4866
Feasibility and Sensitivity of TRUST Measurements in the Upper Arm1Radiology and Nuclear Medicine, Amsterdam UMC, Amsterdam, Netherlands, 2The Netherlands Cancer Institute, Amsterdam, Netherlands, 3Biomedical Engineering and Physics, Amsterdam UMC, Amsterdam, Netherlands, 4Clinical Haematology, CCA - Cancer Treatment and Quality of Life, Amsterdam University Medical Center, Location University of Amsterdam, Amsterdam, Netherlands
Synopsis
Keywords: Arterial Spin Labelling, Vessels
Motivation: T2-relaxation-under-spin-tagging(TRUST) is a non-invasive MRI technique to estimate blood oxygenation in the superior sagittal sinus from a T2 decay fit.
Goal(s): The calibration curve to convert T2 into oxygenation has been derived with ex-vivo experiments for healthy volunteers and patients with specific types of sickle cell disease.
Approach: Validation of these calibration curves is difficult because blood cannot be drawn from the superior sagittal sinus itself, hampering implementation of the technique in other patient groups.
Results: Here, TRUST was adapted and optimized for the arm so that its measurements of venous oxygenation can be directly compared with venipunctures from the cephalic vein.
Impact: The TRUST-sequence was optimized for non-invasive T2-measurement in the upper arm veins. A posteriori correlation with blood properties returns a venous oxygenation mapping. This may confirm the currently used calibration curve and facilitate obtaining accurate calibration curves for specific diseases.
Introduction
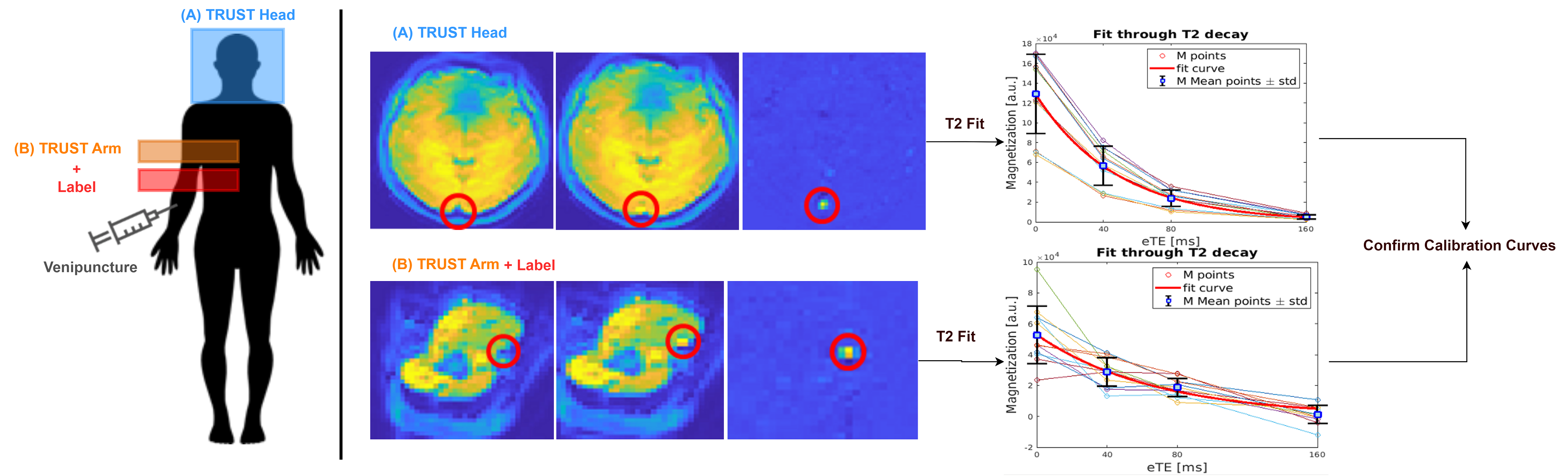
T2-Relaxation-Under-Spin_Tagging (TRUST) is a well established method to measure venous blood oxygenation by estimates of venous blood T2 [1]. The sequence facilitates the isolation of venous blood via a control/label acquisition, and a series of T2-preparation pulses are then used to induce T2-weighting, allowing an exponential fit of the curve.The TRUST-derived T2-constant can then be converted into venous oxygenation using empirical models, which exist for both healthy controls and severe sickle cell disease patients with genetic phenotypes HbSS and HbSβ0[2]. Such models are difficult and expensive to validate because blood cannot directly be drawn from the superior sagittal sinus itself and ex-vivo experiments are complicated by blood coagulation, deoxygenation and changes in temperature. An alternative way to validate these empirical models would be to estimate the venous oxygenation in the antecubital vein using TRUST measurements and then draw blood from this vein and determine its saturation. Here, the TRUST sequence was adapted and optimized to the arm, and subsequently used to determine venous blood T2 in the cephalic vein, providing a method to corroborate the former calibration models and possibly derive new calibrations models in the future.
