. Images underwent 3D reconstruction, and cerebral arteries were analyzed through maximum intensity projections. Two experienced radiologists, blinded to field strength, evaluated image quality using the Likert 5 scale and counted visible branches. SNR and CNR were calculated for quantitative analysis. Statistical analysis employed SPSS 25.0, utilizing T-tests or Mann-Whitney U tests for parametric and non-parametric data, respectively, with chi-square tests for categorical data. Inter- and intra-observer reliability was determined using the intraclass correlation coefficient (ICC), with a threshold of 0.75 for good consistency. Statistical significance was defined at p<0.05.Result
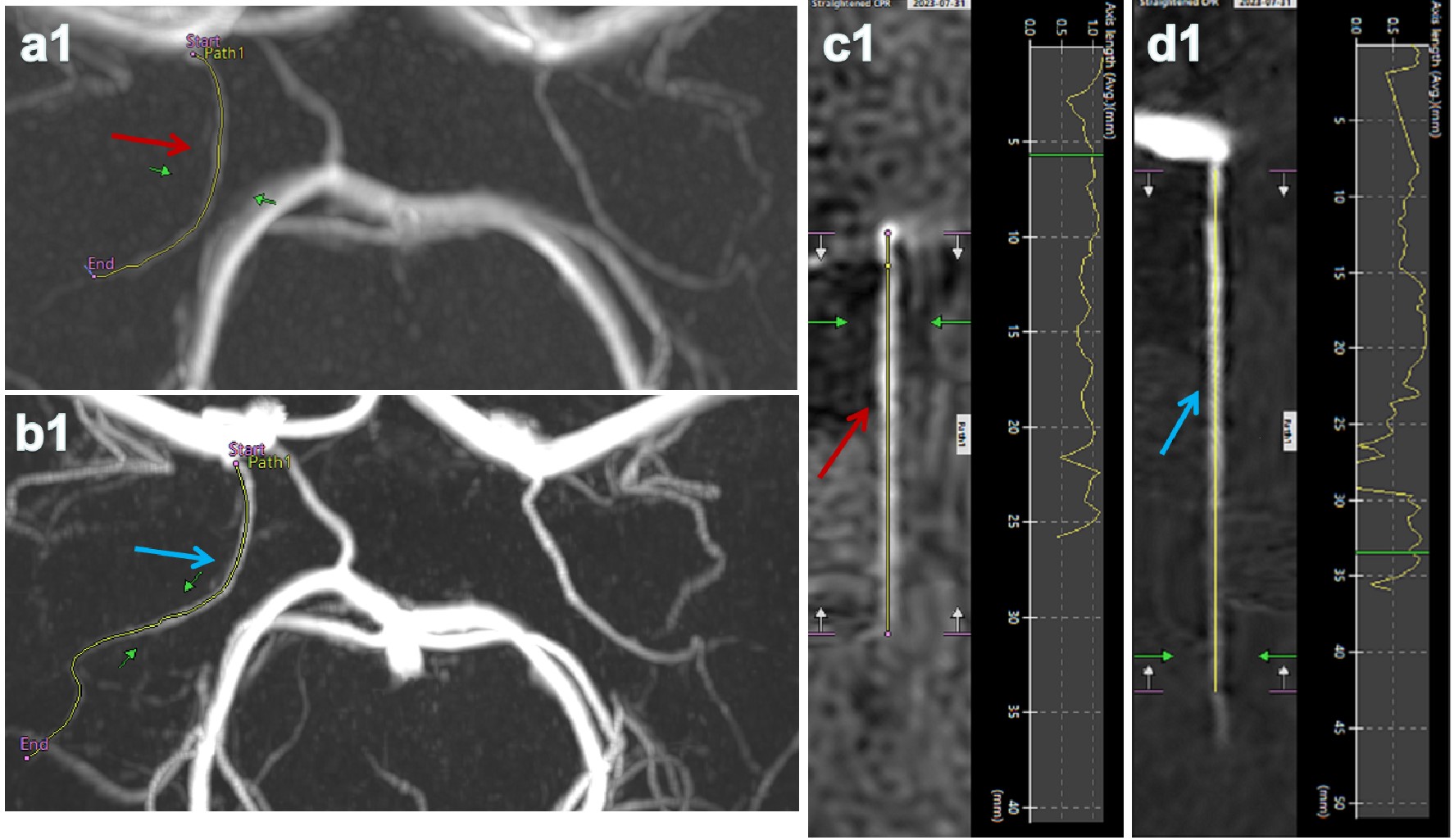
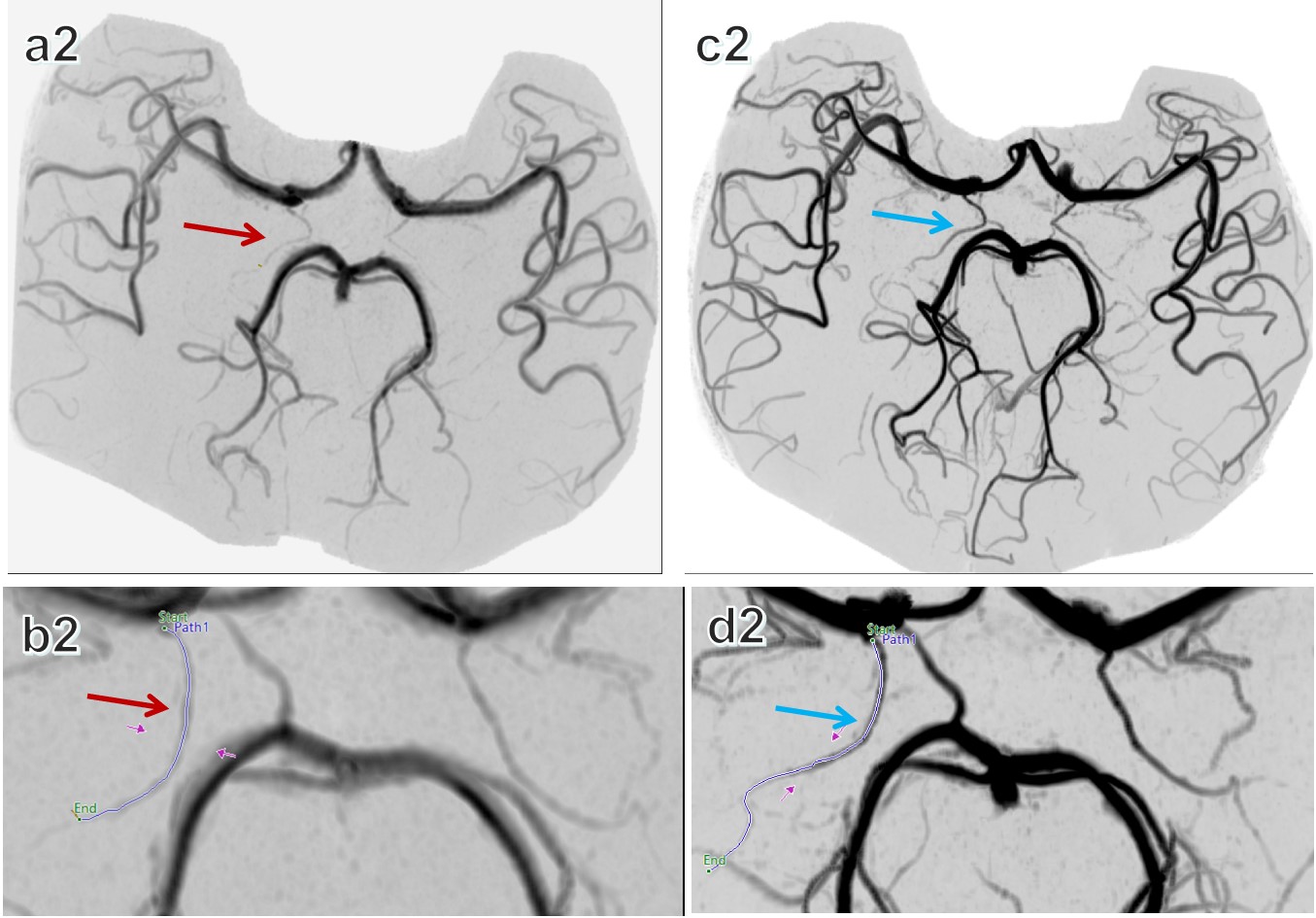
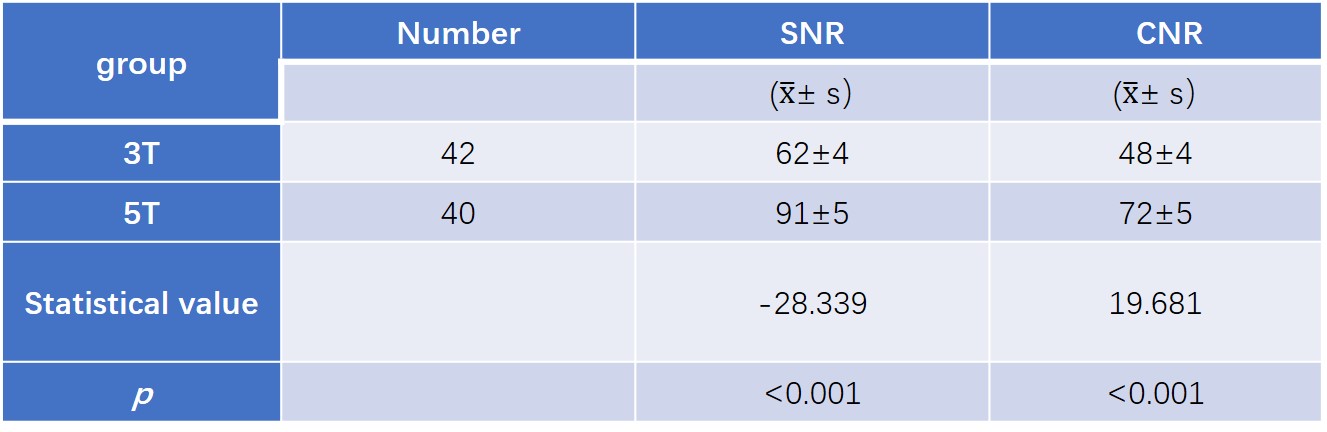
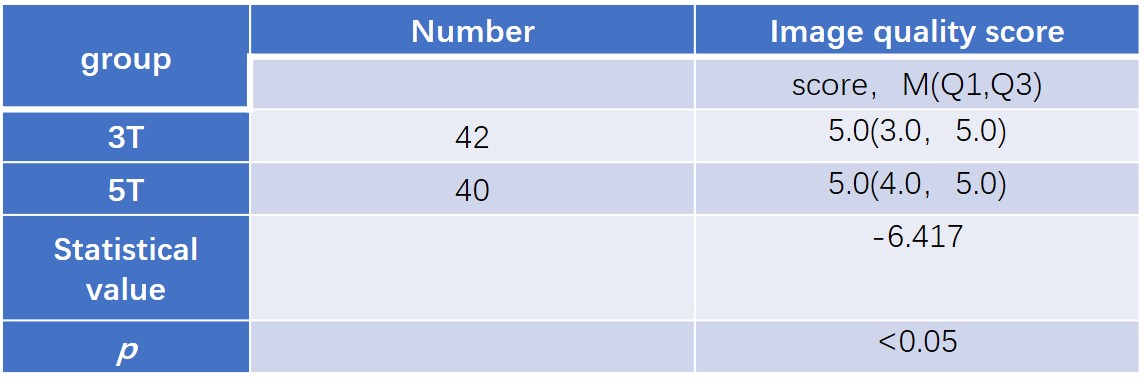
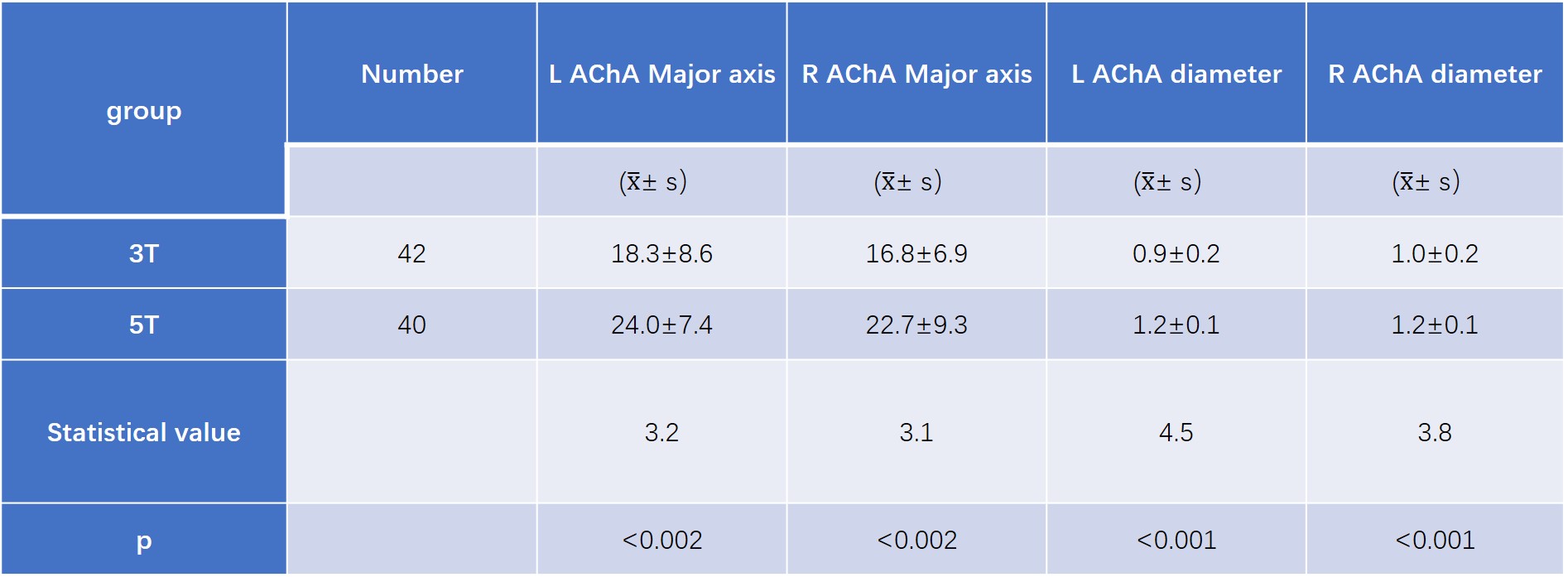
