4852
An appropriate threshold for LGE images using deep learning-based reconstruction in revelation clinically unrecognized myocardial infarction1GE Healthcare, MR Research China, Beijing, China, 2Department of radiology, Renmin Hospital Wuhan University, Wuhan, China
Synopsis
Keywords: AI/ML Image Reconstruction, Cardiovascular
Motivation: To precisely screen out infarction in patients with unrecognized myocardial infarction (UMI) in hope of early intervention to reduce adverse cardiac events.
Goal(s): To evaluate deep learning reconstruction based late gadolinium enhancement (LGEDL) in comparison with conventional reconstructed LGE (LGEO) and also to explore an appropriate threshold method for LGE measurements.
Approach: LGEDL and LGEO of 77 patients diagnosed with UMI were evaluated for image quality and analyzed for MI areas using different standard deviation thresholds and a full-width-half-height (FWHM) method.
Results: The STRM ≥ 4SD and ≥ 3SD is respectively reckoned as the best reference threshold for LGEDL and LGEO.
Impact: The deep-learning based reconstruction LGE images had better image quality and reliable pathological evidences for detection of UMI. Significantly different Parea using threshold techniques for LGEDL and LGEO indicated the utility of STRM should be concerned.
INTRODUCTION
Unrecognized myocardial infarction (UMI) is challenging to be found and has a worse prognosis than recognized myocardial infarction (RMI) due to atypical symptoms and delayed treatments[1]. Cardiomyocytes lack the ability to regenerate, making myocardial cell necrosis permanent[2]. Late gadolinium enhancement (LGE) is commonly used but may have limitations in detecting UMI. Deep learning (DL) can elevate image quality and reduce variability, improving diagnosis and treatment accuracy[3]. A convolutional neural network transformer (CNNT) reduces motion artifacts, and DL reconstruction (DLR) algorithms improve image quality[4]. This study aimed to investigate the consistency of UMI detection rates between conventional and DLR LGE images (LGEO and LGEDL) and also explored the selection of quantification methods using different thresholds and the full width at half maximum (FWHM) method for LGEO and LGEDL.METHODS
This study was approved by our hospital (Approval No. 2022K-K083), and 98 suspected UMI patients who visited the hospital between April 2022 and February 2023 underwent cardiac MRI scans including a LGE sequence using deep-learning reconstruction (LGEDL) and conventional reconstruction (LGEO) on a 3.0 T MRI scanner with the following parameters: TE 2.7ms, flip angle 25°, field of view = 34 cm ×34 cm, matrix size = 260 × 174, slice thickness = 8 mm, gap = 2 cm, bandwidth = 83.33kHz, echo train length = 24, number of excitation = 1, theoretical acquisition time = 8 s × 9 heartbeats. Fifteen minutes ahead of scanning the LGE sequences, gabexidine glucosamine injection (Modic, Shanghai Boris Pharmaceutical Co., Ltd.) was administered at 0.1 mmol/kg body weight at a flow rate of 3.5 ml/s and an equivalent amount of saline at the same flow rate. Quantitative analysis and diagnostic efficacy of the LGEDL and LGEO were assessed.All data were statistically analyzed using R-project (version 4.0.4, http://www.r-project.org). Quantitative data were expressed as x±s or median (25th percentile, 75th percentile). All quantitative data were respectively examined by Wilcoxon signed rank test or paired t test according to normal distribution and variance equality assessed by Shapiro-Wilk test and Levene test. The objective quantitative indicators (SNRO, SNRDL, CNRO, CNRDL, SDO, SDDL, Parea-O and Parea-DL) were evaluated using the intraclass correlation coefficient (ICC) to assess intra- and inter- observer agreements. Parea-DL and Parea-O were assessed by different threshold methods to plot the receiver operator characteristic curve (ROC) and compare the difference in diagnostic efficacy of Parea-DL and Parea-O for UMI or non-UMI groups by area under curve (AUC). P<0.05 was considered statistical difference.RESULTS
