4911
4D flow CMR-derived left ventricular hemodynamic indicators for evaluating heart failure with reduced ejection fraction patients1Department of Radiology, Beijing Anzhen Hospital, Capital Medical University, Beijing, China, 2Philips Healthcare, Beijing, China
Synopsis
Keywords: Heart Failure, Cardiovascular
Motivation: Heart failure is a clinical syndrome in which the heart is unable to pump blood efficiently, and Heart Failure with Reduced Ejection Fraction (HFrEF) with the left ventricular ejection fraction (LVEF) < 40% serve as high morbidity and mortality.
Goal(s): The aim of this study is to investigate the hemodynamic environment in left ventricle of different phases.
Approach: 4D flow technology could offer non-invasive method for quantifying the alternatives of intracardiac blood flow components in HFrEF with and without MACE.
Results: Results showed reduced DF-KEiESV, DEF-KEiESV, higher RVo and peak E-wave RVo-KEiEDV were confirmed in MACE+ group when compared with MACE- group.
Impact: The hemodynamic analysis in HFrEF when compared patients with and without MACE illustrated significant alternative of intracardiac blood flow components by using 4D flow technology, which could offer valuable insight for further assessment and treatment planning.
Introduction
Heart failure (HF) is a multifactorial cardiovascular disorder that has garnered attention within the realm of clinical practice, which engenders considerable morbidity and mortality[1]. Furthermore, amid the diverse array of heart failure subtypes, one of the prominently condition characterized by a distinct pathophysiological hallmark is Heart Failure with Reduced Ejection Fraction (HFrEF) with the left ventricular ejection fraction (LVEF) < 40%[1]. Cardiac magnetic resonance imaging (CMR) has been proved an effective standard for offering morphological and functional information[2]. In order to non-invasively assess the hemodynamic environment in the heart, 4D flow has been