4884
The hierarchy of hazard controls in MR safety practice1Medical Physics Unit and Gerald Bronfman Department of Oncology, McGill University, Montreal, QC, Canada, 2Medical Physics, McGill University Health Centre, Montreal, QC, Canada, 3Medical Imaging, McGill University Health Centre, Montreal, QC, Canada
Synopsis
Keywords: Safety, Safety
Motivation: MR safety guidance formulated by experts from the MR community build upon a combination of experience and technical expertise. MR safety guidance may benefit from assessment based on general workplace safety practices.
Goal(s): To critically assess MR safety guidance and practices using the hierarchy of hazard controls.
Approach: MR safety practices were scored using a 5-point scale derived from the hierarchy of hazard controls, in several areas of risk for MR personnel, patients, and non-MR personnel.
Results: Hazard controls for non-MR personnel had consistently high effectiveness scores, while those for for MR personnel and patients had moderate effectiveness scores, with a greater range.
Impact: The analysis presented in this work could serve as a tool to analyse choices made in the deployment of safety measures, to motivate decision- or policy-making, or as a tool for assessment of MR safety programs.
Introduction
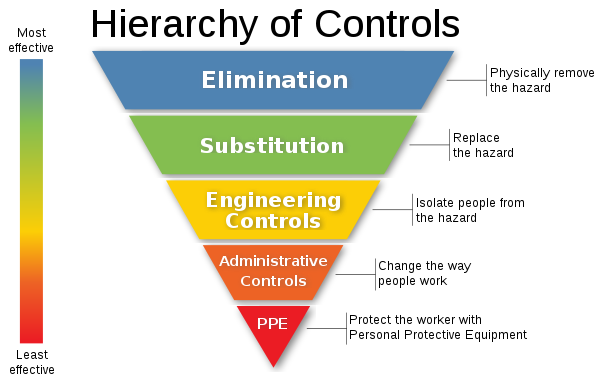
The hierarchy of hazard controls is a framework that can be used to design and assess choices made to provide safety precautions for workers. The hierarchy of hazard controls is often used by government agencies and other institutions (e.g. Centers for Disease Control and Prevention, UK Health and Safety Executive, Health Canada) to guide safety practice in a variety of contexts that is largely aimed at workers exposed to hazardous conditions. The hierarchy of hazard controls is often presented using a colour-coded diagram that shows control methods from least effective to most effective (Figure 1). Control categories range from Elimination (most effective) of Hazard to Personal Protective Equipment (least effective).MR safety practice relies largely on guidance from experts through publications from professional and/or institutional publications, such as the American College of Radiology [1], the United Kingdom’s Medicines and Healthcare products Regulatory Agency [2] and the Royal Australian and New Zealand College of Radiologists [3]. MR safety guidance has largely evolved based on the growth of experience and expertise over time to combine the experience of users in the field, advances in the understanding of clinical practices, risks of patient and staff exposure, scientific understanding, and technological advances.
Assessment of MR safety practice may benefit from tools from general workplace safety. In this work, a critical analysis of MR safety guidance documents was performed using the framework of the hierarchy of hazard controls.
Methods
Risk categories of MR safety practice were selected based on their mention in various safety guidelines. Assessments were performed of safety measures in each category as they apply to 3 different groups of people according to their interaction with MR systems: (i) MR personnel, trained operators of MR systems, (ii) patients and research participants, who enter the MR environment to undergo MR examination, and (iii) the general public, which includes for example non-MR personnel working in MR facilities and individuals accompanying patients or participants during their journey to the MR facility. A scale of 1 to 5 points was assigned to the hierarchy of hazard controls to quantify the level of efficacy as follows: Elimination (5), Substitution (4), Engineering Controls (3), Administrative Controls (2), Personal Protective Equipment (1). MR safety measures recommended by MR safety guidance were scored according to their level of efficacy in the hierarchy of hazard controls. Median and range of scores was used to produce a total score for each risk category.Results
