4910
The effect of valve annulus tracking on mitral valve regurgitation: A comparative in vitro study between ultrasound and 4D flow MRI1Medical Device Development Center, Daegu-Gyeongbuk Medical Innovation Foundation, Daegu, Korea, Republic of, 2Ulsan university, Ulsan, Korea, Republic of, 3Department of Radiology, Children's Hospital Colorado, University-Campus, Aurora, CO, United States, 4Institute of Medical Devices, Kangwon National University, Chuncheon, Korea, Republic of
Synopsis
Keywords: Flow, Cardiovascular
Motivation: Mitral valve regurgitation (MVR) is the most common heart valve diseases, but accurate quantification of MVR has been limited due to the dynamic motion of valves.
Goal(s): We hypothesize that volumetric flow information by 4D flow MRI with the compensation of MV motion could address this challenge.
Approach: MVR was measured using a simulated-in vitro model by comparing with actual flow from pump, ultrasound, and 4D flow MRI with/without a mitral registration algorithm.
Results: PISA method overestimated MVR. 4D flow MRI without algorithm seems to have similar the amount of actual MVR, while it decreased with employing algorithm.
Impact: Accurate quantification of regurgitation plays an important role for diagnosing patients with valvular diseases. This study would have a chance to measure accurate MVR quantification and quantify complex intracardiac blood flow using 4D flow MRI.
