4913
Prognostic Value of Right Ventricular 3D Trabecular Complexity in Arrhythmogenic right ventricular cardiomyopathy1RenJi Hospital, School of Medicine, Shanghai Jiao Tong University, Shanghai, China, 2Philips Healthcare, shanghai, China, 3Philips Healthcare, Xi'an, Shaanxi, China, 4Beijing Anzhen Hospital, Capital Medical University, Beijing, China
Synopsis
Keywords: Myocardium, Cardiovascular
Motivation: Arrhythmogenic right ventricular cardiomyopathy (ARVC) is characterized by progressive myocardial fibro-fatty infiltration accompanied by trabecular disarray. The prognostic value of trabecular disorder assessed by three-dimensional (3D) fractal dimension (FD) measurement is unclear.
Goal(s): To investigate the prognostic value of 3D right ventricular trabecular complexity of ARVC.
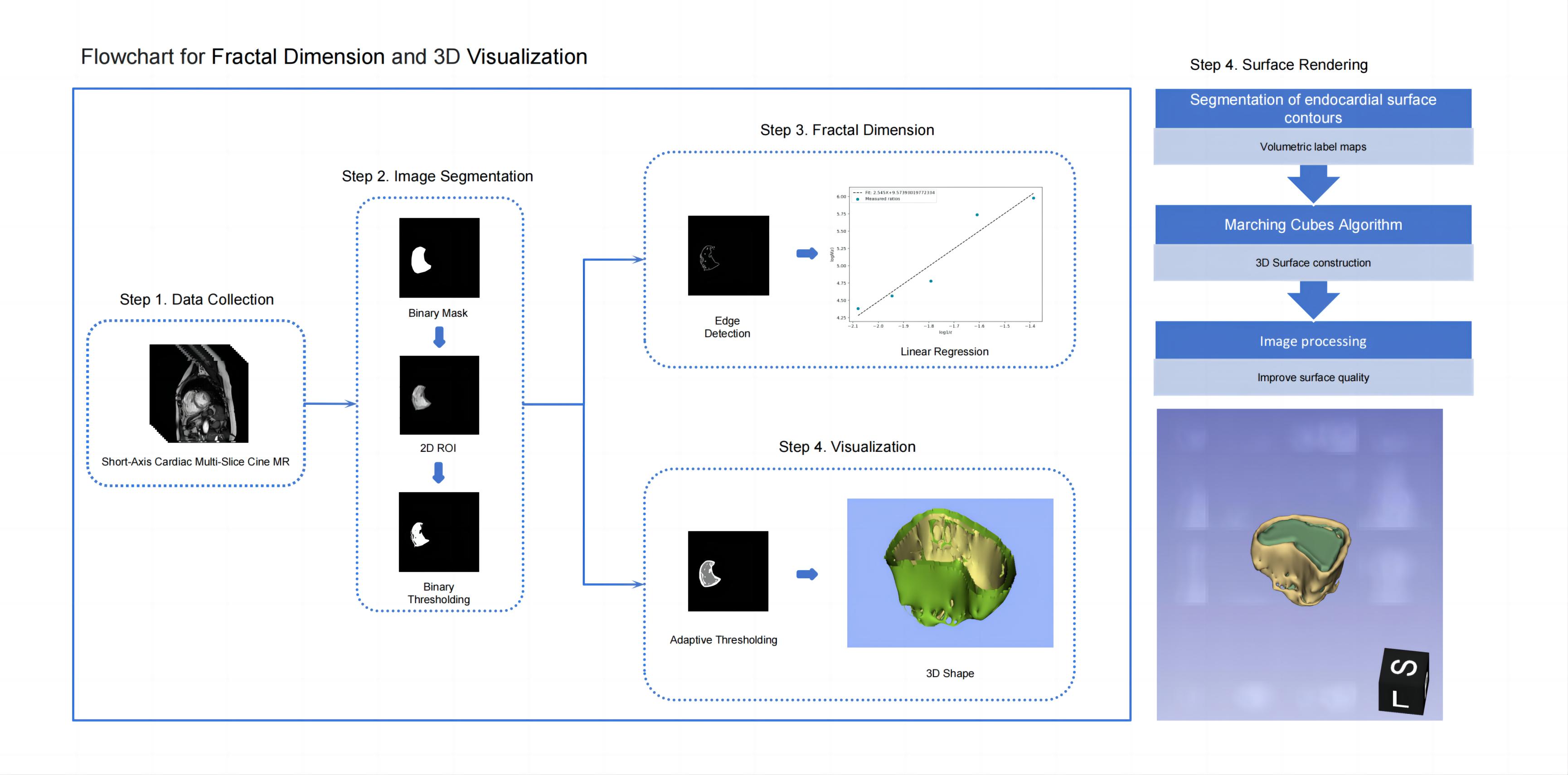
Approach: Using cine images, trabecular complexity was measured with 3D fractal analysis to calculate 3D-FD in ARVC patients retrospectively. Cox regression analyses and Kaplan-Meier survival analysis were performed to identify the prognostic value of 3D-FD.
