4880
Measuring pulse-wave velocity in the healthy human brain using dynamic inflow magnitude contrast (DIMAC) MRI1Cardiff University Brain Research Imaging Centre (CUBRIC), School of Physics & Astronomy, Cardiff University, Cardiff, United Kingdom
Synopsis
Keywords: Velocity/Flow, Brain, Cerebrovascular health & arterial stiffness
Motivation: Arterial stiffness, a key marker of cardiovascular health, can be monitored by measuring pulse-wave velocity. However, current methods do not extend into the brain due to an inability to resolve the pulse waveform on a beat-to-beat basis for intracranial arteries.
Goal(s): Our goal is to demonstrate the concept of measuring intracranial pulse-wave velocity using dynamic inflow magnitude contrast (DIMAC) MRI.
Approach: We measured intracranial pulse-wave velocity by measuring the pulse-wave delay between internal carotid and middle cerebral arteries.
Results: The arterial pulse-wave delay between the internal carotid artery and the middle cerebral artery was 29±14ms, corresponding to a pulse-wave velocity of 6.8±2.2m/s.
Impact: These results are the first stage in establishing pulse-wave velocity as a new non-invasive MRI biomarker for cerebrovascular health, providing a novel tool to investigate the role of arterial stiffness in healthy ageing and brain pathology.
Introduction
Pulse-wave velocity is a measure of arterial stiffness, providing a key marker of cardiovascular health1-4. It is commonly measured as the pulse-wave delay between carotid and femoral arteries divided by the difference in path length from the heart5. Compliant cerebral arteries act to attenuate the pulse-wave, protecting brain tissue from damage. Therefore, a measurement of pulse-wave velocity through the cerebral vasculature provides