Based on clinical indicators and previous reports, 77 patients were diagnosed with UMI. A total of 61 patients were studied (43 males, and 18 females, mean age: 55.9 years ± 8.7) (Fig. 1). SNRDL and CNRDL was 2 times more higher than SNRO and CNRO (p<0.001). SDDL of noise was significantly decreased compared to SDO (all P < 0.001) (Fig. 2). Parea-DL elevated compared to Parea-O sequences using threshold methods (P < 0.001) but not FWHM method (p = 0.194) while Parea-DL and Parea-O except between 2SD and 3SD as well as Parea-O between 4SD/5SD and FWHM were significantly different (P < 0.001) (Table 1). Good intra- and inter-group agreement for SNR, CNR, SD, and Parea (ICC > 0.700, all P < 0.001). ROC curves showed each SD method exhibited good diagnostic efficacy for UMI especially the best diagnostic efficacy of 5SD Parea-DL (AUC=0.891, 95% CI 0.781-0.999, p<0.001) (Fig. 3).DISCUSSION
Presence of infarction in patients with Unrecognized Myocardial Infarction (UMI) is crucial for predicting adverse cardiac events[5]. The enhancement area on LGE images (Parea) serves as an indicator of irreversible tissue damage and helps assess the effectiveness of cardioprotective interventions[6,7]. Deep learning-based LGE reconstruction (LGEDL) produces images with lower noise and clearer boundaries, resulting in improved inter- and intra- consistency in Parea measurements[8]. Parea varies for threshold selection; 4SD threshold showed the highest consistency and reliability, especially for LGEDL images. Parea were consistent between LGEO and LGEDL images using FWHM.CONCLUSION
Overall, LGEDL showed higher diagnostic accuracy of UMI than LGEO. A 4SD threshold for Parea is suggested for more reliable UMI diagnosis, although the 5SD threshold also offers good diagnostic efficacy. Importantly, the detection rate of UMI was the same between LGEO and LGEDL despite higher image quality and reliability for the latter.Acknowledgements
None.References
[1] Weir-McCall JR, Fitzgerald K, Papagiorcopulo CJ, et al. Prevalence of unrecognized myocardial infarction in a low–intermediate risk asymptomatic cohort and its relation to systemic atherosclerosis. Eur Heart J Cardiovasc Imaging 2017;18(1): 657–662.
[2] Kim C, Park CH, Kim DY, et al. Semi-Quantitative Scoring of Late Gadolinium Enhancement of the Left Ventricle in Patients with Ischemic Cardiomyopathy: Improving Interobserver Reliability and Agreement Using Consensus Guidance from the Asian Society of Cardiovascular Imaging-Practical Tutorial (ASCI-PT) 2020. Korean J Radiol 2022;23(3):298-307.
[3] Zucker EJ, Sandino CM, Kino A, Lai P, Vasanawala SS. Free-breathing Accelerated Cardiac MRI Using Deep Learning: Validation in Children and Young Adults. Radiology 2021; 300(3):539-548.
[4] Xue H, Rehman A, Davies RH, Moon JC, Fontana M , Kellman P. CNNT DB-LGE: free-breathing dark blood late enhancement imaging using the convolutional neural network transformer speeds acquisition by 50%. Eur Heart J Cardiovasc Imaging 2022;23(Suppl 2): ii11-ii12.
[5] Halliday BP, Baksi AJ, Gulati A, et al. Outcome in dilated cardiomyopathy related to the extent, location, and pattern of late gadolinium enhancement. JACC Cardiovasc Imaging 2019;12(6):1645-1655.
[6] Stone GW, Selker HP, Thiele H, et al. Relationship between infarct size and outcomes following primary PCI: Patient-level analysis from 10 randomized trials. J Am Coll Cardiol 2016; 67(14): 1674-1683.
[7] Taylor AM. The role of artificial intelligence in paediatric cardiovascular magnetic resonance imaging. Pediatr Radiol 2021;22(1):1-8.