introduced as a valuable technique for quantitively deriving intracardiac blood flow components, offering profound mechanistic insights into the heart failure patients [3]. Given the lack of anticipatory information concerning CMR 4D flow-derived intracardiac blood flow components and kinetic energy (KE), the aimof this study is to investigate the predictive value of hemodynamic parameters in patients HFrEF.Methods
From May 2019 to May 2022, 420 patients with HF were prospectivly enrolled, who underwent comprehensive CMR examination in our single center study. All sequences were performed by a 3.0T MR platform(Ingenia CX; Philips Healthcare, Best, the Netherlands), including conventional image, 4D flow and late gadolinium enhancement (LGE) sequences. Acquisition parameters of 4D flow were as follows: TR/TE=5.2/2.2 ms, flip angle=8°, slab thickness=70–90 mm, compressed SENSE (CS) factor = 4.6, field of view (FOV) =(225–400) × (255–420) mm2, a non-interpolated spatial resolution = 2.3 × 2.3 × 2.3mm3, and the velocity encoding (VENC) was set at 100-120 cm/s. CVI software was used for postprocessing, it was separated into four components: direct flow (DF), retained inflow (RI), delayed ejection flow (DEF), and residual volume (RVo) for LV intracardiac flow analyse,. Systolic KE and diastolic KE (peak E-wave and peak a-wave) was calculated throughout the cardiac cycle, and the values were normalized to LV end-systolic volume (KEiESV) or end-diastolic volume (KEiEDV), respectively. Intracardiac flow was classified into four functional components[14] as described previously: (1) direct flow (DF); (2) retained inflow (RI); (3) delayed ejection flow (DEF); and (4) residual volume (RVo)[4]( Figure 1). Patients were divided into two groups according to major adverse cardiac events (MACEs), including cardiac-related death, rehospitalization, cardiac resynchronization therapy [CRT-D], implantable cardioverter defibrillator [ICD], or revascularization were defned