Methods
The approach presented here is based on the TRUST sequence developed for measuring the blood decay in the sagittal sinus[3]. Label and control images were subtracted and the difference signal at each effective echo time (eTE) was fitted to obtain T2. Given the physiology differences in the venous system in terms of blood flow velocity, vein size, and different T2 values reflecting altering oxygenation, the sequence had to be re-optimized. This study was conducted in healthy volunteers in an attempt to optimize different parameters of the sequence. Eight healthy volunteers(5M:3F, age 28±3 years) were scanned on a 3T Philips Achieva system using a 16-channel small extremity coil.Optimal Post-Labeling Delay (PLD) was determined by comparing a short and long PLD of 250 and 1750 ms to capture slow and fast venous blood flow. The sensitivity of the technique was tested by comparing blood T2 (oxygenation) measured in rest and during a physical challenge (fixed resistance band pulled by the hand until biceps exhaustion). The labeling slab was positioned distally from the imaging slice, thereby abiding to the direction of venous blood flow in the arm. Other imaging parameters were: FOV=220x220cm2, matrix=80x80, labeling gap=30mm, labeling thickness=50mm, NSA=3, slice thickness=0.5mm and effective echo times (eTEs) of 0,40,80 and 160ms, while other parameters were acquired as previously reported [3].
Results
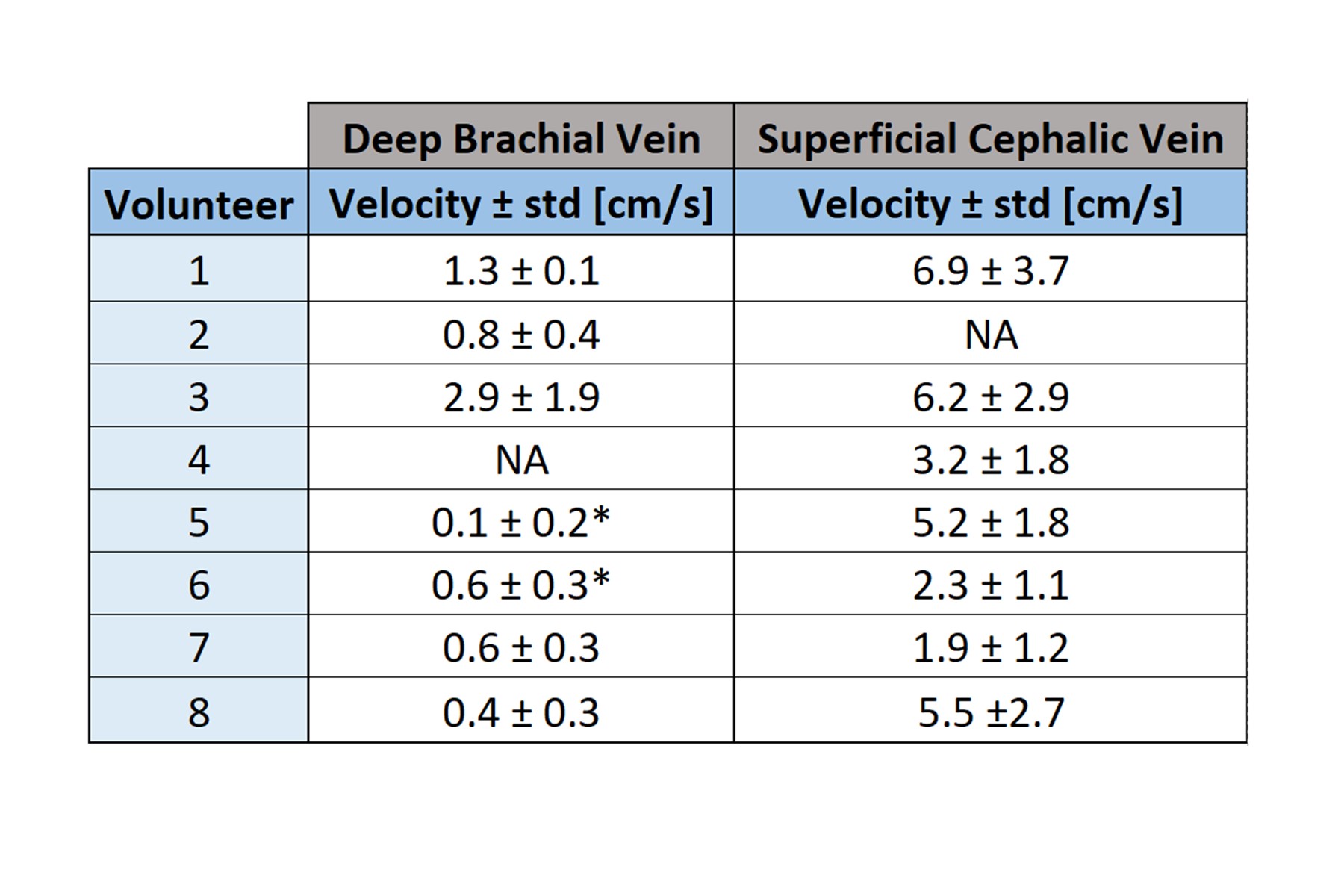
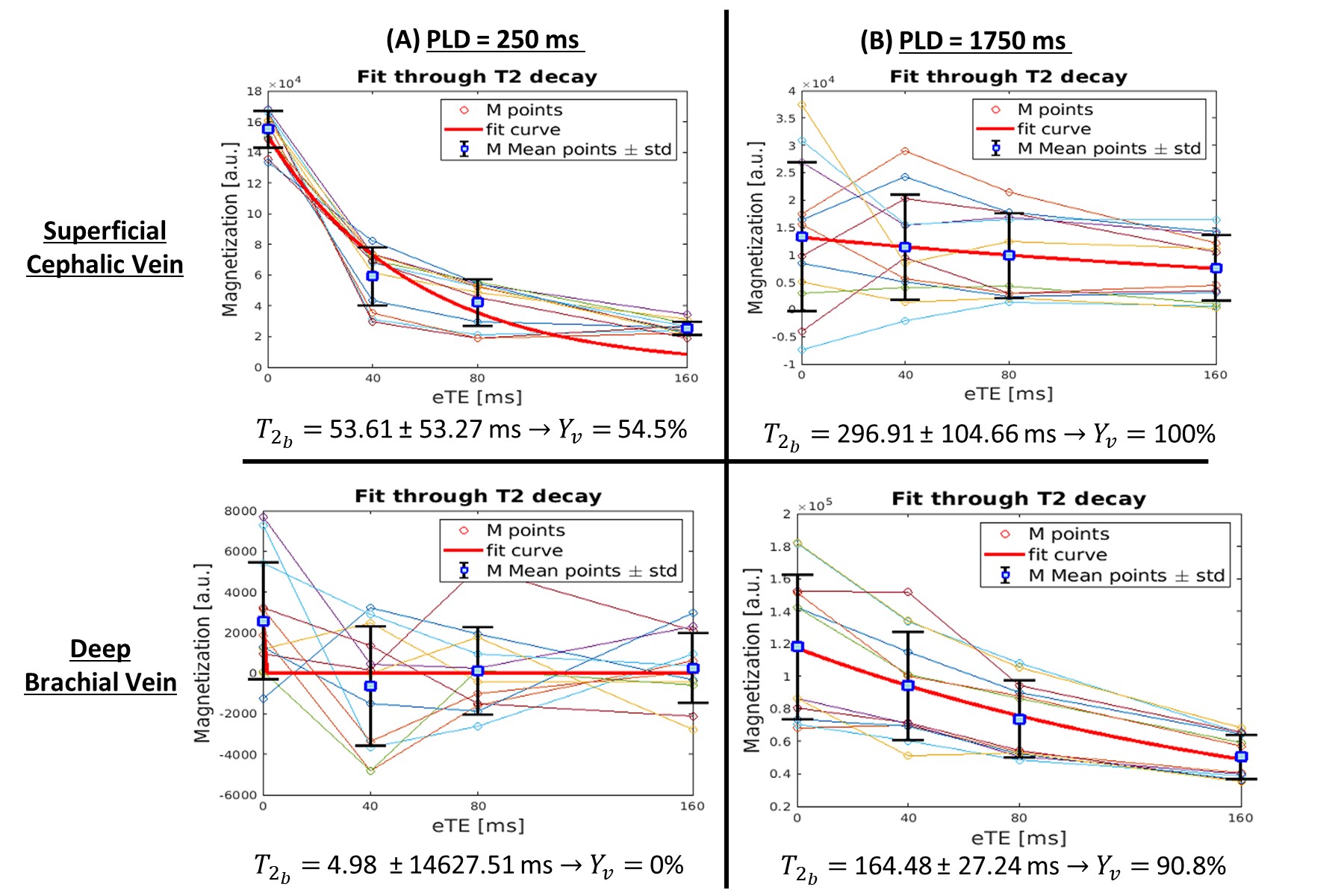
In Table 1, differences in velocities are shown between the main veins in the arm: Deep Brachial Vein (DBV) and Superficial Cephalic Vein (SCV). Overall, DBV has a lower velocity when compared to SCV.Fig.2 shows in a single subject that