4898
Towards an Intraoral Coil Array Design for Dental MRI1Division of Medical Physics, Department of Diagnostic and Interventional Radiology, University Medical Center Freiburg, Faculty of Medicine, University of Freiburg, Freiburg, Germany, 2Department of Neuroradiology, Heidelberg University, Heidelberg, Germany
Synopsis
Keywords: RF Arrays & Systems, RF Arrays & Systems, intraoral, dental, maxillofacial, RF coil
Motivation: In dental diagnostics MRI provides an improved soft tissue contrast for endodontic, craniomaxillofacial and implant applications with better visibility of anatomical structures.
Goal(s): An intraoral coil array is introduced for dental MRI to investigate feasibility, achievable signal gain and parallel acquisition performance.
Approach: Coil element size, material, and shape properties are investigated with respect to image SNR. The array is adjusted to the dental anatomy on a 3D phantom to estimate the sensitivity and the g factor of parallel imaging.
Results: Intraoral coil array improves SNR, spatial resolution and provides a homogenous B1 receive profile. It allows parallel imaging to minimize measurement time.
Impact: Intraoral coil arrays can enhance MRI of small dental structures, required for endodontics, while increasing the spatial coverage in oral cavity. Compared to single-loop coils, a more homogeneous receive sensitivity can be achieved and parallel imaging becomes feasible.
Introduction
MRI offers a superior soft tissue contrast, which can improve diagnosis in endodontics1-3; and planning for craniomaxillofacial surgeries4 with better delineation of lesions and higher contrast in anatomical structures. Most dental pathologies affect the pulp and surrounding dental root canals - small structures with sub-millimeter dimensions. Since resolution and signal-to-noise ratio are inversely proportional, conventional extraoral RF coils have a lower sensitivity than intraoral coils (IOC)5-8. To date, IOCs have been limited to a single coil. This study introduces the first IOC array for dental MRI and investigates the effects of coil element size, material, and shape on the SNR. IOC array is tailored to dental anatomy, and enhances the sensitivity, and enables parallel imaging for faster image acquisition.Most dental pathologies affect the pulp and surrounding canals - small structures with sub-millimeter dimensions.