Introduction
Mitral valve regurgitation (MVR), generating backflow from left ventricle (LV) to left atrium (LA) by MV dysfunction, has been closely associated with various cardiovascular complications such as ventricular fibrillation and heart failure1. Thus, early diagnosis plays an important role to determine severity of diseases and treatment timing. Many studies have investigated non-invasive diagnostic techniques such as ultrasound and magnetic resonance imaging (MRI) to diagnose MVR2,3. In addition, time-resolved three-dimensional phase-contrast MRI (4D flow MRI) technique has emerged as a promising tool to obtain volumetric intracardiac flow information, which enables accurate quantification for complex blood flow4. However, the static placement of measurement planes during 4D flow MRI analysis is not capable of precisely quantifying flow when accompanied by dynamic motions of MV5. Our overarching hypothesis is that tracking dynamic MV motion would potentially compensate flow quantification compared with fixed-plane quantification method. Thus, this study aims to investigate the performance of MVR assessment using an in-house pulsatile pump with a given actual flow, gold-standard ultrasound measurement, and 4D flow MRI with/without a motion correction algorithm through a MVR-simulated in vitro phantom model.Methods
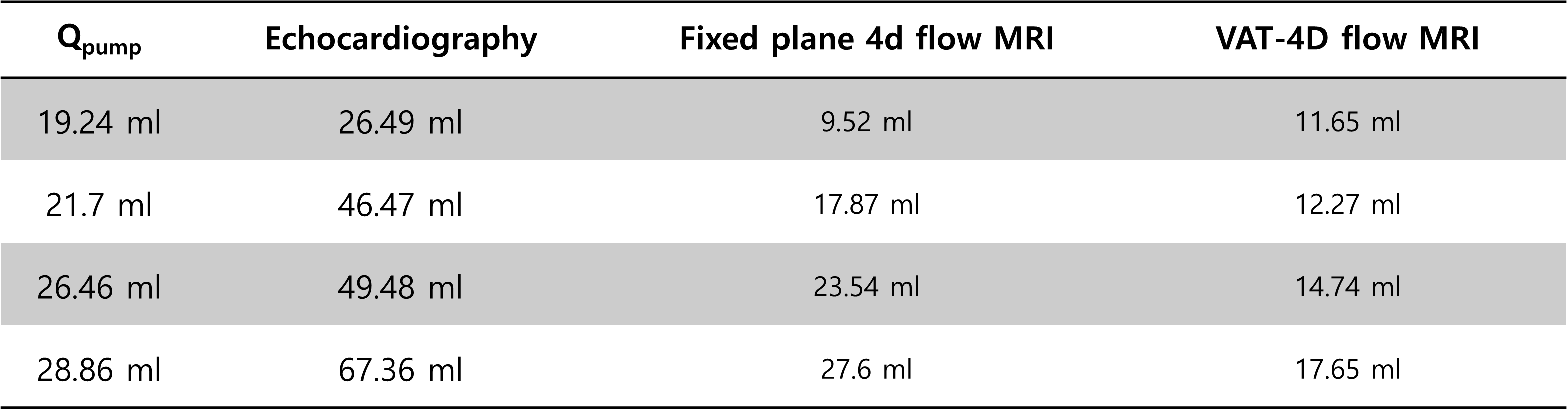
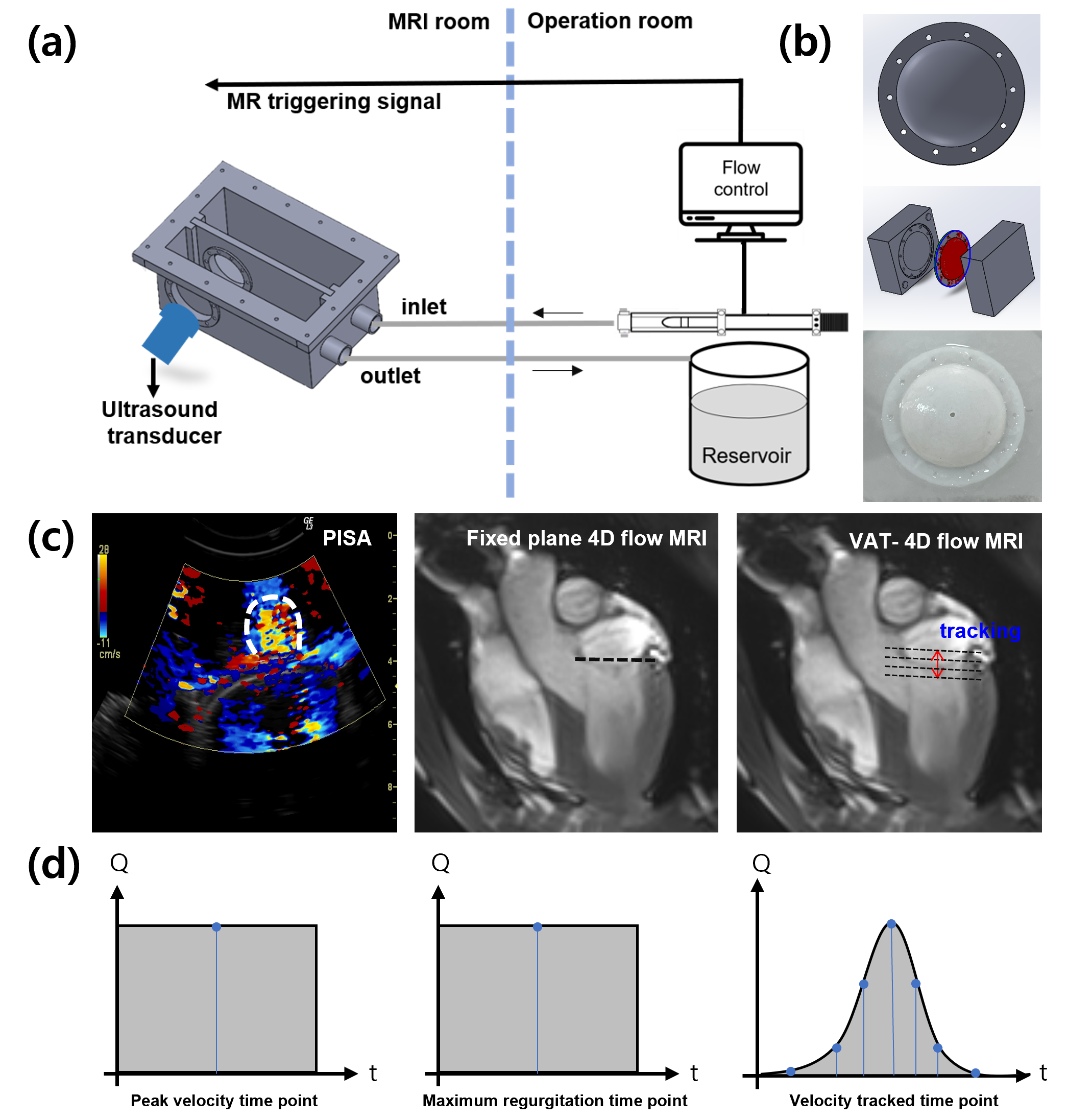
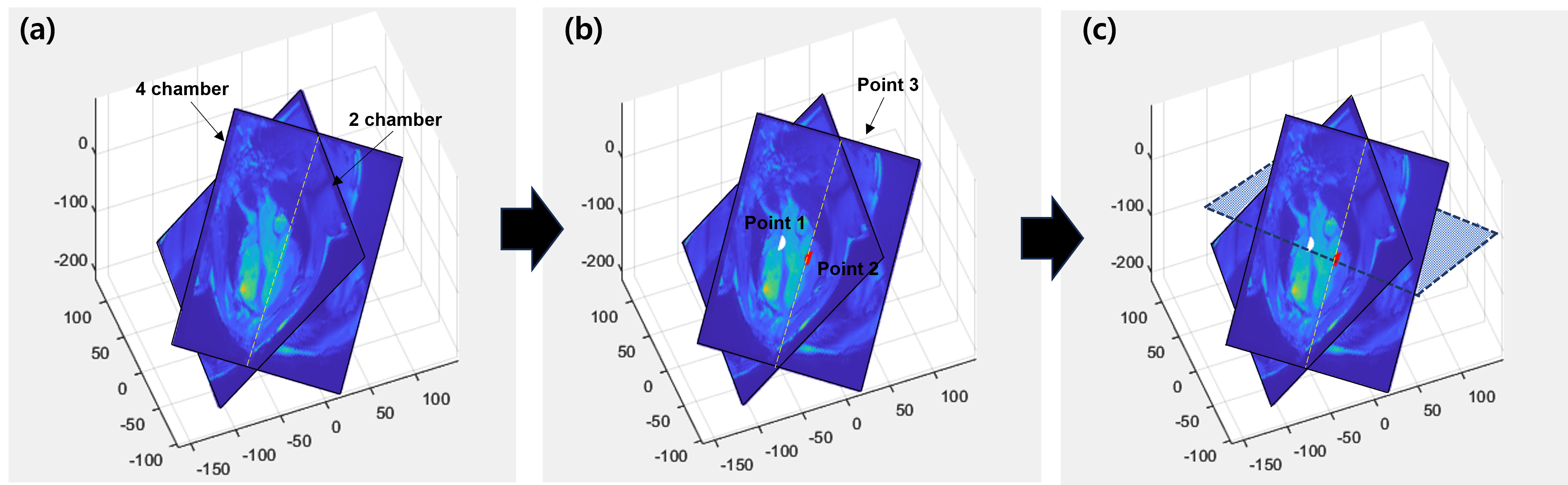
MVR-simulated in vitro phantom model, composing of artificial LV and LA, was fabricated to compare the performance of MVR assessment by both ultrasound and 4D flow MRI (Fig.1a,b). A silicon partition with a tiny hole was placed at the center of the model to replicate MVR. Valve annulus tracking (VAT) algorithm was developed using cardiac MR (CMR) images of a porcine model (Fig. 1c). Spatial orientation and resolution of 4D flow MRI and CMR data were matched in 2-chamber and 4-chamber views. MV plane was extracted from three points, and time-sequential MV planes were obtained at each cardiac cycle. 4D flow MRI images were acquired using a 3T clinical MR scanner (Skyra, Siemens AG, Munich, Germany). Potential actual MVR flow (Qpump) was summarized in Table 1. MVR by ultrasound was quantified using the Proximal Isovelocity Surface Area (PISA) method, while fixed plane and VAT-corrected MVR quantification by 4D flow MRI was also performed using maximum flow rate and time-dependent flow rate, respectively (Fig. 1d).Result