specific information about cerebral arterial stiffness and cerebrovascular health. MRI is uniquely able to non-invasively measure pulsatile flow in arteries deep within the skull. Dynamic inflow magnitude contrast (DIMAC) MRI6 can measure the pulsatile flow waveform for individual heartbeats. Whilst the arterial pulse wave can also be resolved by phase-contrast MRI7, those measurements take several minutes, averaging across hundreds of heartbeats. Natural heart rate variability will smooth out these averaged pulse waveforms, limiting their ability to resolve the fine scale pulse delays of tens of milliseconds between intracranial arteries. In this work, we demonstrate the feasibility of measuring pulse-wave velocity between internal carotid and middle cerebral arteries (MCA) using the DIMAC signal.Methods
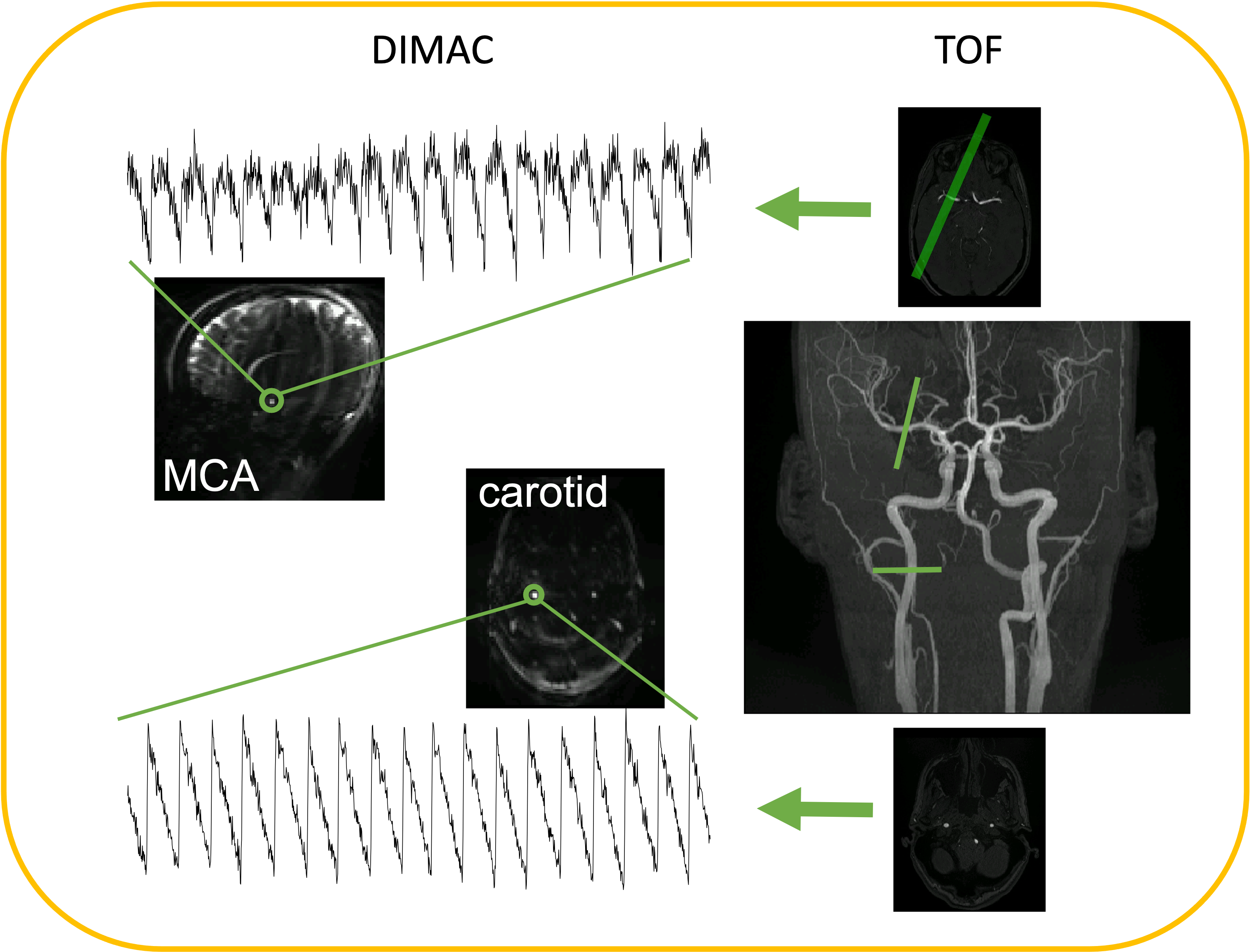
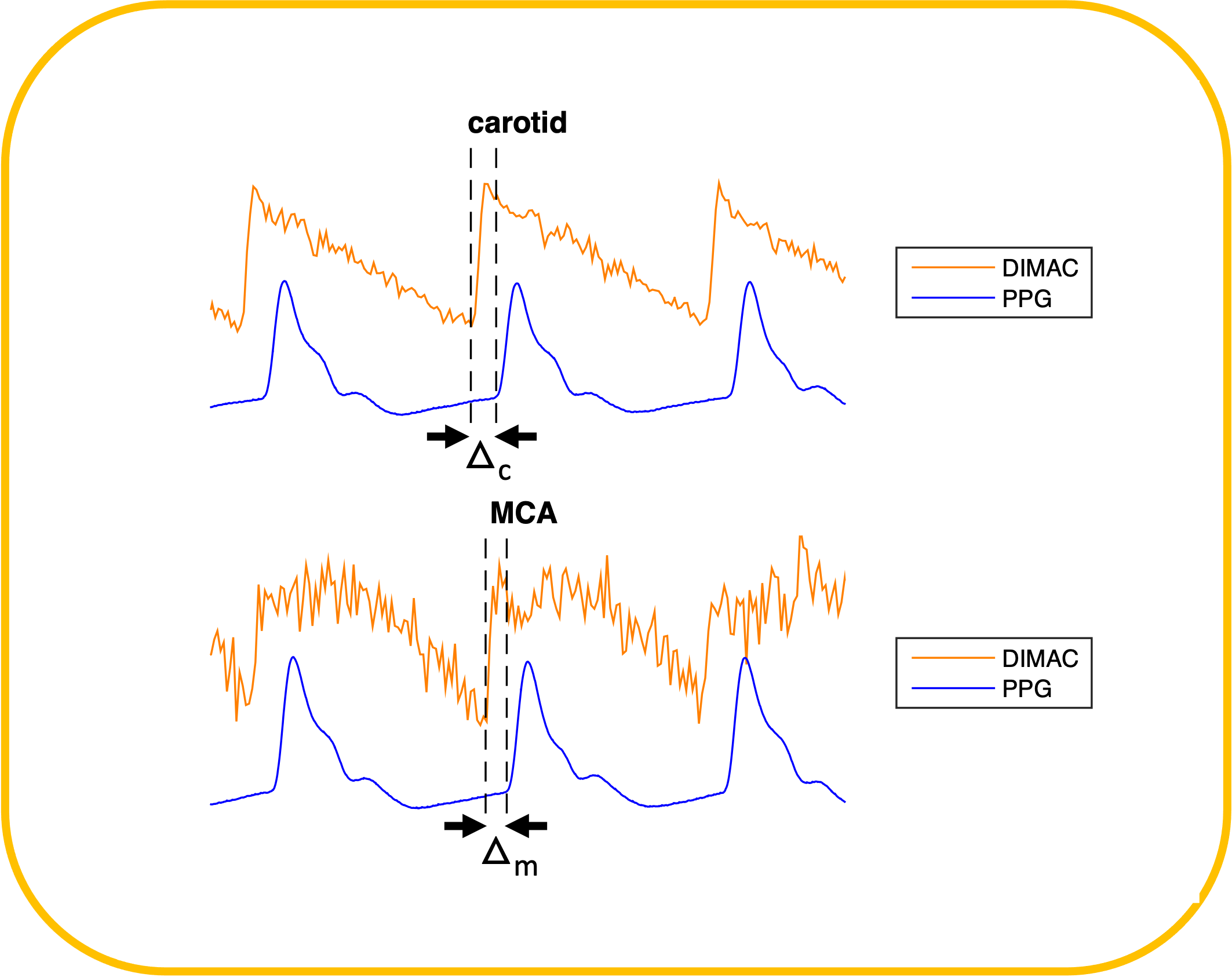
We present data from seven healthy female participants (aged 18-32 years). Data were acquired on a Siemens Prisma 3 Tesla system and peripheral finger pulse measurements were made using a Biopac photoplethysmograph (PPG; 500 Hz sampling frequency). Time-of-flight angiography (TR = 21ms, 0.6mm isotropic) was used for slice positioning and calculating path length between the carotid and MCA. Two DIMAC slices were acquired, positioned perpendicular to the right carotid and right MCA, respectively (Figure 1). Each DIMAC slice was acquired with TR=15ms, 2x2x10mm, GRAPPA=5, 4096 measurements in 1 minute. Pulse timings were determined by fitting a Fourier series basis set to each heartbeat period of each pulse waveform. As carotid and MCA waveforms were not acquired simultaneously, they were both aligned to the finger pulse as a reference point (Figure 2).Results