Methods
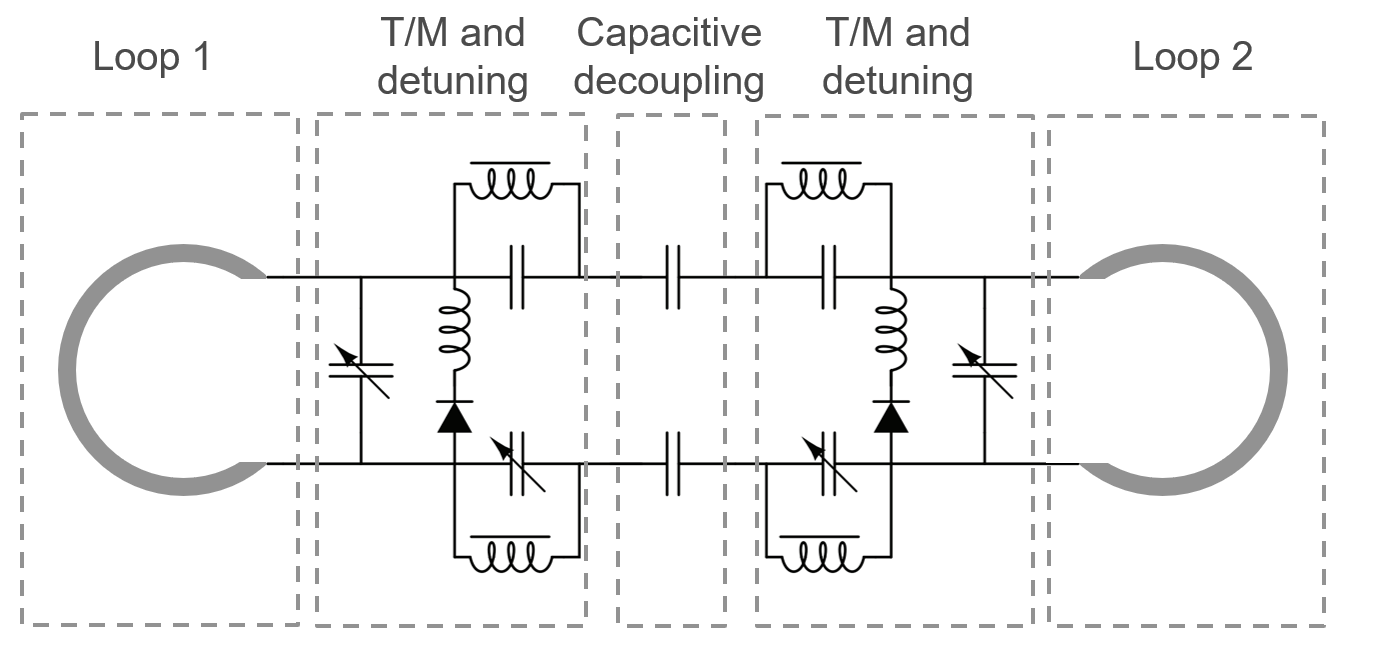
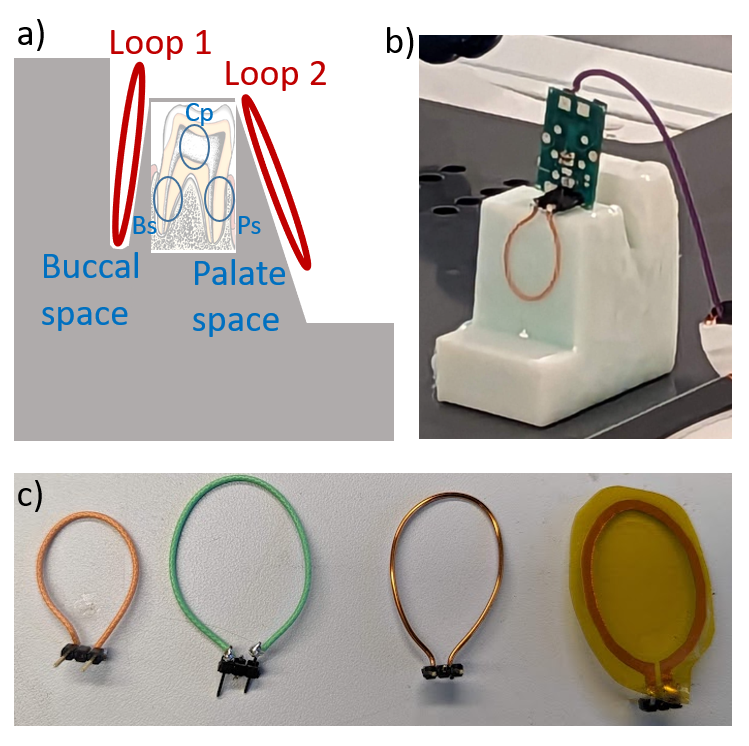
Coil setup: A schematic design shows a receive-only intraoral coil array consisting of 2 coil elements (Fig.1). Both loop coils elements, L1 and L2, are interfaced to the MRI receiver via a tune/match and active detuning circuit. Capacitive decoupling reduces mutual coupling. Principal coil positions are displayed in Fig.2a-b using a 3D printed phantom which is based on oral anatomy. The gaps of the phantom emulate the buccal space between tooth and cheek (L1) and the lingual space between tongue and teeth (L2). To determine the optimal coil size and material, 3 conductor types were compared: solid copper wire, KaptonTM foil with copper tracks (width: 2mm, thickness: 35µm), and the flexible shield of a coaxial wire (Ø: 0.8 and 1mm). Further, 4 different loop coil circumferences were investigated: 6.4, 7.7, 9.0, and 10.3cm. First, 1-channel coils were constructed for all types and sizes, and SNR was calculated in selected region of interest (ROI). Afterwards, 2-channel prototypes were constructed for selected loops to quantify all relevant ROIs.
Measurement setup: All MRI measurements were conducted at a clinical 3T system (PrismaFit, Siemens, Germany). The 3D phantom was filled with water and CuSO4 solution to achieve loading conditions similar to the human body. To compare the SNRs, a 2D FLASH sequence was applied with TR=5.5ms, TE=2.1ms, FA=20°, BW=500Hz/px, resolution: 0.7x0.7mm³, FoV=140mm², averages: 16, TA=56s. In addition, parallel imaging was performed using a generalized autocalibrating partially parallel acquisitions (GRAPPA)9 and sensitivity encoding (SENSE)10 with R=2 and TA=28s. From the SNR maps g-factor maps were calculated for SENSE and GRAPPA.