[8] Toupin A, Pezel T, Bustin A, Cochet H. Whole-Heart High-Resolution Late Gadolinium Enhancement: Techniques and Clinical Applications. J Magn Reson Imaging 2022;55(4):967-987.
Figures
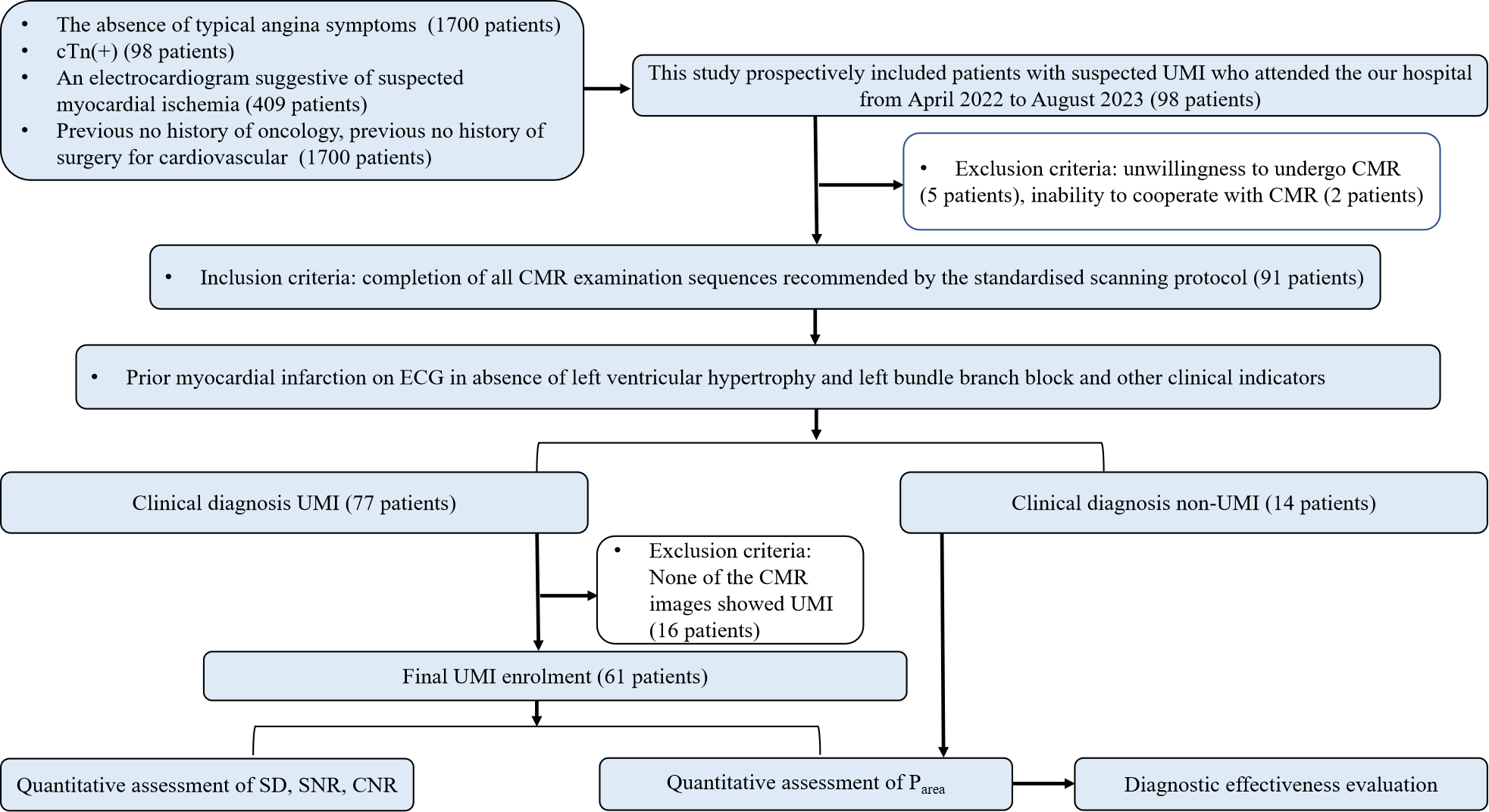
Figure 1: The flowchart of patient enrollment and exclusion.