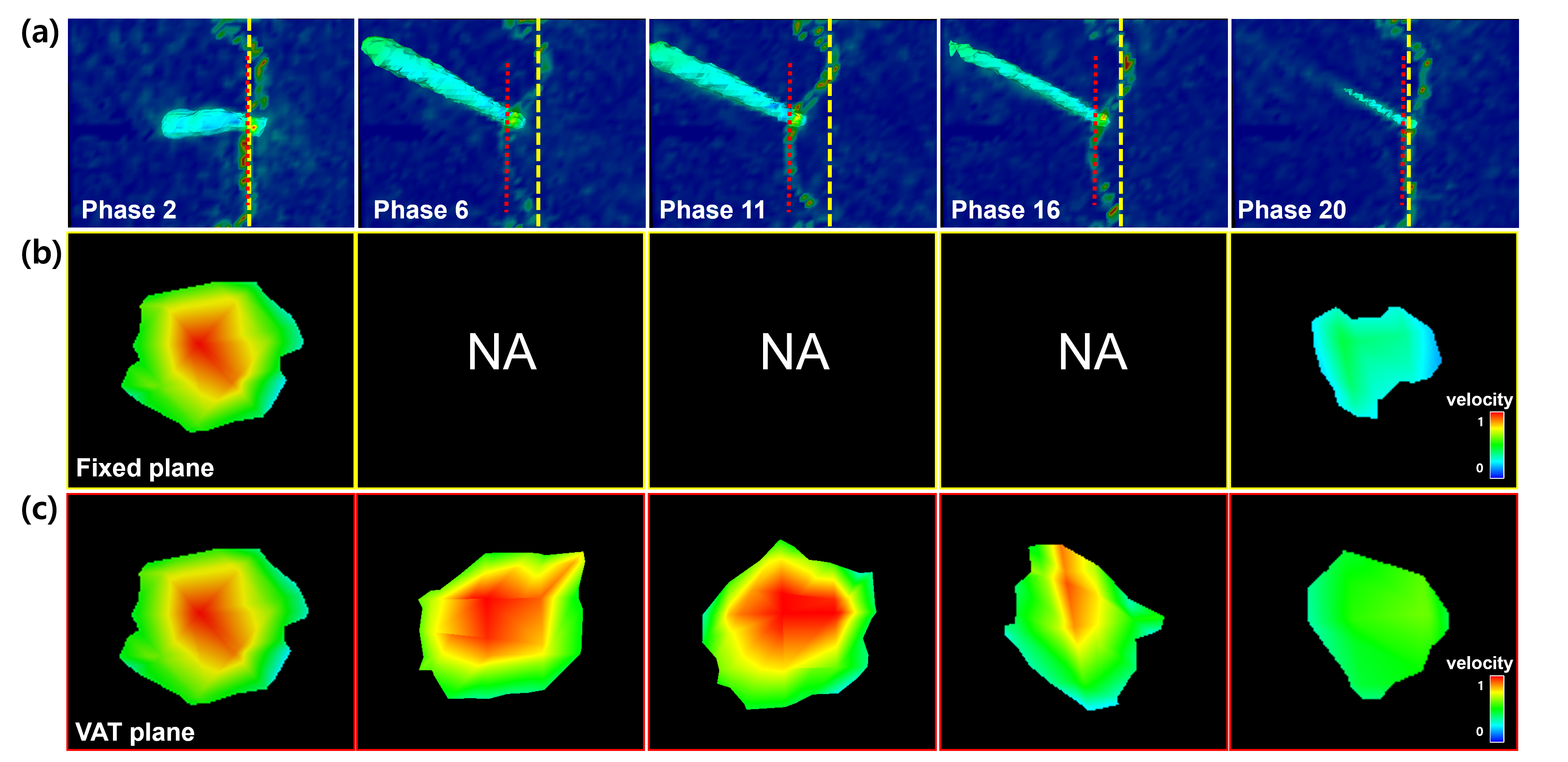
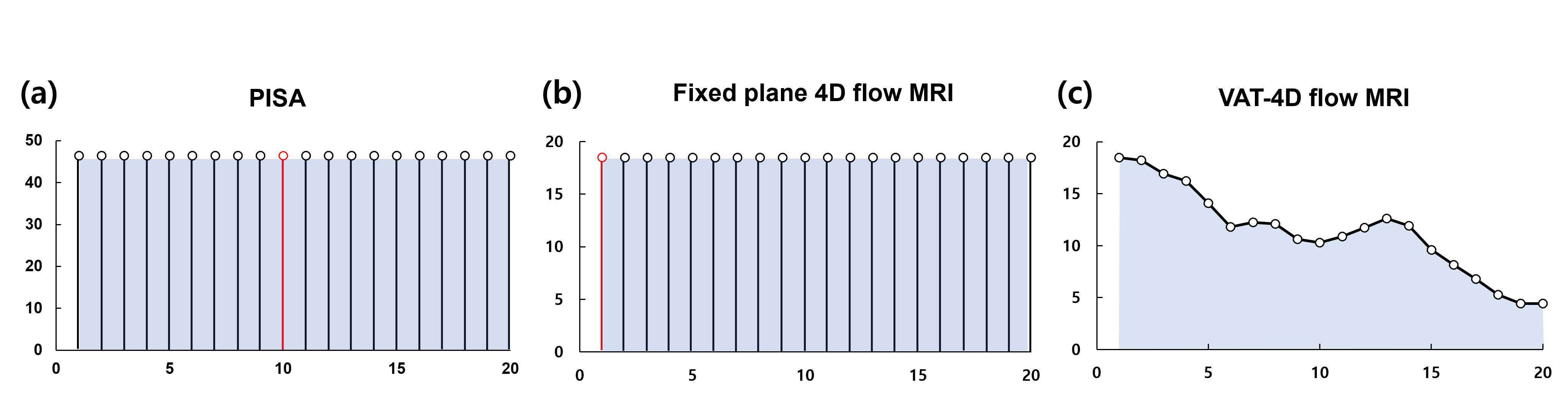
Fixed plane 4D flow MRI had consistent MVR flow over time, while VAT-4D flow MRI is capable of changing MVR over time (Fig. 3). However, we observed that systematic underestimation of MVR quantification by 4D flow MRI with both fixed plane and VAT methods, while the PISA method overestimate MVR quantification (Table 1). This is mainly attributed to the differences in velocity measurement: Fixed plane 4D flow MRI – peak jet velocity, VAT 4D flow MRI – time-dependent flow, ultrasound – maximum velocity (Fig 4).Discussion
We have successfully developed the in vitro analysis platform compatible with both ultrasound and MRI, enabling MVR assessment. However, we observed a discrepancy in the MVR flow measured by the VAT-4D flow MRI, which theoretically should provide precise measurements, compared to Qpump. We speculate that there might be two potential challenges: (1) underestimation of velocity due to the limitations of the MRI system's low spatiotemporal resolution and (2) flow resistance along an extended tube length, resulting in a lower inlet flow within the tube compared to the actual flow generated by the pump. A detailed examination is required for an accurate assessment of MVR and different scenarios of mitral valve dysfunction will be further investigated.Conclusion
The fixed plane and VAT plane 4D flow MRI showed that MVR was underestimated, but most similar to the actual value in the fixed plane and was overestimated in PISA.Acknowledgements
This research was supported by National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIP) (NRF-2021R1C1C1003481)References
1. Agricola, E. et al. Long‐term prognosis of medically treated patients with functional mitral regurgitation and left ventricular dysfunction. European journal of heart failure 11, 581-587 (2009).
2. Igata, S. et al. Optimal quantification of functional mitral regurgitation: comparison of volumetric and proximal isovelocity surface area methods to predict outcome. Journal of the American Heart Association 10, e018553 (2021).
3. Sivalokanathan, S. The role of cardiovascular magnetic resonance imaging in the evaluation of hypertrophic cardiomyopathy. Diagnostics 12, 314 (2022).
4. Blanken, C. et al. Quantification of mitral valve regurgitation from 4D flow MRI using semiautomated flow tracking. Radiology: Cardiothoracic Imaging 2, e200004 (2020).
5. Fidock, B. et al. A systematic review of 4D-flow MRI derived mitral regurgitation quantification methods. Frontiers in cardiovascular medicine 6, 103 (2019).
Figures