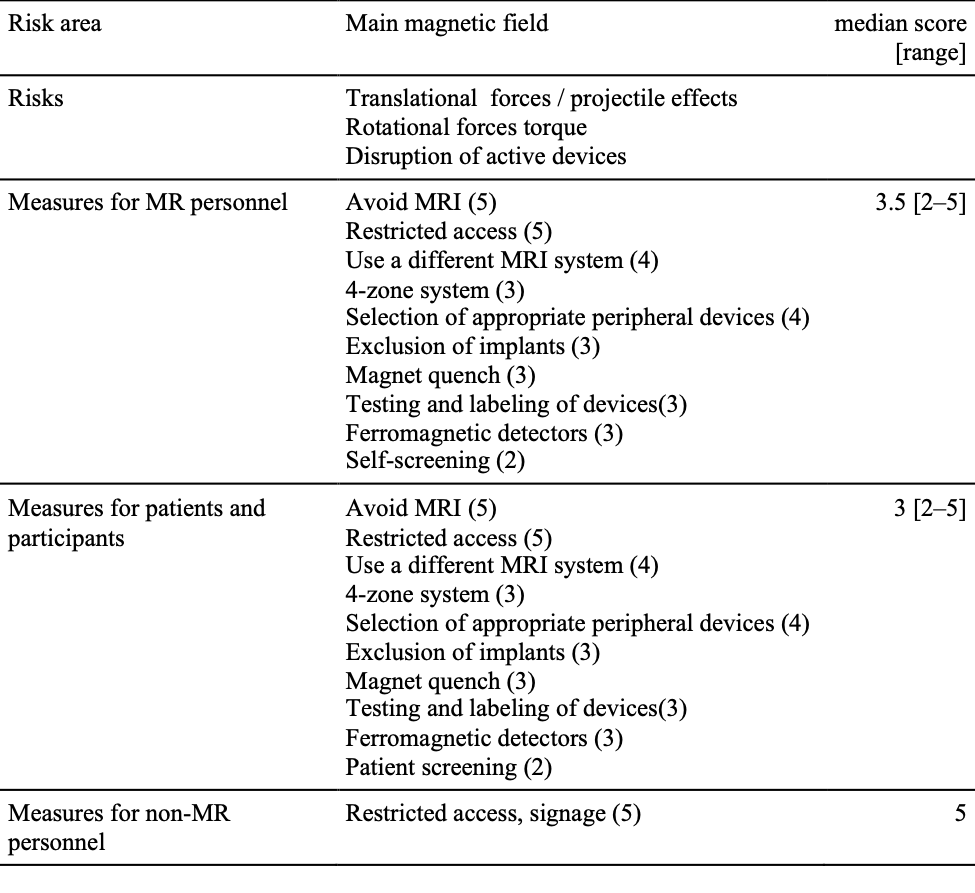
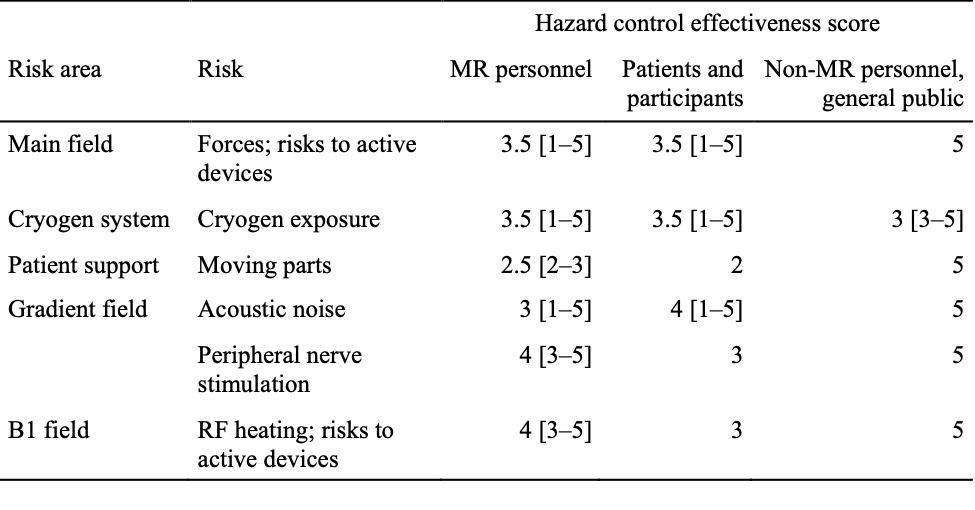
An example assessment is described for one area of risk in Table 1. Summary results of the scoring exercise are reported in Table 2. In this analysis, many potential measures available for reduction of hazards were considered. The median score thus reflects the achievable score when all protective measures are included in the analysis. The range of scores in each category reflects the range of effectiveness of controls in each area. The highest median scores were seen for measures for non-MR personnel, while scores are relatively similar for MR personnel and patients. The largest ranges of control scores are observed for exposure to gradient field acoustic noise and main magnetic field.Discussion
This work presents a preliminary critical assessment of hazard controls in MR safety. Consideration of these scores could be used in judging emphasis to be applied in MR safety programs, underlining the importance of select operational decisions, or in decision-making in the deployment of MR systems.Certain hazard control measures in MR practice must be implemented at the system design level (e.g. calculation of exposure to RF fields through SAR, acoustic damping in MR systems) or at the time of system feature selection (main field strength, pulse sequence selection) and are therefore out of reach of the MR system operator making decisions that affect patient exposure to various risks.
As a limitation of this work, the significant benefit that patients derive from entering the MR environment to undergo MR examination was not scored in this study. An appropriate system for risk-benefit analysis, weighed against this hierarchy of hazard controls, could be a significant improvement on the proposed analysis. The hierarchy could also be used to score the effectiveness of policies to protect research participants in carrying out risk analysis for specific studies and/or research facilities.
Finally, this analysis could be applied to areas of concern (real or potential) arising from specialized use of MR systems in non-conventional settings (MR-guided interventions, MR-guided radiation therapy). The scoring system could be of interest in assessment of specific MR safety programs.
Acknowledgements
No acknowledgement found.References
[1] American College of Radiology, ACR Manual on MR Safety, 2020, https://www.acr.org/-/media/ACR/Files/Radiology-Safety/MR-Safety/Manual-on-MR-Safety.pdf (retrieved 2023-11-08)
[2] UK Medicines and Healthcare products Regulatory Agency, Safety Guidelines for Magnetic Resonance Imaging Equipment in Clinical Use, 2021, https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/958486/MRI_guidance_2021-4-03c.pdf (retrieved 2023-11-08)
[3] Royal Australian and New Zealand College of Radiologists, RANZCR MRI Safety Guidelines, 2021, https://www.ranzcr.com/college/document-library/mri-safety-guidelines (retrieved 2023-11-08)
Figures