veins with different blood velocities require different PLDs - a faster blood flow will travel more rapidly to the acquisition plane so a shorter PLD is needed for a good T2 fit (top left, SCV), while a longer PLD reduces the signal difference as well as the fit quality (top right, SCV). On the opposite, veins with a slower flow (DBV, bottom figures) will have both a smaller signal difference and bad quality fit in earlier PLDs (bottom left) while having increased magnetization and quality fit for longer PLDs (bottom right).
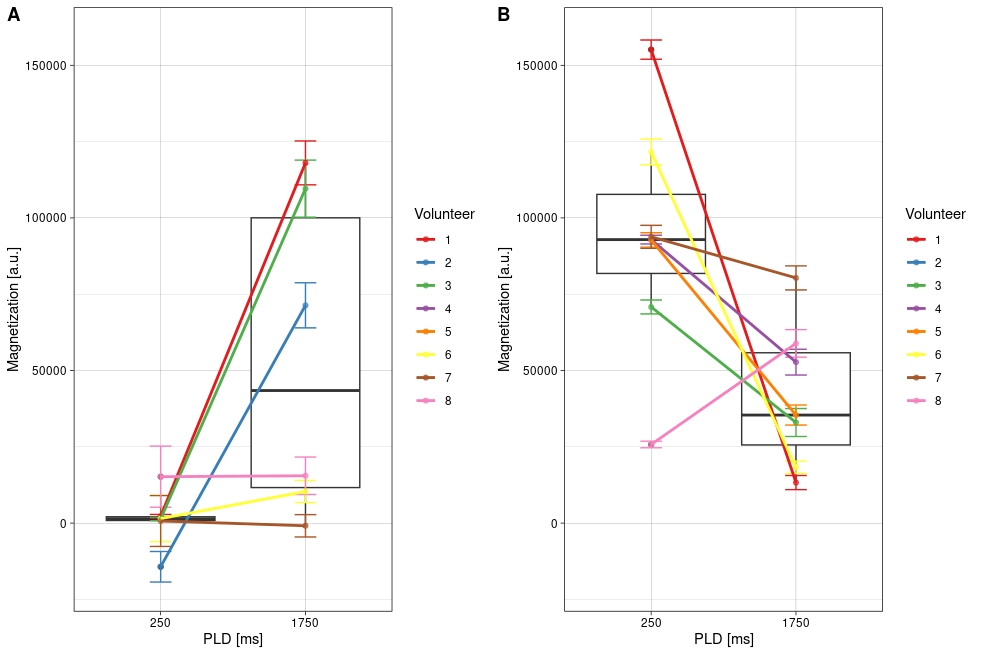
Fig.3 illustrates the mean signal difference for eTE=0ms in all eight volunteers for both PLDs in the observed veins. On average the same behavior can be seen as illustrated in Fig.2 for one single subject: the short PLD is optimal for the SCV, whereas longer PLDs are optimal for measurements in the DBV.