Results: RV 3D-FD was a significant risk predictor for MACE in ARVC and provided incremental prognostic value to conventional predictors.
Impact: Based on the results, we suggested 3D RV trabecular complexity, derived from non-invasive imaging examination, as a new biomarker for early clinical therapy in medication and ICD implantation in order to moderate the onset of adverse endpoints in ARVC patients.
Background
Arrhythmogenic right ventricular cardiomyopathy (ARVC) is characterized by progressive myocardial fibro-fatty infiltration accompanied by trabecular disarray. Two-dimensional (2D) fractal dimension (FD) analysis was conventionally utilized to evaluate trabecular disarray. While the prognostic value of trabecular disorder assessed by three-dimensional (3D) fractal dimension (FD) measurement is unclear.Purpose
To investigate the prognostic value of right ventricular trabecular complexity using 3D fractal dimension analysis based on CMR cine images in participants with ARVC.Materials and Methods
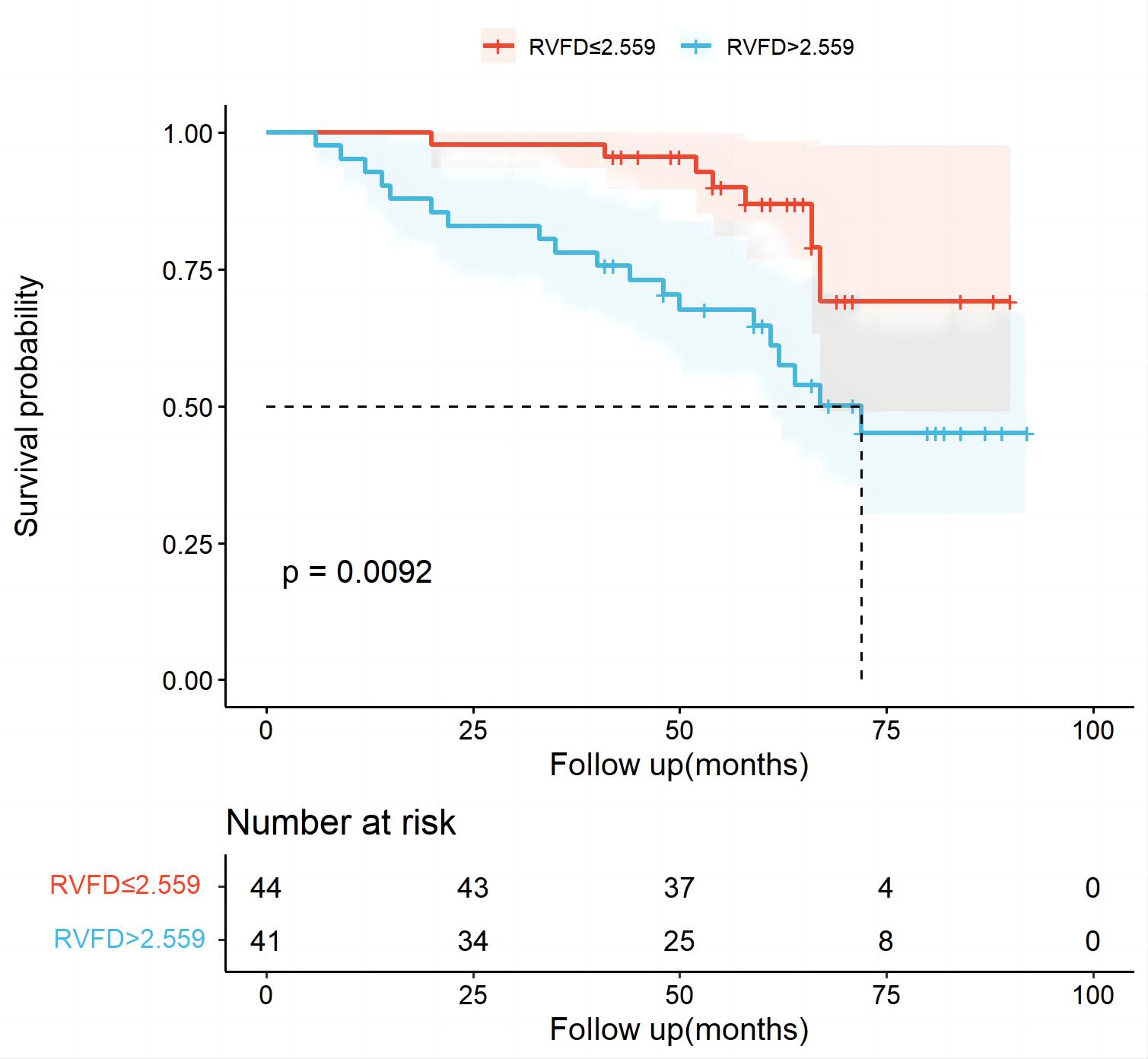
In this retrospective research, participants with ARVC who underwent CMR examination between May 2013 and May 2022 from2 sites were included. Using cine images, trabecular complexity was measured with three-dimensional (3D) fractal analysis to calculate 3D fractal dimension (FD). Major adverse cardiac events (MACE) were defined as a combination of aborted cardiac arrest, sudden cardiac arrest, and appropriate implantable cardioverter-defibrillator (ICD) intervention. Cox regression analyses and Kaplan-Meier survival analysis were performed to identify the prognostic value of 3D-FD.Results