This study comprised 80 participants (37 males and 43 females, age range 12-87 years, mean age 59). It included 42 patients in the 3.0T group (23 males, 19 females, mean age 59.4) and 38 in the 5.0T group (16 males, 24 females, mean age 60.5). Age and gender distributions between groups were statistically comparable (P > 0.05). Inter- and intra-physician assessments demonstrated strong consistency in image and vascular quality evaluations (ICC between 0.93 and 0.99). In the 3.0T group, observations included 84 AChA-A1 segments, 56 AChA-A2, and 20 AChA-A3. The 5.0T group had 80 AChA-A1, 80 AChA-A2, and 60 AChA-A3 segments observed. SNR and CNR values were significantly higher in the 5.0T group compared to the 3.0T group (P < 0.05), and the subjective image quality rating also significantly differed between groups (P < 0.05). TOF MRA images from both groups showed significantly improved visualization of the anterior choroidal artery's length and diameter compared to standard 3.0T MR imaging (P < 0.05). These findings are detailed in Table 4 and illustrated in Figure 1 and Figure 2.Discussion
This retrospective study compared the image quality and vessel delineation of TOF MRAs between 3.0T and 5.0T MR imaging, revealing that the 5.0T provided significantly higher SNR and CNR. Particularly, the 5.0T system offered superior visualization of the anterior choroidal artery, enhancing the detail of intracranial vessels, and thereby improving non-invasive vascular imaging for cerebrovascular disease assessment. The anterior choroidal artery is vital for supplying various brain regions; thus, its clear imaging is crucial for diagnosing related infarcts, which may lead to severe neurological symptoms. The 5.0T MR's enhanced capabilities not only yield better image quality but also facilitate more accurate diagnosis of small vessel diseases, aiding in the management of conditions like moyamoya syndrome and potentially improving outcomes for neurodegenerative diseases and stroke. Despite these advancements, this study's limitations include its single-center nature and the absence of a 7.0T control group, indicating a need for more comprehensive, multi-center studies to validate these findings.Conclusion
This study showcases the application of a 5.0T ultra-high-field MR scanner for comprehensive cerebrovascular assessment, marking a significant stride in the diagnosis and differentiation of cerebrovascular conditions. It underscores the clinical value of detailed AChA visualization, which is crucial for diagnosing conditions like moyamoya disease, hippocampal sclerosis, and Parkinson's disease. The 5.0T system surpasses the limitations of 7.0T scanners for whole-body scans and outperforms 3.0T in visualizing deep brain vascular structures, offering substantial support for clinical diagnosis and management of cerebrovascular diseases.Acknowledgements
Conflict of interest The authors state no conflict of interest.References
[1] Satoshi,Tsutsumi,Hideo,et al.The cisternal segment of the anterior choroidal artery: an anatomical study using magnetic resonance imaging[J].Child's Nervous System, 2017, 33(11):1-6.DOI:10.1007/s00381-017-3525-8.
