4856
A Two Step Workflow to Support Fully Autonomous MR Scanning in Prostate1GE Healthcare, Waukesha, WI, United States, 2GE Healthcare, Bengaluru, India, 3GE Healthcare, Niskayuna, NY, United States
Synopsis
Keywords: Other AI/ML, Machine Learning/Artificial Intelligence
Motivation: A fully automatic workflow for scan plane prescription is desirable in clinical settings.
Goal(s): Our goal is to demonstrate a deep learning-based MRI scan workflow for fully automated MR scanning in the prostate.
Approach: This new scan workflow will identify anatomical landmarks and scan planes for prostate planning (coverage, FOV and orientation) from coil sensitivity and 3plane scout images.
Results: The deep learning-based anatomy recognition showed acceptable average location error below 5mm and plane orientation error below 10 degrees.
Impact: As no interaction from the operator is required to complete a full MR prostate scan, it paves the way for fully automated MR scans for the prostate anatomy.
INTRODUCTION
MRI is inherently a multi-planar imaging modality. An automatic workflow for scan plane prescription of different landmarks and anatomies is desirable in clinical settings to reduce MRI exam time and improve image consistency, especially in longitudinal studies. Previously, it was demonstrated that intelligent slice placement (ISP) for multiple landmarks in the brain and knee is possible using a deep learning-based framework based on standard 2D tri-planar localizer images [1-3]. However, the scout images are setup manually in blinded manner and ISP algorithm must accommodate variability in scout placements for robust performance. Sometimes the scout images are repeated due to insufficient anatomical coverage. Previously, it was also demonstrated that the coil sensitivity maps can be used to automatically find the region of interest of spine anatomy to correctly position the volume for the 3plane scout scan, typically the first scan for any patient scan planning [4].In this work, we demonstrate a generalized, deep learning (DL)-based framework for a fully automated MRI scan workflow for the prostate anatomy. It consists of automated volume prescription for the 3plane scout scan using CalLocNet model based on the 3D coil sensitivity scan to identify the prostate location from the coil sensitivity map volume. After the 3plane scout scan is acquired, multiple deep neural networks (ScanNets) will identify the anatomical structures around the prostate in the scout volume, which include apex and base of the prostate, rectum, pubis, seminal vesicles, L5 and S1, left and right hip, prostate, and urethra. All the above information can then be used to prescribe the imaging volume center, field of view, slice coverage and volume orientation for acquiring the high-resolution prostate MR scans automatically.
METHODS
Data: Cohort A. 66 coil sensitivity maps and 3plane scout images of volunteers were collected for the CalLocNet. Cohort B. 741 volume of patients from different hospitals were collected and used for training and evaluation of ScanNets models. In all training and evaluation testing, 80% of data were used for training, 10% for validation and 10% for testing.Models: The fully automated workflow is supported by 5 deep learning models (based on architecture for segmentation [6]) as described below:
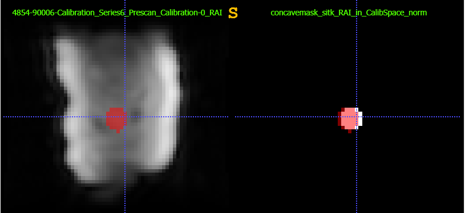
1) CalLocNet: Identifies the prostate location from the coil sensitivity map volume. The prostate location is then used to determine the volume for 3plane scout scan.
