4858
Automated Bladder Segmentation of 3D Dynamic MRI For Urodynamic Analysis Using Deep Learning1University of Wisconsin-Madison, Madison, WI, United States
Synopsis
Keywords: Analysis/Processing, Machine Learning/Artificial Intelligence, Segmentation, Urodynamics
Motivation: Bladder dysfunction is assessed using catheterization which are invasive and provides insufficient biomechanical information. MRI urodynamics is tedious because segmentation of bladders over numerous time steps during voiding.
Goal(s): Implement automated segmentation using deep learning for accelerating the workflow of MRI-based urodynamic assessment.
Approach: Train a U-Net using 3D dynamic images and manually segmented masks. Use time and dice score to assess the performance of the network.
Results: Images of bladder voiding from five subjects were used to train the network and can segment one bladder in <3 minutes, compared to 20 minutes for manual segmentation. Dice score was 0.99 showing excellent performance.
Impact: Urodynamic assessment using MRI is a tedious process due to segmentation of the bladder from 3D dynamic image datasets. We automated segmentation using deep learning to accelerate the workflow. Our automated process reduced time sixfold and produces excellent segmentation.
Introduction
Bladder dysfunction is common among aging men due to benign prostatic hyperplasia (BPH) and lower urinary tract symptoms (LUTS)1,2. Multichannel urodynamic studies (UDS) is the most common diagnostic method used to assess BPH/LUTS3,4. These procedures are invasive requiring urethral and rectal catheterization, and provide insufficient biomechanical information5,6. Our laboratory recently published the feasibility of using 3D dynamic MRI to calculate various urodynamic nomograms non-invasively7. Manually segmenting the bladder is a tedious step and is a bottleneck for increasing the study cohort. The purpose of this study is to implement a deep learning approach that automatically segments the bladder from 3D dynamic images of voiding. This will significantly accelerate our MRI urodynamic workflow.Methods
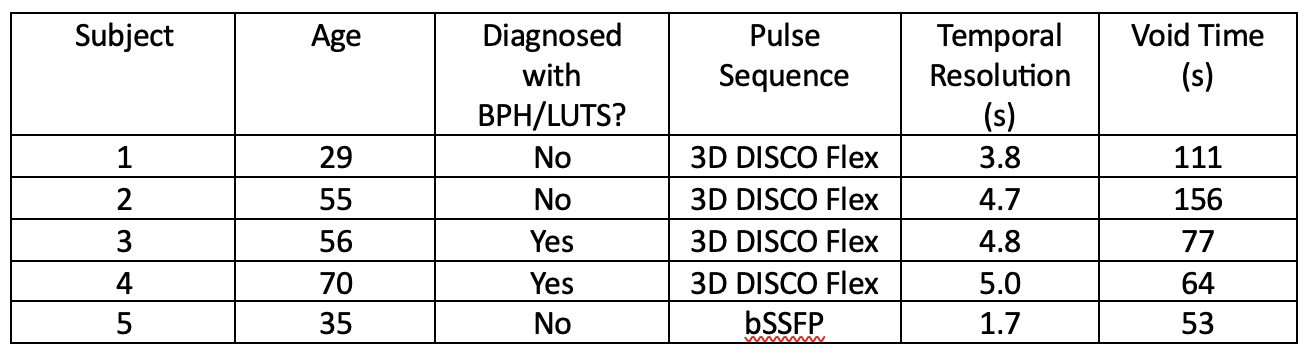
Male subjects were recruited following an IRB-approved HIPAA-compliant protocol. Subjects underwent pelvic MRI on a clinical 3T scanner (Premier, GE Healthcare, Waukesha, WI, USA). The pulse sequence was either 3D Differential Subsampling with Cartesian Ordering (DISCO) Flex for which patients received 1/3 of a single weight-based dose (0.1 mmol/kg) of gadolinium-based contrast which was slowly hand injected intravenously 15 minutes prior to the start of the imaging session, or balanced steady state free precession (bSSFP) that did not require contrast. Subjects that received contrast were asked to walk around to ensure contrast mixing and homogeneous enhancement of the urine in the bladder. Immediately before the scan, the subjects were equipped with a condom catheter to allow micturition and urine collection while scanning. Subjects were scanned in supine position and volumetric dynamic images of the bladder and urethra were acquired throughout the voiding event. The 3D image datasets were loaded into semiautomatic segmentation software packages Mimics (Materialise NV, Leuven, Belgium). The bladder was manually segmented such that there were separate 3D masks at each time point of the voiding event. These manually segmented masks served as the ground truth. The U-Net8 convolutional neural network (CNN) was used to analyze the images and automatically detect the bladder geometry and generate a binary mask. All images have 256x256 pixels and 112-152 sagittal layers. This spatial anisotropy required us to filter the 2D images through the CNN. The procedure was implemented using PyTorch (The Linux Foundation, San Francisco, CA, USA) inside a Docker9 container. All training and testing were performed on an Intel Core i7-9800X processor and Nvidia Titan RTX GPU. Dice score was used to compare manual and automated segmentations.Results
Five subjects underwent pelvic MR scans and 3D dynamic images were successfully acquired while they voided during scanning. Table 1 provides subject and scan information. Figure 1 visualizes the bladder voiding for all five subjects. Subject 5’s images exhibited significant artifact due to eddy currents that led to poor image quality. A total of 6366 2D sagittal images from 3D dynamic images were used: 5730 for training and 636 for validation of the CNN. The Dice score was 0.99, and total training time was 13 minutes. Time to manually segment one 3D bladder at one time point was 20 minutes, compared to < 3 minutes using the automated approach. Figure 2 shows the manual and automated segmentation during voiding, for Subject 1 as an example, as well as the difference image.Discussion