[2] Ma L , Feng H , Yan S ,et al.Endovascular Treatment of Complex Vascular Diseases of the Internal Carotid Artery Using the Willis Covered Stent: Preliminary Experience and Technical Considerations[J].Frontiers in Neurology, 2020, 11:554988-.DOI:10.3389/fneur.2020.554988.
[3] Li Xiao, Guan Yongsong, Zhou Xiangping, et al. Cerebral artery DSA morphological analysis and its implications [J]. Chinese journal of clinical anatomy, 2005, 23 (3) : 4. DOI: 10.3969 / j.i SSN. 1001-165 - x. 2005.03.007.
[4] Park C A , Kang C K , Kim Y B ,et al.Advances in MR angiography with 7T MRI From microvascular imaging to functional angiography.[J].NeuroImage, 2017:S1053811917300198.DOI:10.1016/j.neuroimage.2017.01.019.
[5] Fagan AJ, Bitz AK, Björkman-Burtscher IM, et al. 7T MR Safety. J Magn Reson Imaging. 2021;53(2):333-346. doi:10.1002/jmri.27319
[6] Wang TH, Jingami N, Okada T, Yunoki T, Ohtsuru S, Koike K. Anterior Choroidal Artery Infarction Evaluated with 123I-Imp Single-Photon Emission Computed Tomography and 7 Tesla Magnetic Resonance Imaging. J Stroke Cerebrovasc Dis. 2019 May;28(5):e51-e52. doi: 10.1016/j.jstrokecerebrovasdis.2019.02.007. Epub 2019 Mar 9. PMID: 30862395.
[7] Hamoir XL, Grandin CB, Peeters A, Robert A, Cosnard G, Duprez T. MRI of hyperacute stroke in the AChA territory. Eur Radiol. 2004;14(3):417-424. doi:10.1007/s00330-003-2220-1
[8] De Cocker LJ, Lindenholz A, Zwanenburg JJ, van der Kolk AG, Zwartbol M, Luijten PR, Hendrikse J. Clinical vascular imaging in the brain at 7T. Neuroimage. 2018 Mar;168:452-458. doi: 10.1016/j.neuroimage.2016.11.044.
[9] Zhang Z, Fan Z, Kong Q, Xiao J, Wu F, An J, Yang Q, Li D, Zhuo Y. Visualization of the lenticulostriate arteries at 3T using black-blood T1-weighted intracranial vessel wall imaging: comparison with 7T TOF-MRA. Eur Radiol. 2019 Mar;29(3):1452-1459. doi: 10.1007/s00330-018-5701-y. Epub 2018 Aug 27. PMID: 30151642.
[10] Spincemaille P , Anderson J , Wu G ,et al.Quantitative Susceptibility Mapping: MRI at 7T versus 3T[J].Journal of Neuroimaging, 2020(2).DOI:10.1111/jon.12669.
[11] Shi Zhang, Miao Xiyin, Zhu Shuo, et al. Clinical 5.0 T ultra high field MRI assessment of the value of the cerebral artery and its branches [J]. Chinese journal of radiology, 2022, 56 (8) : 886-891. The DOI: 10.3760 / cma. J.c. n112149-20211224-01142
[12] Rutland JW, Delman BN, Gill CM, Zhu C, Shrivastava RK, Balchandani P. Emerging Use of Ultra-High-Field 7T MRI in the Study of Intracranial Vascularity: State of the Field and Future Directions. AJNR Am J Neuroradiol. 2020;41(1):2-9. doi:10.3174/ajnr.A6344
[13] Spitz L , Gaidzik F , Stucht D ,et al.A hybrid hierarchical strategy for registration of 7T TOF-MRI to 7T PC-MRI intracranial vessel data[J].International journal of computer assisted radiology and surgery, 2023.DOI:10.1007/s11548-023-02836-y.