as primary clinical endpoint. Statistical analysis was performed using SPSS statistical software version 22.0 (SPSS Inc, Chicago, IL, USA). Characteristics were summarized with continuous variables expressed as means ± SD and categorical variables presented as frequencies and percentages. P value < 0.05 was considered statistically significant.Results
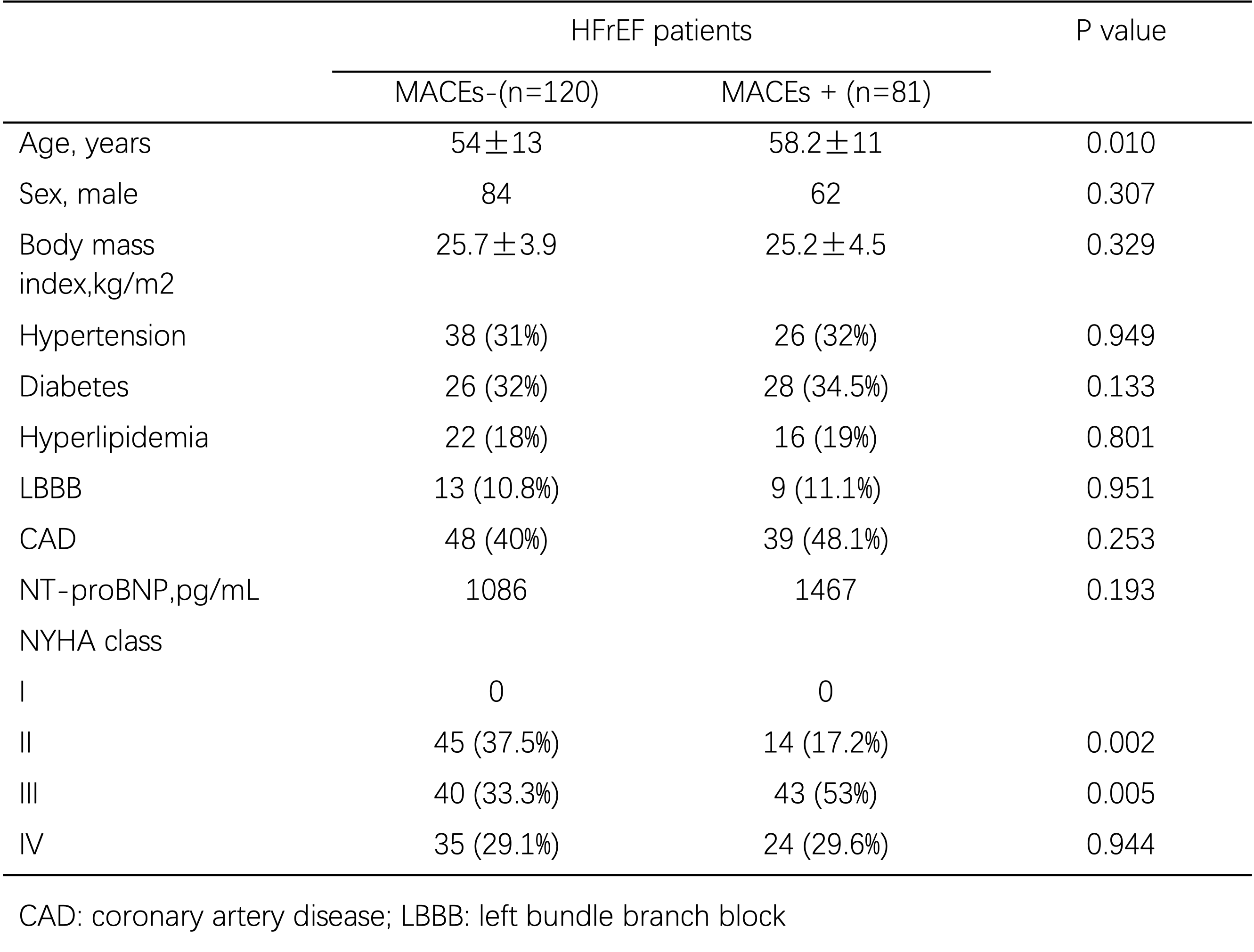
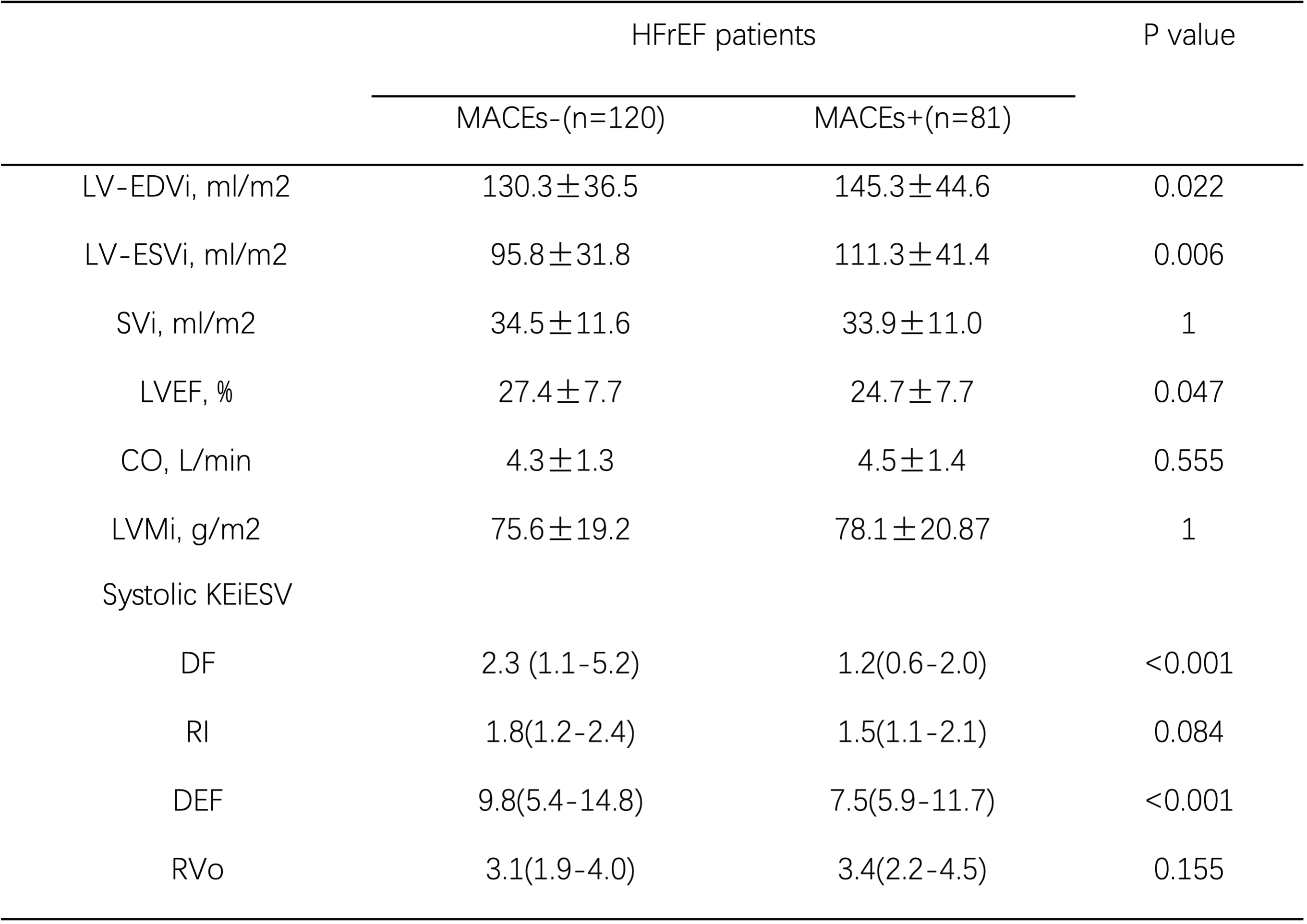
A total of 201 patients with HFrEF were finally recruited in the study, with 81 (62 males) MACEs+ and 120 MACEs- (84 males) patients, the average age were higher when compared with the latter group (58.2±11 vs 54±13 yeas, P = 0.01)(Table 1). MACEs+ groups had the lower DF and DF-KEiESV/EDV, which also featured with the higher RVo and peak E-wave RVo-KEiEDV when compared with MACEs- group (all P<0.05) (Table 2). It has similar trend when considered progressive LV volumes, deteriorated left ventricular ejection fraction (LVEF) (P<0.05). In the multivariable logistic regression model, the factors that acted as independent predictors were peak E-wave RVo-KEiEDV (OR=1.40, 95% CI=1.19-1.65, P=0.0001). In contrast, neither LV volumes nor LVEF showed independently predictive capability. Youden’s Index identified an optimal peak E-wave RVo-KEiEDV cut-of at 6.63 μJ/mL to classify patients at high-risk category (p <0.001 on log rang testing).Discussion
CMR 4D flow is recognized as a promising imaging tool to evaluate intracardiac blood flow component[5]. Reduced DF-KEiESV, DEF-KEiESV, higher RVo and peak E-wave RVo-KEiEDV were identified in MACE+ group when compared with MACE+ group. But no there were no significantly deference in DEF and RI between MACEs+ and MACEs- groups of HFrEF, in HFrEF patients. There is a theory that pathologically enlarged LV leads to an increased LV RVo[6]. However, it would be an interaction of LV dilation and enlarged RVo of LV flow component. The progressively increase of RVo also contributed to