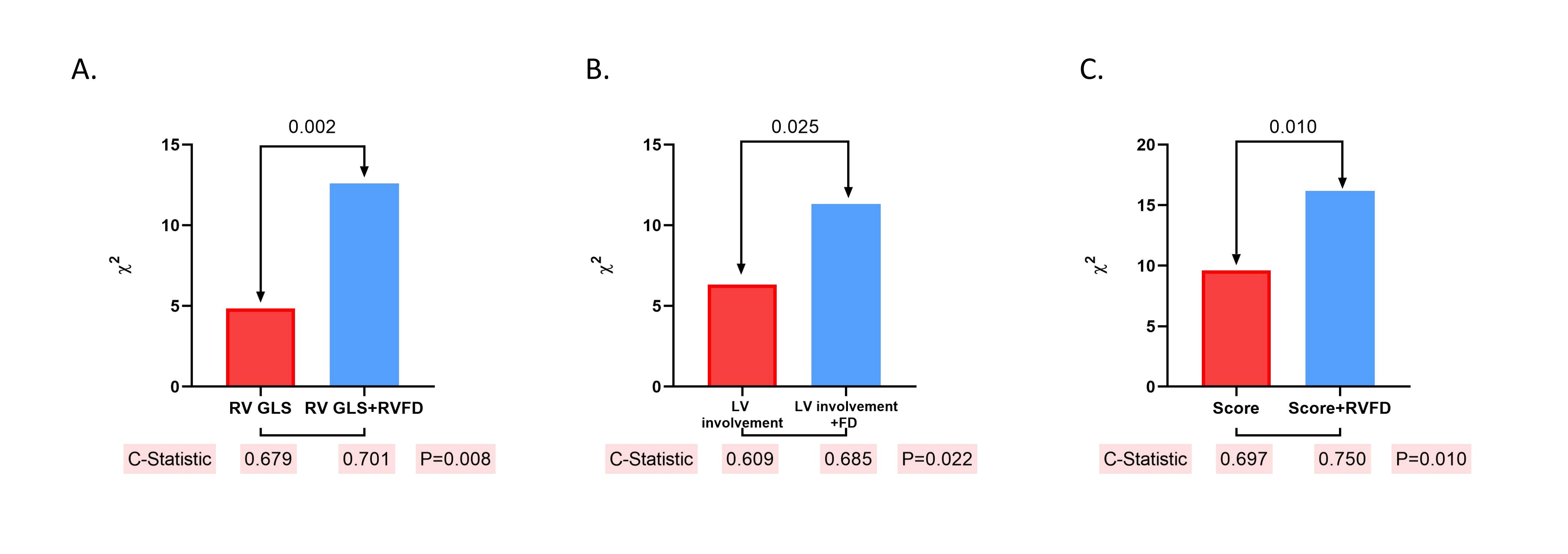
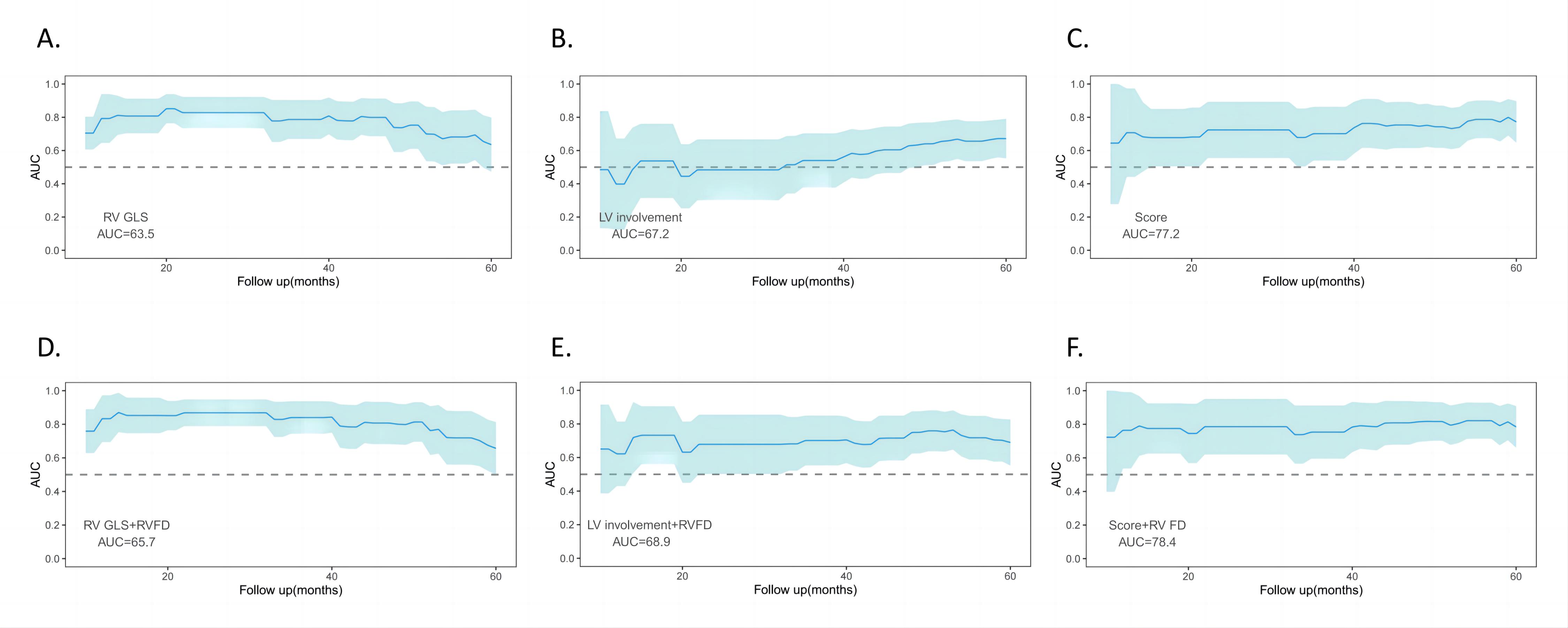
A total of 85 ARVC patients (median age: 49 years, interquartile range: 31–58 years; 52 male) were included, with 26 MACE recorded during the 60 month follow-up (interquartile range: 48- 67 months) after the CMR examination. RV 3D-FD differed between ARVC patients with and without MACE (2.67, interquartile range:2.51~2.81 vs 2.52, interquartile range:2.40~2.67, P<0.01). In multivariable Cox analysis, RV 3D-FD was suggested as a significant risk predictor for MACE in ARVC patients (hazard ratio, 1.02; 95% confidence interval:1.01, 1.04; P=0.01). In addition, prognostic model fitness was improved after adding 3D-FD to RV global longitudinal strain, LV involvement, and 5-year risk score separately (all P<0.05).Conclusion
The myocardial trabecular complexity assessed through 3D fractal dimension analysis was found to be associated with MACE and provided incremental prognostic value beyond conventional ARVC risk predictors.Acknowledgements
No acknowledgement found.References
1. Iyer VR, Chin AJ. Arrhythmogenic right ventricular cardiomyopathy/dysplasia (ARVC/D). Am J Med Genet C Semin Med Genet 2013;163c(3):185-197. doi: 10.1002/ajmg.c.31368
