4879
Ultrafast breast MRI in differentiating high-grade from benign and low-grade malignant breast lesions1The Fourth Affiliated Hospital of Hebei Medical University, Shijiazhuang, China, 2MR Research Collaboration, Siemens Healthineers Ltd, Beijing, China, 3MR Application Predevelopment, Siemens Healthineers AG, Erlangen, Germany
Synopsis
Keywords: Perfusion, Contrast Mechanisms, breast tumor; Ultrafast Breast MRI
Motivation: Ultrafast (UF)-DCE MRI is a novel approach to obtain kinetic information very early after enhancement, which promises improved capabilities in differentiating malignant from benign lesions of breast cancers.
Goal(s): The early hemodynamic characteristics of lesions using breast UF-DCE MRI were systematically investigated to evaluate the value of the relevant kinetic parameters in the diagnosis of different grades of breast cancer.
Approach: The kinetic parameters of UF-DCE MRI were calculated to differentiate the different grades of breast cancer.
Results: The kinetic parameters of UF-DCE MRI can be used to distinguish high-grade from benign and low-grade breast cancer.
Impact: Breast ultrafast DCE MRI was used to explore the early hemodynamic characteristics of the lesions and evaluate the value of the relevant dynamic parameters in the diagnosis of different grades of breast cancer.
Introduction
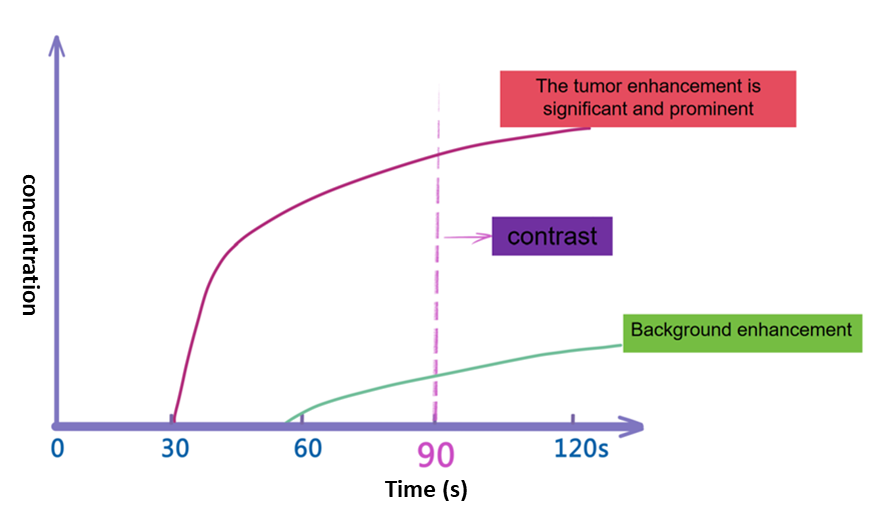
According to the physiological characteristics of the breast circulation, the contrast agent reaches the blood supply artery of the breast within 25~30 s. At this point, the lesions of the malignant tumors with increased vascular permeability are "stained" by the contrast agent, and the tumor bed is fully strengthened. However, the background parenchyma (BP) is not yet fully enhanced, affecting the available time for determining the morphological characteristics of the tumor1 (Figure 