progressively enlarged LV volume. The KE of the RVo may also hold a potential advantage in preventing blood stasis and thrombus formation. This hypothesis is supported by the study utilizing CMR 4D flow study that found lower apical intracardiac KE in patients with thrombus compared to the other group [7].Conclusions
CMR 4D flow derived intracardiac hemodynamic parameters are associated with MACEs in HFrEF patients,which could provide clinical value for early diagnosis and treatmentAcknowledgements
noneReferences
1. Maggioni A P, Dahlström U, Filippatos G, Chioncel O, Leiro MC, Drozdz J, et al. EURObservational Research Programme: regional differences and 1-year follow-up results of the Heart Failure Pilot Survey (ESC-HF Pilot). Eur J Heart Fail 2013;15:808-817.
2. Juffermans J F, Minderhoud S, Wittgren J, Kilburg A, Ese A, Fidock B, et al. Multicenter consistency assessment of valvular flow quantification with automated valve tracking in 4D flow CMR. JACC Cardiovasc Imaging 2021; 14:1354-1366.
3. Kanski M, Arvidsson P M, Töger J, Borgquist R, Heiberg E, Carlsson M, et al. Left ventricular fluid kinetic energy time curves in heart failure from cardiovascular magnetic resonance 4D flow data. J Cardiovasc Magn Reson 2015; 17:111.
4. Van Der Geest R J, Garg P. Advanced analysis techniques for intra-cardiac flow evaluation from 4D flow MRI. Curr Radiol Rep 2016; 4:38.
5. Dyverfeldt P, Bissell M, Barker A J, Bolger AF, Carlhäll C-J, Ebbers T, et al. 4D flow cardiovascular magnetic resonance consensus statement. J Cardiovasc Magn Reson 2015; 17:72.
6. Stoll V M, Hess A T, Rodgers C T, Bissell MM, Dyverfeldt P, Ebbers T, et al. Left ventricular flow analysis. Circ Cardiovasc Imaging 2019;12:e8130.
7. Garg P, van der Geest R J, Swoboda P P, Crandon S, Fent GJ, Foley JRJ, et al. Left ventricular thrombus formation in myocardial infarction is associated with altered left ventricular blood flow energetics. Eur Heart J Cardiovasc Imaging 2019; 20:108-117.
Figures