Note: cTn: cardiac troponin; ECG: electrocardiogram; LGEO:conventionally constructed late gadolinium enhancement;LGEDL:deep-learning based reconstruction late gadolinium enhancement; SD:standard deviation,;SNR:signal to noise ratio;CNR: contrast to noise ratio
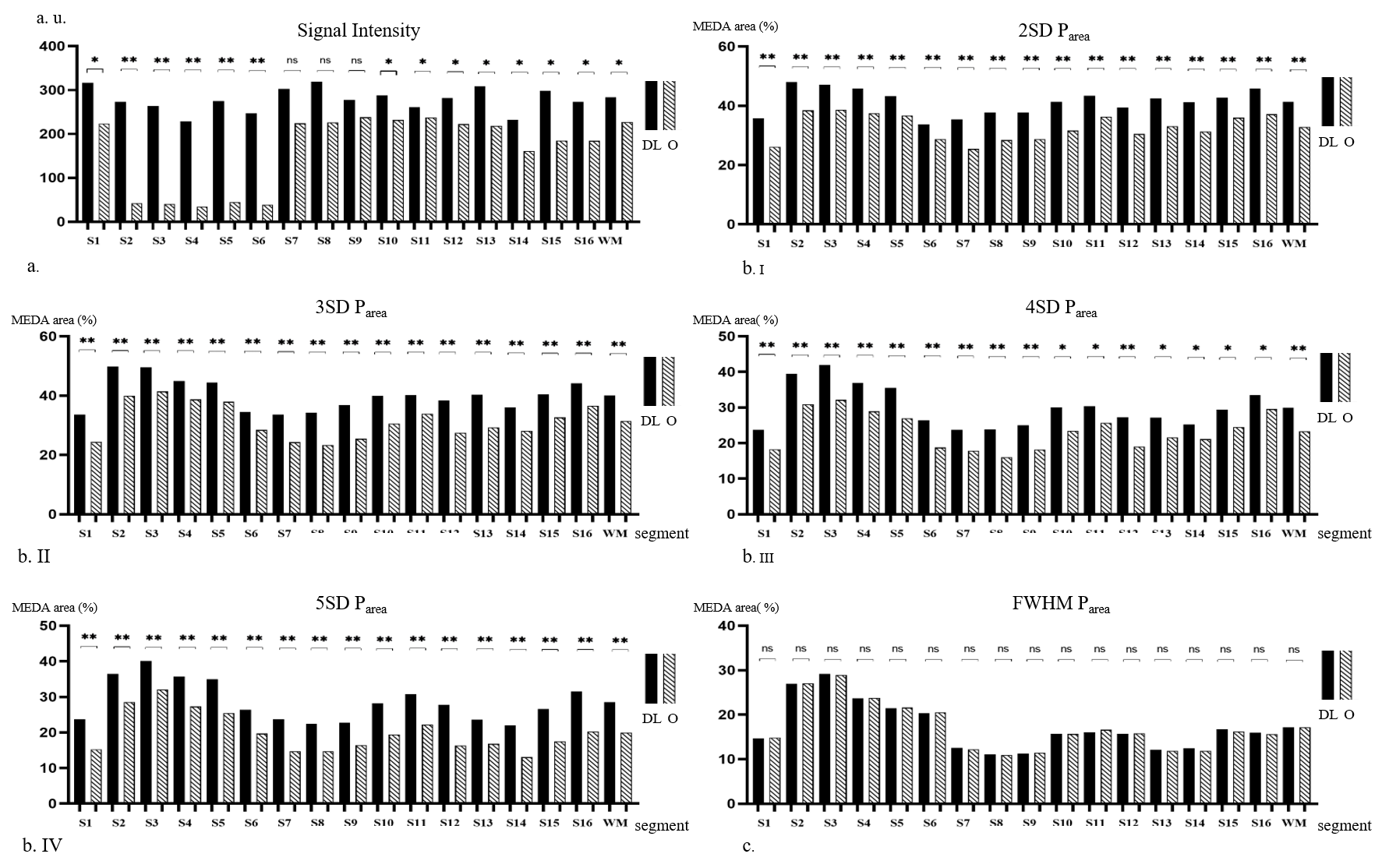
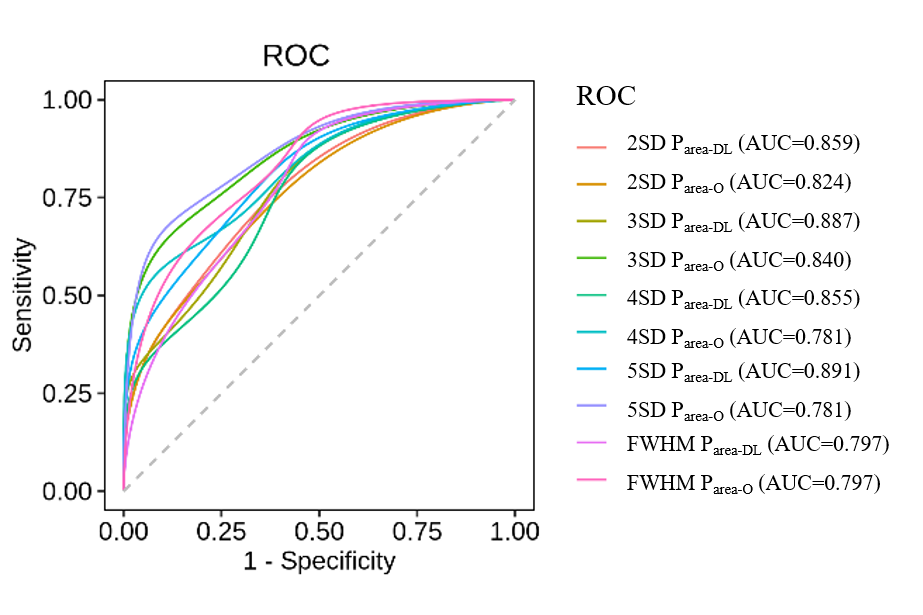
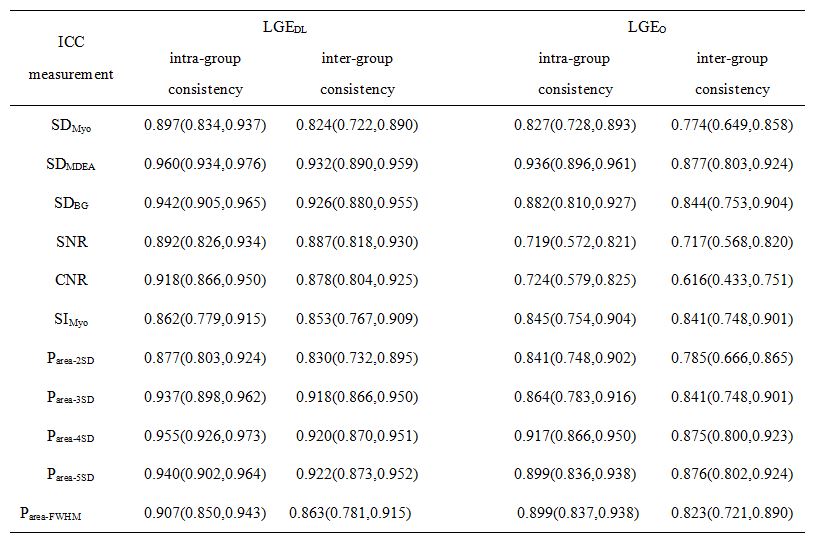
Table1. Consistency of quantitative measurements.
Note: Values in the table are consistency values (95% Confidence Interval)