1). Therefore, the ultrafast dynamic contrast-enhanced (UF-DCE) MRI technique has been employed to capture the relevant dynamic information of breast lesions within 60 s2. The golden-angle radial sparse parallel MRI (GRASP) technology can achieve continuous dynamic multi-phase enhancement scanning with an ultra-high temporal resolution of 3-10 s and improved spatial resolution. This enables the capture of 10-20 dynamic enhancement phases in the first 60 s after the contrast agent injection. Along these lines, the purpose of this work was to systematically explore the application of breast UF-DCE MRI for identifying benign, low-grade, and high-grade malignant breast tumors.Methods
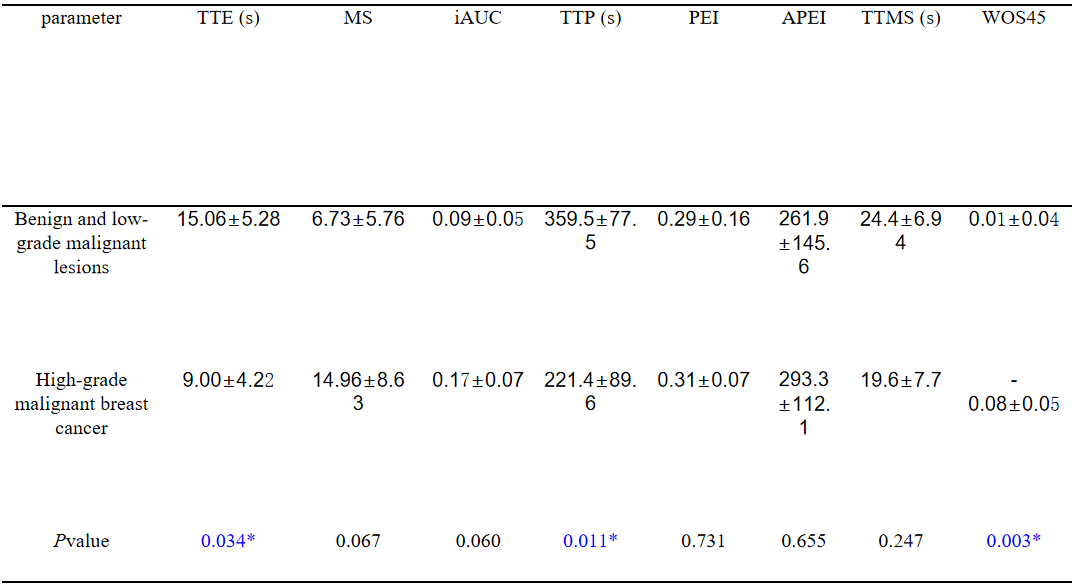
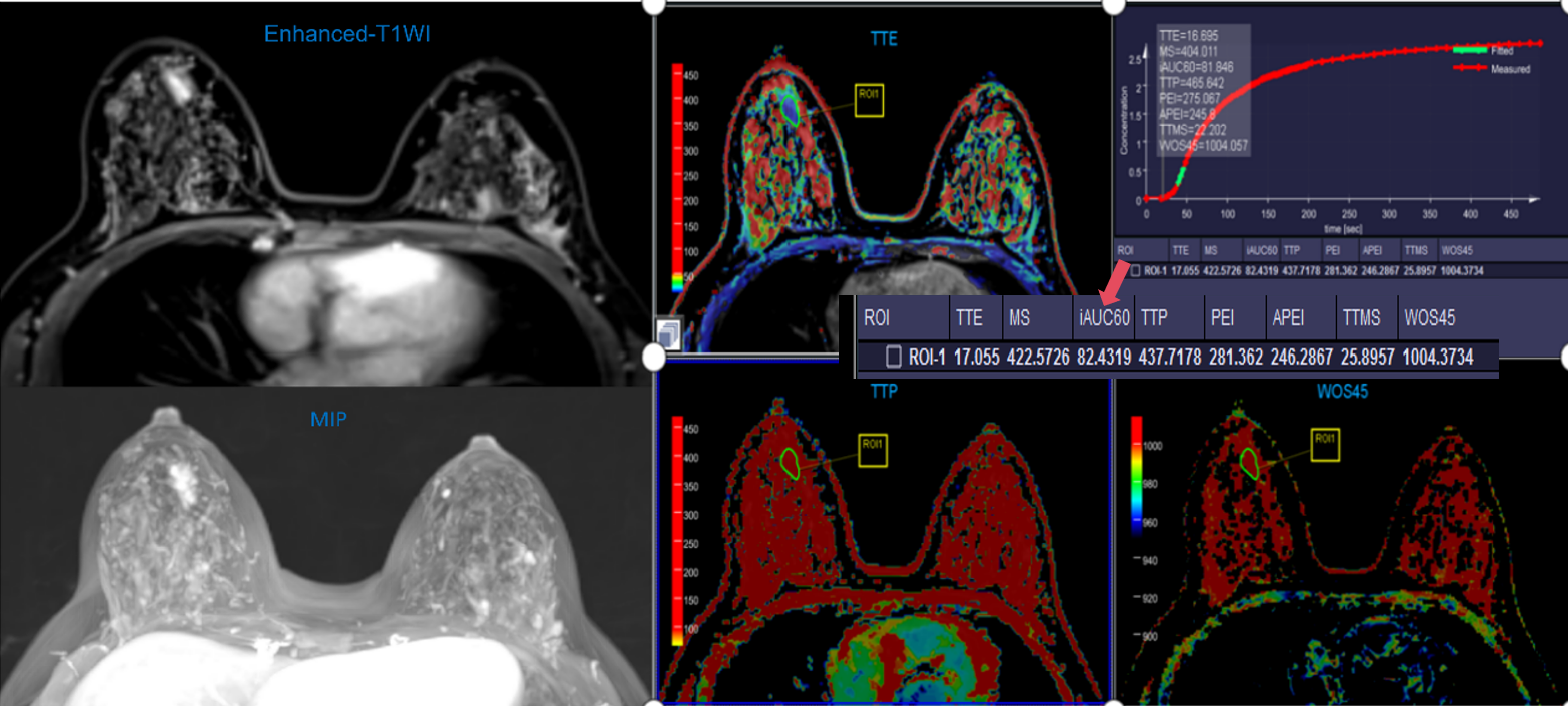
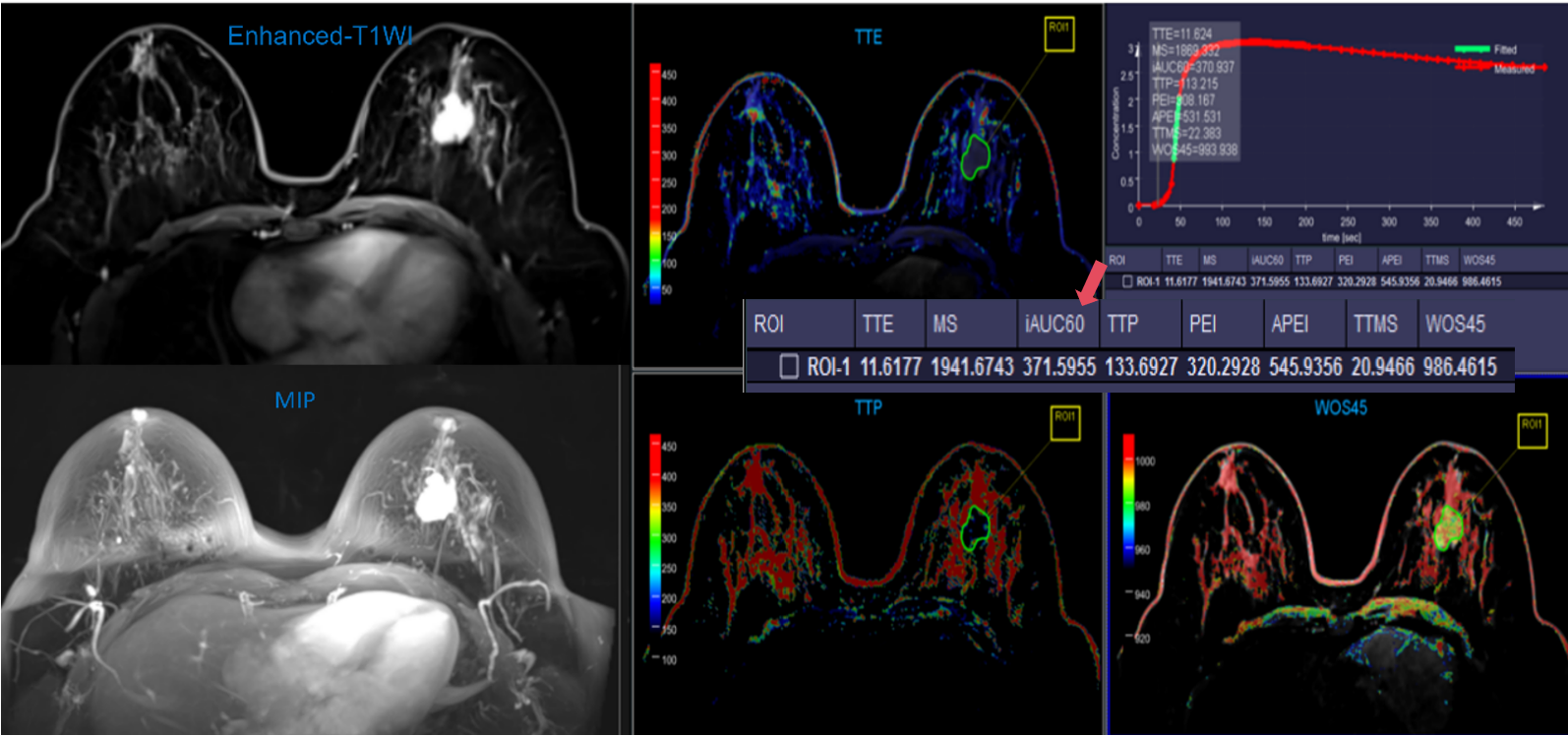
A total of 28 patients were recruited in this study including 6 benign, 8 low-grade malignant breast cancer, and 14 high-grade malignant breast cancer. All patients underwent breast MRI at a 3T MAGNETOM Vida MR scanner (Siemens Healthcare, Erlangen, Germany), before and after the administration of contrast media (0.2 mmol/kg, Gadovist, Bayer) at a rate of 3 mL/s followed by a 10-mL saline chaser. The UF-DCE MRI images were obtained in the axial plane using GRASP in a free-breathing manner, lasting for 8 min and 25 s. The scanning parameters were as follows: variable temporal resolution reconstruction using 12.5 s for the first 20 s, then 3 s, and 12.5 s time resolution again for the last 300 seconds, field of view of 380 mm x 380 mm, matrix of 380 x 320, and voxel size of 1.2 mm x 1.2 mm x 2.5 mm.The new kinetic parameters obtained from UF-DCE MRI (time-to-enhancement (TTE) normalized to arrival in the aorta, maximum slope (MS)), and the conventional semi-quantitative parameters (area under the curve (60 s after enhancement) (iAUC60), time-to-peak