2. Kirkels FP, Lie Ø H, Cramer MJ, Chivulescu M, Rootwelt-Norberg C, Asselbergs FW, Teske AJ, Haugaa KH. Right Ventricular Functional Abnormalities in Arrhythmogenic Cardiomyopathy: Association With Life-Threatening Ventricular Arrhythmias. JACC Cardiovasc Imaging 2021;14(5):900-910. doi: 10.1016/j.jcmg.2020.12.028
3. Molinari G, Sardanelli F, Gaita F, Ottonello C, Richiardi E, Parodi RC, Masperone MA, Caponnetto S. Right ventricular dysplasia as a generalized cardiomyopathy? findings on magnetic resonance imaging. Eur Heart J 1995;16(11):1619-1624. doi: 10.1093/oxfordjournals.eurheartj.a060786
4. Petersen SE, Jensen B, Aung N, Friedrich MG, McMahon CJ, Mohiddin SA, Pignatelli RH, Ricci F, Anderson RH, Bluemke DA. Excessive Trabeculation of the Left Ventricle: JACC: Cardiovascular Imaging Expert Panel Paper. JACC: Cardiovascular Imaging 2023;16(3):408-425. doi: https://doi.org/10.1016/j.jcmg.2022.12.026
5. Dawes TJW, Cai J, Quinlan M, de Marvao A, Ostrowski PJ, Tokarczuk PF, Watson GMJ, Wharton J, Howard L, Gibbs JSR, Cook SA, Wilkins MR, O'Regan DP. Fractal Analysis of Right Ventricular Trabeculae in Pulmonary Hypertension. Radiology 2018;288(2):386-395. doi: 10.1148/radiol.2018172821
6. Camporeale A, Moroni F, Lazzeroni D, Garibaldi S, Pieroni M, Pieruzzi F, Lusardi P, Spada M, Mignani R, Burlina A, Carubbi F, Econimo L, Battaglia Y, Graziani F, Pica S, Chow K, Camici PG, Lombardi M. Trabecular complexity as an early marker of cardiac involvement in Fabry disease. Eur Heart J Cardiovasc Imaging 2022;23(2):200-208. doi: 10.1093/ehjci/jeaa354