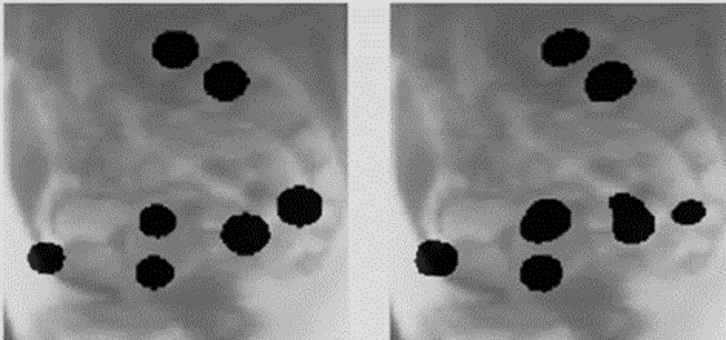
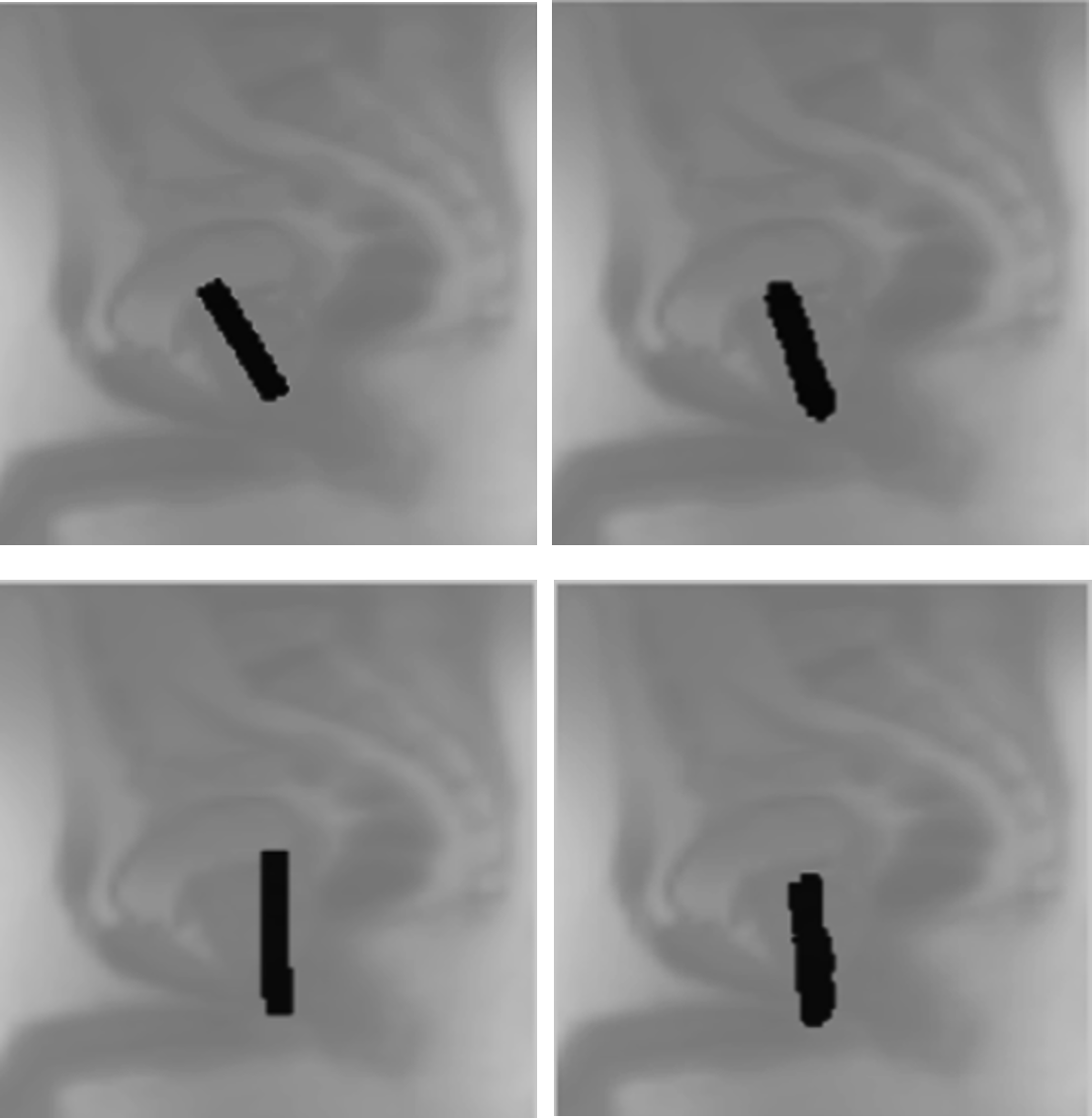
2) ScanNets: Four models to Identify specific anatomy locations and volumes around the prostate region. The first model (3D SagLocNet) identifies apex and base of prostate, L5, S1, pubis, rectum, seminal vesicle. The second (3D CorLocnet) identifies left and right hip, the third one (2D ProstateSeg) identifies prostate mask and the fourth model (3D Oblique PlaneNet) identifies oblique planes aligned with prostate apex and base, and urethra.