after enhancement (TTP), relative peak enhancement (PEI), absolute peak enhancement (APEI), time to center of maximum slope (TTMS), wash-out slope for 45 s after peak, or last 45 s of scan (WOS45)) were calculated by using the breast model of a research software (MR DCE version 1.1.2, Siemens Healthcare, Germany). Statistical analysis was performed using the SPSS software package (SPSS Inc., Chicago, IL, USA). All parameters were expressed as mean ± standard deviation and the P-values < 0.05 were considered statistically significant.Results
The TTE, TTP, and WOS45 values of high-grade malignant tumors were lower than those of the benign and low-grade malignant lesions (P-values of 0.034, 0.011, and 0.003, respectively) (Figures 2, 3), while other indicators were not statistically significant (P > 0.05) (Table 1).Discussion
TTE can reflect how early the lesions begin to enhance. The results showed that the high-grade malignant group has shorter TTE than the benign and low-grade malignant breast tumors (the P-values were 0.034, 0.011, and 0.003, respectively), which demonstrate that the onset time of the lesion enhancement in malignant tumors takes place significantly earlier than that in benign and low-grade malignant group. In the results of Goto et al.3 and Sung et al.4, the median TTE values were 9.9 s and 9.0 s, respectively, which is similar to our results. In addition, it was found that the TTP and WOS 45 indicators of malignant breast cancer were also significantly lower than those of the benign and low-grade malignant groups. According to the literature, this effect could be attributed to the rich neovascularization and increased immature vascular permeability of the invasive tumors. More specifically, the values of the TTE, TTP, and WOS45 parameters are closely related to the degree of neo-microvascularisation of invasive