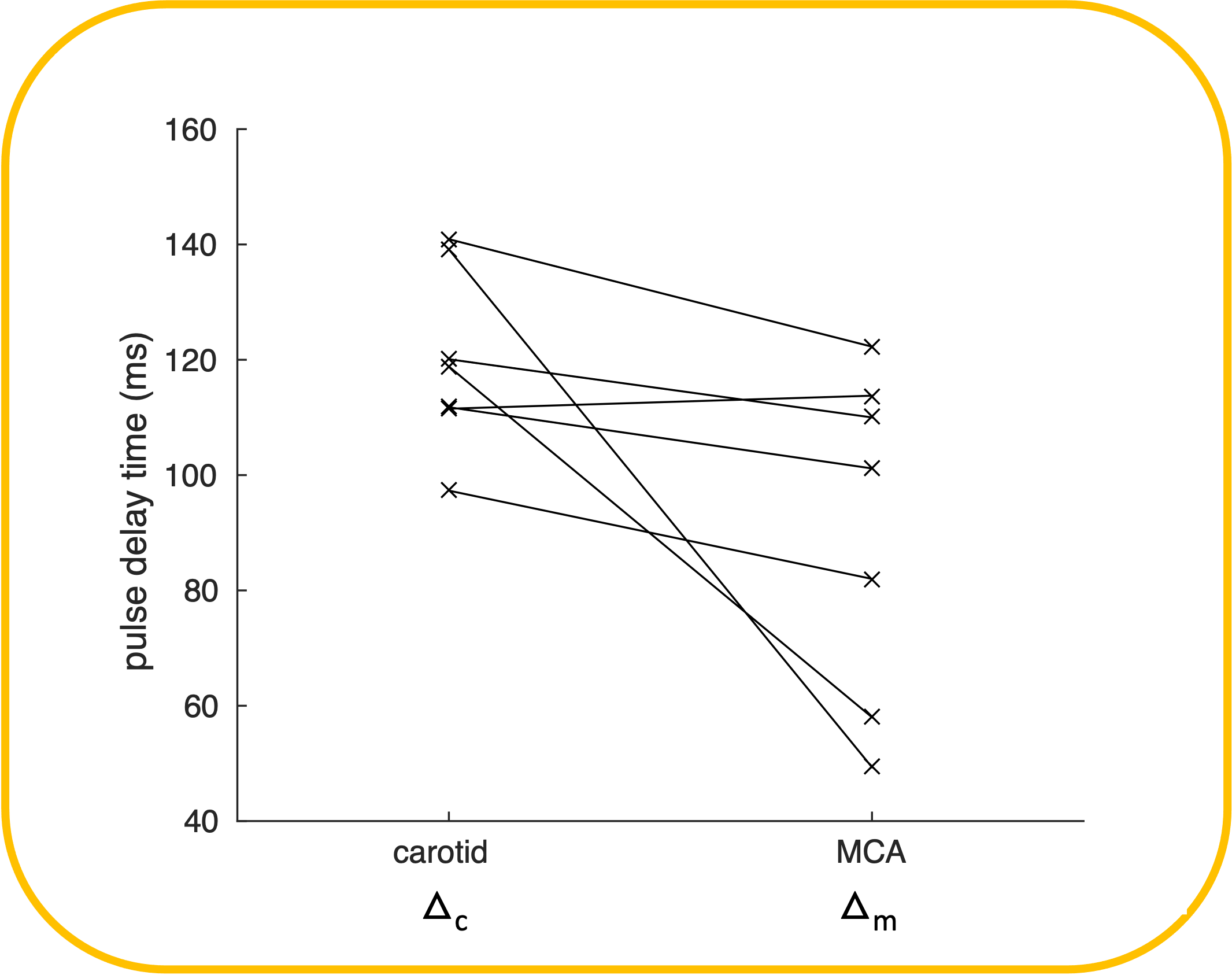
Delays from the DIMAC pulse to the finger pulse are shown in Figure 3, averaged across all heartbeat periods for each subject. The carotid artery led the finger pulse by 120±6ms and the MCA led the finger pulse by 91±12ms. Therefore, the carotid pulse led the MCA pulse by 29±14ms (pWilcoxon=0.03, signed rank=27). The carotid pulse led the MCA pulse in 6 out of the seven subjects. The path length from the carotid to the MCA was measured at 115±7mm. Dividing the path length by the delay for the 6/7 datasets where carotid led MCA pulse gives a pulse-wave velocity of 6.8±2.2m/s.Discussion
In this work we introduce the concept of measuring pulse-wave velocity in the healthy brain. Pulse-wave velocity is a key indicator of vascular compliance, how the pulse-wave is attenuated before reaching (and damaging) brain tissue. The DIMAC flow-sensitive signal allows the pulse to be resolved for individual heartbeats, so is less sensitive to heart rate variability than other MRI methods for studying flow velocity, such as phase-contrast MRI7. The pulse-wave velocity measured here (6.8±2.2m/s) is consistent with carotid to femoral artery measurements in a young, healthy cohort8. This is a small dataset, with a homogeneous demographic (young, female participants). The carotid pulse led the MCA pulse in 6/7 subjects, whilst the amplitude of the delay was driven by 2 subjects. These two subjects, along with the subject with the MCA leading the carotid pulse, had noisier data than the others, with noisier fit residuals. Therefore, we will build on this initial concept demonstration by expanding the sample size, to further understand the variability of the measurement.Conclusion