Labels: All anatomical locations and masks were manually labeled on the 3-plane scout volume, except prostate and urethra were labeled on the high resolution sagittal T2 volume, and then resampled on the 3plane scout volume.
Augmentation: All or part of the augmentation techniques were implemented to improve model performance: intensity augmentation, noise corruption, adaptive histogram equalization, median filter, volume translation, rotation and cropping, z-score normalization etc.
DL Methodology: DL segmentation networks were adapted for all the five models [5-7].
Accuracy Assessment: For CalLocNet model, dice score was used as accuracy metric. For all ScanNets, accuracy was assessed by calculating location from a segmentation mask and then the location error was evaluated between GT and DL prediction. For predicted planes for prostate apex/base and urethra, angle error between GT and DL-predicted planes was calculated.
RESULTS AND DISCUSSION
For CalLocNet, the testing DICE score is 84.21%. For all ScanNets, the average location error is less than 5mm, and angle error is less than 10 degrees. Fig. 1 shows an example of predicted prostate mask vs ground truth prostate mask for the CalLocNet. Fig. 2 shows an example of predicted 7 locations from SagLocNet on the right comparing with ground truth locations on the left. Table 1 presents the average location error on the validation and testing datasets for the SagLocNet. Fig. 3 shows an example of predicted prostate apex/base plane and urethra plane comparing to ground truth. Table 2 presents the average angle error on the validation and testing datasets for the ObqliuePlaneNet.CONCLUSION
We introduced a fully automated MR scanning workflow starting from a large FOV coil sensitivity volume scan. Results indicate very high accuracy for volume prescription for all prostate scans including 3plane scout scan. The generalized fully automated workflow can be extended to other anatomies as well.Acknowledgements
No acknowledgement found.References
- Liu Y, Dawant BM. “Automatic localization of the anterior commissure, posterior commissure, and midsagittal plane in MRI scans using regression forests”. IEEE J Biomed Health Inform. 2015;19(4):1362-74.
- Wieslaw L. Nowinski et.al., “Rapid and automatic calculation of the midsagittal plane in magnetic resonance diffusion and perfusion images”, Acad Radiol. 2006 May; 13(5): 652–663.
- Bhushan, Chitresh & Shanbhag, Dattesh & Maximo, Andre & Sreekumari, Arathi & Gui, Dawei & Patil, Uday & Pascual, Brandon & Mullick, Rakesh & Yeo, Desmond & Foo, Thomas. “Intelligent Knee MRI slice placement by adapting a generalized deep learning framework”. Proceedings of ISMRM 2020
- K Manickam, M Shao, D Gui, C Bhushan, Dattesh D Shanbhag. “Intelligent automatic slice prescription of scout scans of MSK MRI imaging using surface coil sensitivities.” Proceedings of ISMRM 2023
- Deep Anand et.al., “Realizing a robust multi-task training strategy with deep learning: application in Spine MR image quality assessment”, Proceedings of ISMRM 2023, p. 2950.
- Olaf Ronneberger, Philipp Fischer, Thomas Brox, “U-Net: Convolutional Networks for Biomedical Image Segmentation”, Medical Image Computing and Computer-Assisted Intervention (MICCAI), Springer, LNCS, Vol.9351: 234--241, 2015
Figures