Results
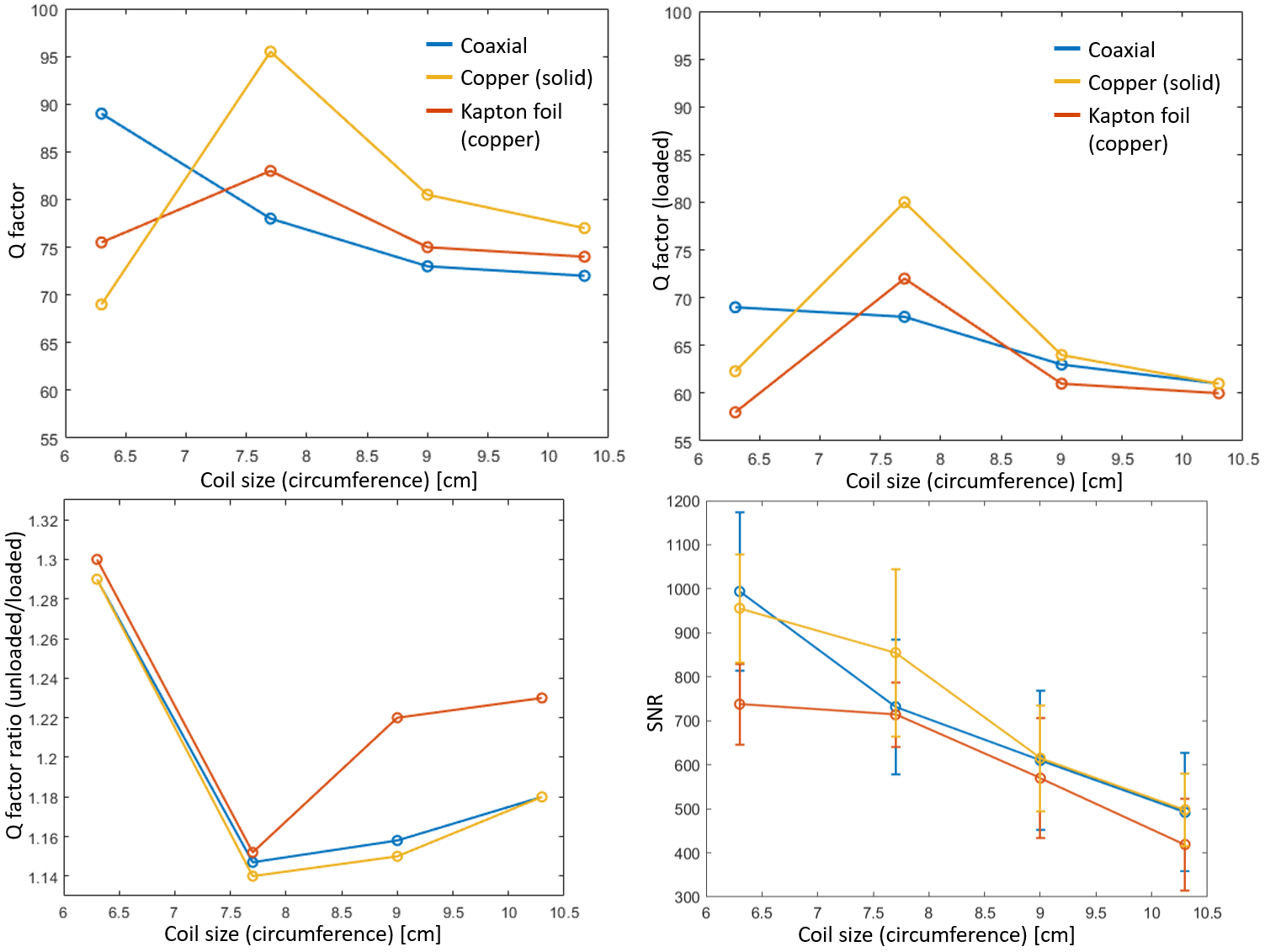
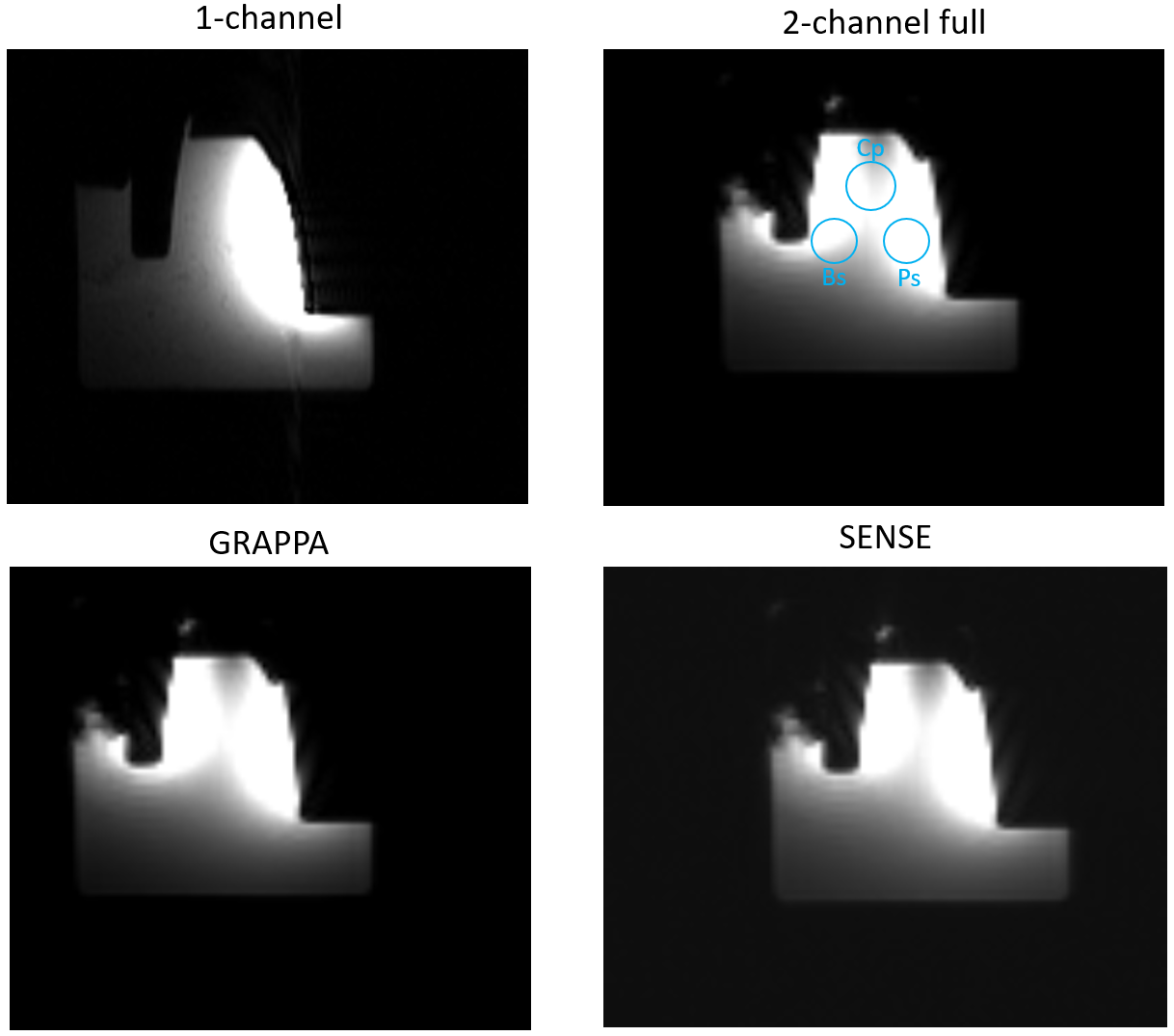
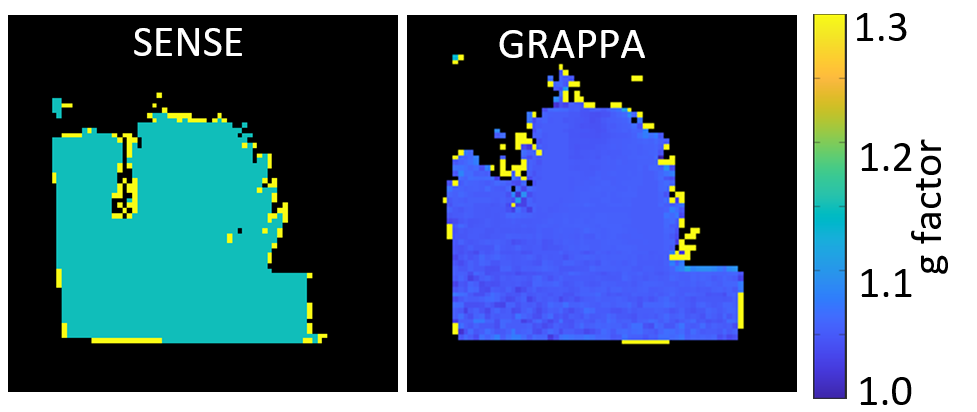
Fig.3 summarizes the Q factor and SNR comparison of the different 1-channel prototypes. Solid copper and Kapton display the same trend for all results with 6% to 15% higher Q factor values and up to 26% higher SNR for solid copper coils. Q factor of the coaxial loop coils is up to 10% lower than the other coils. Under loading, coaxial loop performs better with decreasing size. The smallest coaxial loop shows the best performance in unloaded (88), loaded (68) Q factor and SNR (1001), similar to the solid cooper for SNR. Kapton has the lowest SNR with a maximum SNR of 730 for the smallest loop.Fig.4 shows a comparison of SNR between full and parallel acquisition (GRAPPA and SENSE) for three different ROIs (Fig.2a). ROIBs has the highest SNR for the full acquisition of 3858 with comparable value at ROIPs. The ROICp retains around 70% of the SNR at 2276. Grappa has an SNR of 2692 at ROIBs and 1591 at ROICp which is around 69% of the expected SNR $$$ \approx 1/\sqrt{2}$$$. With SENSE, a lower SNR of 2422 at ROIBs and 1336 at ROICp is seen, i.e., 60% of the full acquisition SNR. The quantitative g-factor map (Fig.5) for SENSE shows an average g value of 1.05 and GRAPPA resulted in a value of 1.15.