breast cancer, which can increase the speed of the contrast agent entering or leaving the blood vessels5. Natsuko et al. pointed out that compared with the in-situ ductal carcinoma, significantly larger MS and shorter bolus arrival time (BAT) were observed in invasive carcinoma6, while the overall difference of MS in invasive carcinoma in this study was not statistically significant.Conclusion
This preliminary study found that TTE, TTP, and WOS45 of highly malignant cancer lesions were shorter than benign and low-grade malignant lesions, which is of great importance in assisting the clinical differentiation between benign and malignant breast cancer. The UF-DCE MRI technique could be included in breast diagnosis in the future to simplify the MR examination process.Acknowledgements
No acknowledgement found.References
1. RM Mann, N Cho, L Moy. Breast MRI: State of the Art. Radiology. 2019;292(3):520-536.
2. RD Mus, C Borelli, P Bult, et al. Time to enhancement derived from ultrafast breast MRI as a novel parameter to discriminate benign from malignant breast lesions. Eur J Radiol. 2017;89:90-96.
3. BK Szabó, P Aspelin, WM Kristoffersen, et al. Invasive breast cancer: correlation of dynamic MR features with prognostic factors. Eur Radiol. 2003;13(11):2425-35.
4. SU Shin, N Cho, SY Kim, et al. Time-to-enhancement at ultrafast breast DCE-MRI: potential imaging biomarker of tumour aggressiveness. Eur Radiol. 2020;30(7):4058-4068.
5. N Mori, H Abe, S Mugikura et al. Ultrafast dynamic contrastenhanced breast MRI: kinetic curve assessment using empirical mathematical model validated with histological microvessel density. Acad Radiol. 2018;26(7):E141-E149.
6. N Onishi, M Sadinski, MC Hughes, et al. Ultrafast dynamic contrast-enhanced breast MRI may generate prognostic imaging markers of breast cancer. Breast Cancer Res. 2020 28;22(1):58.
Figures