[14] Liu J , Chen F , Wang X ,et al.A Comparative Analysis Framework of 3T and 7T TOF- MRA Based on Automated Cerebrovascular Segmentation[J].Computerized Medical Imaging and Graphics, 2021(9):101830.DOI:10.1016/j.compmedimag.2020.101830.
[15] Leemans E , Cornelissen B , Sing M L C ,et al.7T versus 3T MR Angiography to Assess Unruptured Intracranial Aneurysms[J].Journal of Neuroimaging, 2020.DOI:10.1111/jon.12772.
[16] Bhogal P, Ganslandt O, Bäzner H, Henkes H, Aguilar Perez M. Treatment of Unruptured, Saccular, Anterior Choroidal Artery Aneurysms with Flow Diversion : A Single Centre Experience. Clin Neuroradiol. 2019;29(3):459-465. doi:10.1007/s00062-018-0677-1
[17] Shah AU, Joshi AR, Rai PR, Kapse P. Hyperplastic Anterior Choroidal Artery-A Rare Variant Detected on MR Angiography. Indian J Radiol Imaging. 2022;32(2):266-269. Published 2022 Jun 9. doi:10.1055/s-0042-1744231
[18] Zhang C, Shi J. 7T MRI for Intracranial Vessel Wall Lesions and Its Associated Neurological Disorders: A Systematic Review. Brain Sci. 2022 Apr 21;12(5):528. doi: 10.3390/brainsci12050528.
[19] Guo X, Gao L, Yu H, et al. Computed tomographic angiography may be used for assessing the dilatation of the anterior choroidal and posterior communicating arteries in patients with moyamoya syndrome. Eur Radiol. 2021;31(8):5544-5551. doi:10.1007/s00330-021-07722-2
[20] Opheim G, van der Kolk A, Markenroth Bloch K, et al. 7T Epilepsy Task Force Consensus Recommendations on the Use of 7T MRI in Clinical Practice. Neurology. 2021;96(7):327-341. doi:10.1212/WNL.0000000000011413
[21] Platt T , Ladd M E , Paech D .7 Tesla and Beyond: Advanced Methods and Clinical Applications in Magnetic Resonance Imaging[J].Investigative Radiology, 2021, Publish Ahead of Print.DOI:10.1097/RLI.0000000000000820.
[22] Okada T, Fujimoto K, Fushimi Y, Akasaka T, Thuy DHD, Shima A, Sawamoto N, Oishi N, Zhang Z, Funaki T, Nakamoto Y, Murai T, Miyamoto S, Takahashi R, Isa T. Neuroimaging at 7 Tesla: a pictorial narrative review. Quant Imaging Med Surg. 2022 Jun;12(6):3406-3435. doi: 10.21037/qims-21-969.
[23] Alves IS, Coutinho AMN, Vieira APF, et al. Imaging Aspects of the Hippocampus. Radiographics. 2022;42(3):822-840. doi:10.1148/rg.210153.
[24] Li Hongcui, Li Xiao, Tang Chengwei, et al. Before the choroid artery anatomy and clinical significance of the research progress of [J]. Journal of anatomy and clinical, 2010 (1) : 3. DOI: 10.3969 / j.i SSN. 1671-7163.2010.01.019.
Figures
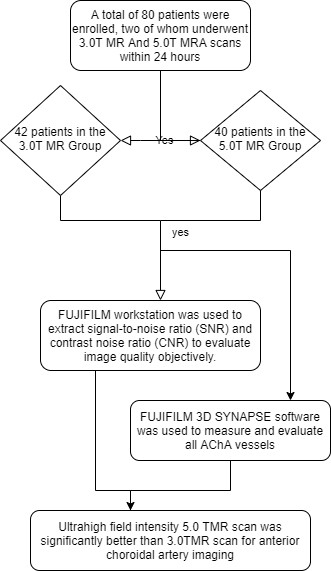
Figure 1.Comparison flow chart of 3.0T and 5.0TMR anterior choroidal artery imaging.