Discussion
In this study, we introduced the first intraoral coil array for dental MRI. Measurements showed that at coil diameters as small as 19mm sample noise dominated – previous measurements demonstrated that a 15mm coil is sufficient to depict root canals6. Flexible coaxial wires outperformed other conductors with an overall SNR gain between 2.5 (parallel acquisition) and 3.8 – this SNR increase adjacent to the coil might improve delineation of small dental structures. The SNR of the coil array will be investigated in vivo and compared to other coil systems to demonstrate the benefits. Further, mutual coil coupling will be studied as this can change substantially in vivo. Extending this coil concept to a higher number of coil elements in the array can considerably increase the SNR which might allow rapid parallel acquisition techniques to shorten the acquisition times.Acknowledgements
No acknowledgement found.References
1. Ariji Y, Ariji E, Nakashima M, Iohara K. Magnetic resonance imaging in endodontics: a literature review. Oral Radiol. 2018;34:10–16 doi: 10.1007/s11282-017-0301-0.
2. Leontiev W, Bieri O, Madörin P, et al. Suitability of Magnetic Resonance Imaging for Guided Endodontics: Proof of Principle. J. Endod. 2021;47:954–960 doi: 10.1016/j.joen.2021.03.011.
3. Juerchott A, Pfefferle T, Flechtenmacher C, et al. Differentiation of periapical granulomas and cysts by using dental MRI: a pilot study. Int. J. Oral Sci. 2018;10 doi: 10.1038/s41368-018-0017-y.
4. Juerchott A, Freudlsperger C, Zingler S, et al. In vivo reliability of 3D cephalometric landmark determination on magnetic resonance imaging: a feasibility study. Clin. Oral Investig. 2020;24:1339–1349 doi: 10.1007/s00784-019-03015-7.
5. Ludwig U, Eisenbeiss A-K, Scheifele C, et al. Dental MRI using wireless intraoral coils. Sci. Rep. 2016;6:23301 doi: 10.1038/srep23301.
6. Tesfai AS, Vollmer A, Özen AC, et al. Inductively Coupled Intraoral Flexible Coil for Increased Visibility of Dental Root Canals in Magnetic Resonance Imaging. Invest. Radiol. 2022;57:163–170 doi: 10.1097/RLI.0000000000000826.
7. Idiyatullin D, Corum CA, Nixdorf DR, Garwood M. Intraoral approach for imaging teeth using the transverse B1 field components of an occlusally oriented loop coil. Magn. Reson. Med. 2014;72:160–165 doi: 10.1002/mrm.24893.
8. Özen AC, Idiyatullin D, Adriany G, et al. Design of an Intraoral Dipole Antenna for Dental Applications. IEEE Trans. Biomed. Eng. 2021;68:2563–2573 doi: 10.1109/TBME.2021.3055777.
9. Griswold, Mark A., et al. "Generalized autocalibrating partially parallel acquisitions (GRAPPA)." Magnetic Resonance in Medicine: An Official Journal of the International Society for Magnetic Resonance in Medicine 47.6 (2002): 1202-1210.
10. Pruessmann, Klaas P., et al. "SENSE: sensitivity encoding for fast MRI." Magnetic Resonance in Medicine: An Official Journal of the International Society for Magnetic Resonance in Medicine 42.5 (1999): 952-962.
Figures