In conclusion, we present a proof-of-concept study of MRI derived pulse-wave velocity measurements in the human brain. These measurements could provide valuable information on arterial stiffness, that would extend our understanding of vascular pathophysiology in neurodegeneration and related diseases2.Acknowledgements
This work was supported by The Wellcome Trust [WT200804;WT224267].References
1. Alastruey et al. Arterial pulse wave modeling and analysis for vascular-age studies: a review from VascAgeNet. Am J Physiol Heart Circ Physiol 2023; 325: H1–H29; doi: 10.1152/ajpheart.00705.2022
2. Scuteri and Wang. Pulse Wave Velocity as a Marker of Cognitive Impairment in the Elderly. J Alzheimers Dis. 42 Suppl 2014; 4:S401-10; doi: 10.3233/JAD-141416
3. Li et al. Effects of regular aerobic exercise on vascular function in overweight or obese older adults: A systematic review and meta-analysis. J Exerc Sci Fit. 2023; 21(4):313-325; doi: 10.1016/j.jesf.2023.06.002
4. Pomeroy et al. The relationship between sleep duration and arterial stiffness: A meta-analysis. Sleep Med Rev. 2023; 70:101794; doi: 10.1016/j.smrv.2023.101794
5. Milan et al. Current assessment of pulse wave velocity: comprehensive review of validation studies. J Hypertens. 2019; 37(8):1547-1557; doi: 10.1097/HJH.0000000000002081
6. Whittaker et al.
Measuring Arterial Pulsatility With
Dynamic Inflow Magnitude Contrast.
Front Neurosci. 2022; 17;15:795749; doi: 10.3389/fnins.2021.795749
7. Bjornfot et al. Assessing cerebral arterial pulse wave velocity using 4D flow MRI. JCBFM. 2021; 41(10) 2769–2777; doi: 10.1177/0271678X211008744
8. Parikh et al. Measurement of pulse wave velocity in normal ageing: comparison of Vicorder and magnetic resonance phase contrast imaging. BMC Cardiovascular Disorders. 2016; 16:50; doi: 10.1186/s12872-016-0224-4
Figures