Using 3D dynamic MRI of only five patients, we implemented a deep learning-based automated segmentation of bladder during voiding. The main findings of the study are the CNN segments a 3D bladder at one time point in < 3 minutes, produces excellent segmentation, and performs well over a range of subject ages, phenotypes and two different sequences. Figure 2 shows that the difference in segmentations is about 1-2 pixel wide around the bladder wall, which is in the range of spatial resolution. We chose the U-Net architecture due to its popularity in the image segmentation field10–12. We also prioritized portability of the CNN by using a container which will allow easier scaling to high-performance computing clusters and sharing with the scientific community. The segmented masks can be used to calculate urodynamic metrics including flow rate, post-void residual volume, and bladder neck angle. Future studies would investigate spatio-temporal interconnectivity of the images, increase the number of subjects, explore the effects of interobserver variability and scan parameters, and compare the urodynamic metrics from manual segmentation with automated.Conclusion
We previously introduced MRI urodynamics using 3D dynamic imaging to enhance information from UDS while being non-invasive. Segmentation is the most tedious step in our workflow, and this automated process significantly reduces operator time. This acceleration in the workflow paves the path for MRI urodynamics to increase cohort size and provide urodynamic nomograms faster.Acknowledgements
NIH R01 DK126850-01A1 and Wisconsin Partnership Program WPP; AAM3497
GE Healthcare which provides research support to the University of Wisconsin-Madison.
References
1. Roehrborn CG. Benign Prostatic Hyperplasia: An Overview. Rev Urol. 2005;7(Suppl 9):S3. Accessed November 3, 2021. /pmc/articles/PMC1477638/
2. Thorpe A, Neal D. Benign prostatic hyperplasia. In: Lancet. Vol 361. Elsevier; 2003:1359-1367. doi:10.1016/S0140-6736(03)13073-5
3. Nitti VW. Pressure Flow Urodynamic Studies: The Gold Standard for Diagnosing Bladder Outlet Obstruction. Rev Urol. 2005;7(Suppl 6):S14. Accessed December 1, 2022. /pmc/articles/PMC1477621/
4. Blaivas J. Multichannel urodynamic studies. Urology. 1984;23(5):421-438. doi:10.1016/S0090-4295(84)80005-9
5. Bushman W. Etiology, Epidemiology, and Natural History. Urologic Clinics of North America. 2009;36(4):403-415. doi:10.1016/j.ucl.2009.07.003
6. Pewowaruk R, Rutkowski D, Hernando D, Kumapayi BB, Bushman W, Roldán-Alzate A. A pilot study of bladder voiding with real-time MRI and computational fluid dynamics. PLoS One. 2020;15(11 November):e0238404. doi:10.1371/journal.pone.0238404
7. Gonzalez-Pereira JP, Johnson CJ, Wells S, Bushman W, Roldan-Alzate A. Technical feasibility of uro-dynamic MRI study of voiding biomechanics: a pilot study. Int Urol Nephrol. Published online October 12, 2023:1-7. doi:10.1007/S11255-023-03823-7/FIGURES/8
8. Ronneberger O, Fischer P, Brox T. U-net: Convolutional networks for biomedical image segmentation. Lecture Notes in Computer Science (including subseries Lecture Notes in Artificial Intelligence and Lecture Notes in Bioinformatics). 2015;9351:234-241. doi:10.1007/978-3-319-24574-4_28/COVER
9. MerkelDirk. Docker. Linux Journal. Published online March 1, 2014. doi:10.5555/2600239.2600241
10. Berhane H, Scott M, Elbaz M, et al. Fully automated 3D aortic segmentation of 4D flow MRI for hemodynamic analysis using deep learning. Magn Reson Med. 2020;84(4):2204-2218. doi:10.1002/mrm.28257
11. Bustamante M, Petersson S, Eriksson J, et al. Atlas-based analysis of 4D flow CMR: automated vessel segmentation and flow quantification. J Cardiovasc Magn Reson. 2015;17(1). doi:10.1186/S12968-015-0190-5
12. Herment A, Kachenoura N, Lefort M, et al. Automated segmentation of the aorta from phase contrast MR images: Validation against expert tracing in healthy volunteers and in patients with a dilated aorta. Journal of Magnetic Resonance Imaging. 2010;31(4):881-888. doi:10.1002/JMRI.22124
Figures