7. Zheng T, Ma X, Li S, Ueda T, Wang Z, Lu A, Zhou W, Zou H, Zhao L, Gong L. Value of Cardiac Magnetic Resonance Fractal Analysis Combined With Myocardial Strain in Discriminating Isolated Left Ventricular Noncompaction and Dilated Cardiomyopathy. J Magn Reson Imaging 2019;50(1):153-163. doi: 10.1002/jmri.26616
8. Tandri H, Calkins H, Nasir K, Bomma C, Castillo E, Rutberg J, Tichnell C, Lima JA, Bluemke DA. Magnetic resonance imaging findings in patients meeting task force criteria for arrhythmogenic right ventricular dysplasia. J Cardiovasc Electrophysiol 2003;14(5):476-482. doi: 10.1046/j.1540-8167.2003.02560.
9. Captur G, Muthurangu V, Cook C, Flett AS, Wilson R, Barison A, Sado DM, Anderson S, McKenna WJ, Mohun TJ, Elliott PM, Moon JC. Quantification of left ventricular trabeculae using fractal analysis. J Cardiovasc Magn Reson 2013;15(1):36. doi: 10.1186/1532-429x-15-36
10. Lopes R, Betrouni N. Fractal and multifractal analysis: a review. Med Image Anal 2009;13(4):634-649. doi: 10.1016/j.media.2009.05.003
11. Corral Acero J, Schuster A, Zacur E, Lange T, Stiermaier T, Backhaus SJ, Thiele H, Bueno-Orovio A, Lamata P, Eitel I, Grau V. Understanding and Improving Risk Assessment After Myocardial Infarction Using Automated Left Ventricular Shape Analysis. JACC Cardiovasc Imaging 2022;15(9):1563-1574. doi: 10.1016/j.jcmg.2021.11.027
Figures