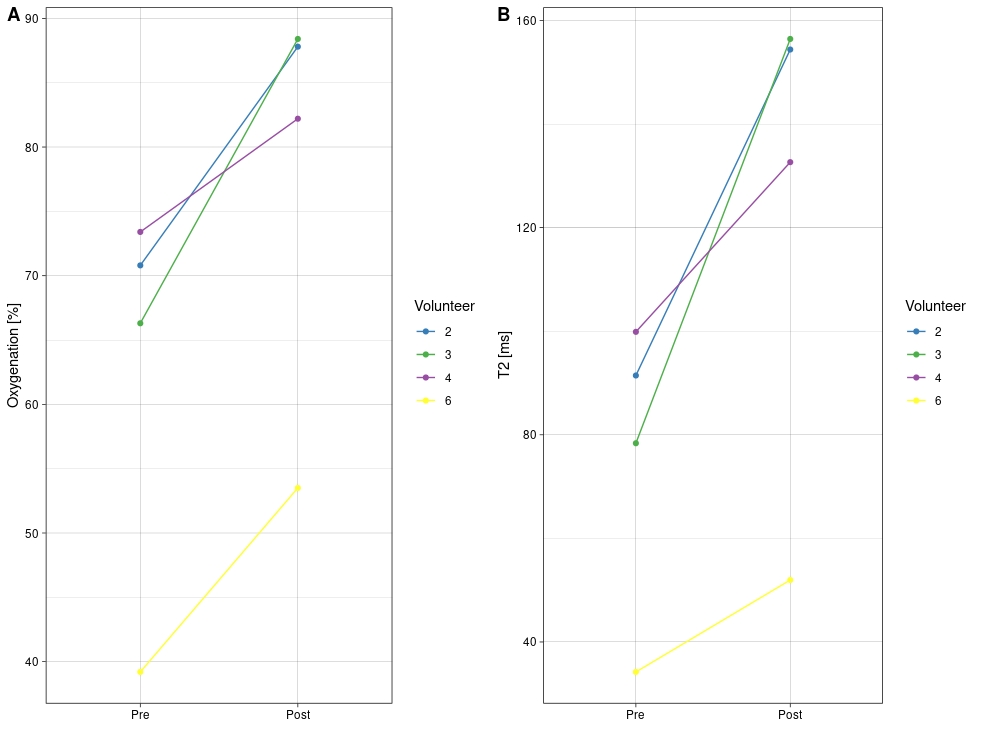
For the physical challenge (Fig.4), we selected four subjects for which there was an increase in signal in the DBV in Fig. 3. The T2b values increased from 76±29ms to 123.0±49ms and oxygenation from 62.4±15.8% to 78.0±15.8% in the DBV. The observed rise in oxygenation level following the biceps exercise challenge was seen in all subjects.
Discussion and conclusion
We showed the feasibility of TRUST in the upper arm together with its sensitivity to a physical challenge. Our data shows that different veins require the use of different PLDs due to differences in blood flow velocity. Although further optimization is required, this technique can potentially be used to validate existing TRUST calibration curves or derive new ones for new patient groups more easily.Acknowledgements
No acknowledgement found.References
[1]H. L. a. Y. Ge, "Quantitative Evaluation of Oxygenation in Venous Vessels Using T2-Relaxation-Under-Spin-Tagging MRI," Magnetic Resonance in Medicine 60:357–363 (2008).
[2] Bush, MRM 2021.
[3]T. D. C. a. J. C. W. Adam M. Bush, "Diminished Cerebral Oxygen Extraction and Metabolic Rate in Sickle Cell Disease Using T2 Relaxation Under Spin Tagging MRI," Magnetic Resonance in Medicine 80:294–303 (2018).
[4]M. S. et al., "Comparison of the Dependence of Blood R2 and R*2 on Oxygen Saturation at 1.5 and 4.7 Tesla," Magnetic Resonance in Medicine 49:47–60 (2003).
[5]Khan et al. “Proof of concept non-invasive estimation of peripheral venous oxygen saturation” BioMed Eng OnLine (2017)[6] Bishop et al. “THE BLOOD FLOW IN THE HUMAN ARM DURING SUPINE LEG EXERCISE”, J. Physiol. (I957) I37, 294-308
Figures